
Abstract
Purpose:
This study evaluated postoperative complications of percutaneous nephrolithotomy (PCNL) and the influence of selected factors on the risk of complications using the Clinical Research Office of the Endourological Society (CROES) PCNL Global Study database.
Patients and Methods:
The CROES PCNL Global Study collected prospective data for consecutive patients who were treated with PCNL at centers around the world for 1 year. Complications were evaluated by the modified Clavien classification system.
Results:
Of 5724 patients with Clavien scores, 1175 (20.5%) patients experienced one or more complications. The most frequent complications were fever and bleeding. Urinary leakage, hydrothorax, hematuria, urinary tract infection, pelvic perforation, and urinary fistula also occurred in ≥20 patients in each group. The majority of complications (n=634, 54.0%) were classified as Clavien grade I. Two patients died in the postoperative period. The largest absolute increases in mean Clavien score were associated with American Society of Anesthesiologists (ASA) physical status classification IV (0.75) or III (0.34), anticoagulant medication use (0.29), positive microbiologic culture from urine (0.24), and the presence of concurrent cardiovascular disease (0.15). Multivariate regression analysis revealed that operative time and ASA score were significant predictors of higher mean Clavien scores.
Conclusion:
The majority of complications after PCNL are minor. Longer operative time and higher ASA scores are associated with the risk of more severe postoperative complications in PCNL.
Introduction
Recent studies have extended the use of the modified Clavien classification system to the assessment of outcomes of percutaneous nephrolithotomy (PCNL). 12 –14 It is unclear, however, whether the modified Clavien grading system is valid for evaluation of all urologic procedures and whether the classification system can provide valid audit, thereby allowing comparison between hospitals and individual surgeons on the outcome for a particular procedure.
PCNL as a primary treatment for patients with renal stones has been resurgent during the last decade, 15 leading to an increase in variations of the technique. In light of this, the Clinical Research Office of the Endourological Society (CROES) has conducted a prospective observational study of consecutive patients who were treated with PCNL at centers around the world over 1 year. 16 The purpose of the CROES PCNL Global Study was to establish a prospective global database for the current indications and outcomes of PCNL. The present analysis of the database examined postoperative complications of the PCNL procedure using the modified Clavien classification system and the influence of selected risk factors on the risk of complications.
Patients and Methods
The CROES PCNL Global Study was a prospective observational study during which data were collected for consecutive patients who were treated at each participating center over a 1-year period. The study organization and methods have been described previously. 16 Perioperative complications were assessed and scored according to the modified Clavien classification system 2 as applied to PCNL 13 (Table 1).
Study objectives
The objectives of this analysis were: To identify the common complications of PCNL; to identify risk factors for the development of postoperative morbidity after PCNL; to assess the relationship between the modified Clavien classification system (Clavien score) and American Society of Anesthesiologists (ASA) physical status classification scores; and to explore the possible development of a prediction model of Clavien score based on identified risk factors using multivariate analysis.
Analytical and statistical methods
In this analysis, the Clavien classification system was treated as an ordinal scale with values from 1 to 8, as follows: 1, Clavien grade 0 (no complications); 2, Clavien grade I; 3, Clavien grade II; 4, Clavien grade IIIa; 5, Clavien grade IIIb; 6, Clavien grade IVa; 7, Clavien grade IVb; and 8, Clavien grade V (death during the postoperative period). Because more than 50% of patients had no complications, for comparative and statistical analyses, 1 was used as the reference point of the ordinal scale and the difference between each level in the scale were assumed to be equivalent. An example of the calculation performed is as follows. Assuming the mean Clavien score for patients with cardiovascular disease (CVD) was 1.48 while for those without CVD, it was 1.33. This gives an absolute difference in the mean Clavien score of 0.15; the relative increase in Clavien score from the presence of CVD was therefore 11.2%; ie, 0.15/1.33×100%.
Based on published literature, the relationship between Clavien score and the following patient characteristics and operative factors was analyzed: age, sex, weight category, ASA physical status classification score, CVD status, diabetes status, anticoagulant use, urine microbiologic culture, stone load, clinical center PCNL case volume, and operative time. Patients were assigned to groups according to these variables. The mean Clavien score for each group and the intergroup difference in mean Clavien scores was calculated.
For patients with nonstaghorn calculi, renal stone load was calculated by aggregating the estimated volume of each stone using the formula: Total stone load=∑(length×width×Π×0.25). 17 Patients were assigned according to their calculated total stone load to groups with low (up to and including the median stone burden of 353 mm3) or high (above 353 mm3) stone burden.
Different clinical centers were categorized according to PCNL case volume as follows: Low volume centers <25 cases; medium volume centers 25–100 cases; and high volume centers had >100 cases during the 1-year study period.
For multivariate logistic regression analysis, the Clavien scores were grouped into minor complications (Clavien grades I and II) and major complications (Clavien grades III and IV), as previously defined. 18 The interaction of the selected variables with minor and major complications was then analyzed by standard regression analysis methods.
Results
Data were obtained from 5803 patients at 96 study centers in Europe, Asia, North America, South America, and Australia for the total database. Clavien scores were collected for 5724 (98.6%) patients, of whom 1175 (20.5%) patients experienced one or more complications.
Postoperative complications
The most frequent complications were fever and bleeding, occurring in 161 and 147 patients (Fig. 1). Urinary leakage, including an internal leakage around the kidney that may necessitate secondary drainage, hydrothorax, hematuria, urinary tract infection, and urinary fistula also occurred in 20 or more patients. According to the modified Clavien classification, the majority of complications (n=634, 54.0%) were classified as Clavien grade I (Fig. 2). Two patients died during the postoperative period because of fatal urosepsis.
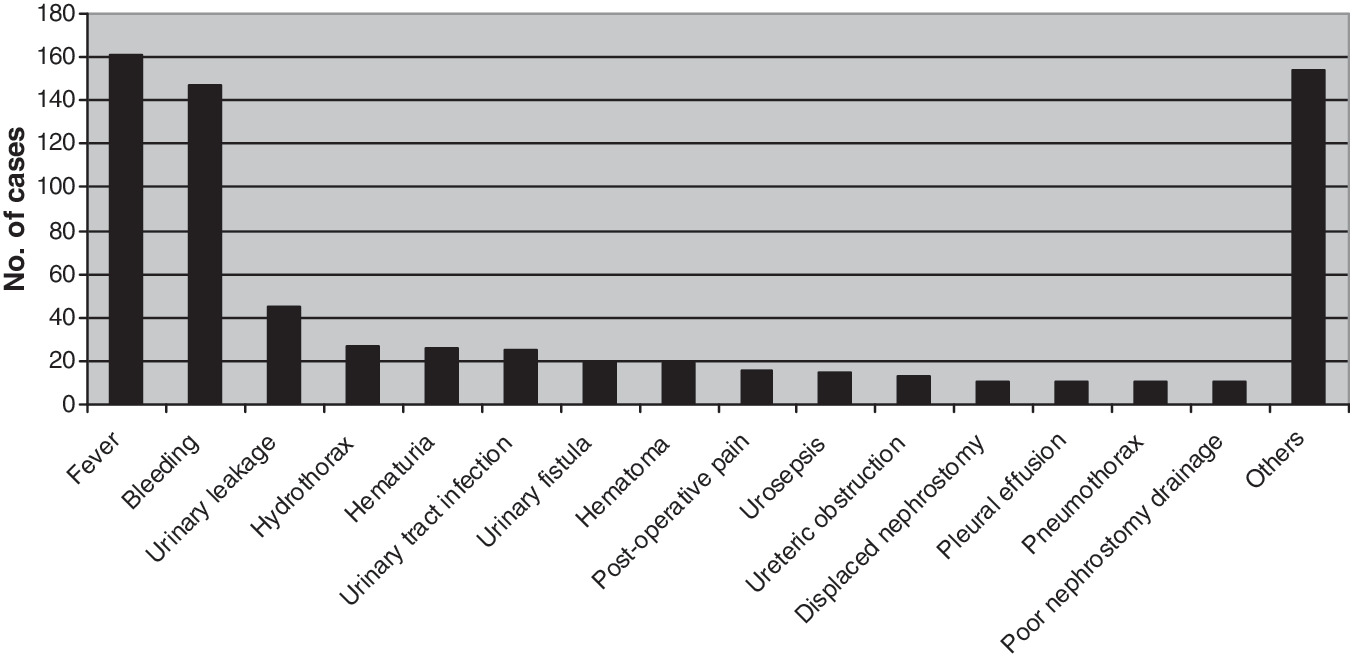
Number of complications occurring in 10 or more patients.

Distribution of modified Clavien grading scores.
Relationship between Clavien score and risk factors
The mean Clavien scores for selected patient and procedural characteristics are shown in Table 2. The skewed distribution of the Clavien scores in all patients with complications, as shown in Figure 2, also occurred in the distribution of scores in each risk factor subgroup. The factors associated with the largest absolute increases in mean Clavien score were: ASA physical status classification IV (0.75), ASA physical status classification III (0.34) (relative to ASA physical status classification I), use of anticoagulant medication (0.29), positive microbiologic urine culture (0.24), and the presence of concurrent CVD (0.15). For comparison, the relative increases in mean Clavien score were: ASA physical status classification IV (58.1%), ASA physical status classification III (26.4%) (relative to ASA physical status classification I), use of anticoagulant medication (21.5%), positive microbiologic urine culture (18.1%), and the presence of concurrent CVD (11.3%). Sex, age ranges <19 years and 40 to 59 years (relative to age 19–<40 years), and being overweight or obese had no or a negligible impact (<5% change) on mean grading score. All other selected risk factors increased the mean grading score by 5% to 10%.
BMI categories defined according to the World Health Organization.
SD=standard deviation; BMI=body mass index; ASA=American Society of Anesthesiologists; PCNL=percutaneous nephrolithotomy.
Relationship between ASA physical status classification and Clavien score
In view of the fact that higher ASA physical status classification scores corresponded to higher Clavien score (Table 2), the relationship between the two grading systems was studied in more detail. Mean (95% confidence interval) Clavien score calculated for each ASA score category is shown in Figure 3. The mean number of patients in each ASA category decreased with increasing ASA score from 3017 with ASA score 1 to 51 patients with ASA score 4. Of note, as the ASA score increased, the mean Clavien score similarly increased; ie; the chance of having a complication increased for every increase in ASA score.
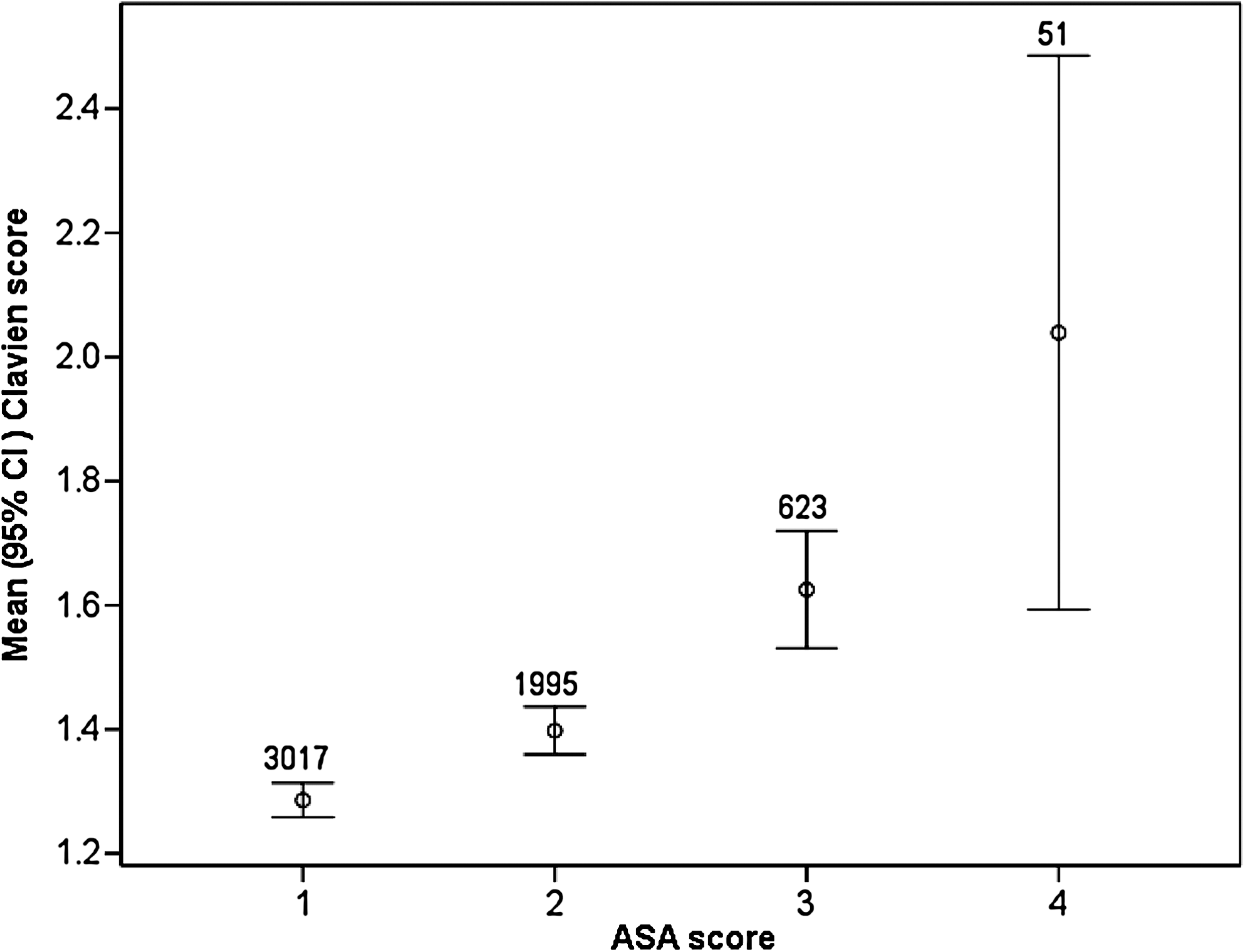
Relationship between Clavien score and ASA score. CI=confidence interval.
Multivariate regression analysis of potential predictors of Clavien score
Multivariate regression analysis of the selected patient and procedural characteristics revealed that operative time and ASA score were significant predictors of higher mean Clavien scores (Table 3). The odds of having a major complication (Clavien IIIA and above) increased as the operative time of the patients increased; patients with an operative time lasting between 51 and 75 minutes had the lowest odds of postoperative complications. The odds of a major complication increases in tandem with an increase in the ASA score. The following covariates were not associated with increased risk of major or severe complications: CVD, diabetes mellitus, case volume, body weight, and age categories.
References levels: Operating time (Short: ≤50 minutes) and ASA score (ASA 1).
Statistically significant at P<0.05.
ASA=American Society of Anesthesiologists.
Discussion
The CROES PCNL Global Study is the largest database of patients who were treated with PCNL to be reported to date. 16 The results were collected from patients with a variety of indications for PCNL in a wide range of clinical centers worldwide, and thus reflect the routine clinical use of this technique. Consistent with previous studies, 19 the results of the CROES PCNL Global Study show that while complications after PCNL are common, and most, such as bleeding or fever, are medically controllable through good clinical surveillance. Major complications, such as septicemia, renal hemorrhage necessitating intervention, pleural injury, and colonic injury, are rare. In the present study, approximately 80% of all complications were minor, and only 20% were major. This emphasizes the importance of grading perioperative complications according to their severity and reinforces the need for a reliable and easy-to-use system for classifying and recording complications.
In the current analysis, we used the absolute difference in mean Clavien score as a proxy for the impact of each risk factor. Thus, a risk factor that is associated with a larger absolute change in mean Clavien score has more impact on actual Clavien scores, and thus a greater increase in risk of postoperative complications. Conversely, variables that impart a lower mean difference in mean Clavien score have less impact on the actual grading score and are less likely to increase the risk of complications. Using this approach, five risk factors were identified that were associated with a marked increase in mean Clavien score and thus represent risk factors for increased likelihood of postoperative complications: ASA physical status classification III or IV, use of anticoagulant medication, positive microbiologic culture from urine, and the presence of concurrent CVD.
The ASA physical status classification is a widely accepted method of evaluating perioperative risk and is a predictor of postoperative outcome. 20 This classification is not, however, specific to urologic procedures nor to risk of postoperative complications. In addition, interobserver inconsistency can be marked. 21 In PCNL, the overall complication rate has been shown to be similar in patients who are identified as high risk (ASA III or IV) or low risk (ASA I or II). 22 In the present study, the distribution of ASA physical status classification scores varied across Clavien scores (Fig. 3). This suggests that characteristics of patients that vary with ASA physical status have different effects on the severity of subsequent complications as graded by the modified Clavien classification system.
Given the frequency of postoperative bleeding after PCNL, identification of anticoagulant medication use as a predictor of postoperative complications is not surprising. Use of this procedure in patients who are receiving long-term anticoagulant therapy poses a clinical dilemma. Current clinical experience suggests that PCNL can be performed on these high-risk patients with adequately planned cessation of anticoagulant therapy; eg, from 10 days preoperatively to 5 days postoperatively. Patients should be informed of the increased risks of thromboembolic events and postoperative hemorrhagic complications. 23,24 A positive microbiologic culture from urine is also not unexpected as a risk factor for postoperative complications. Although patients with fever post-PCNL are more likely to have a positive urine culture, 25 stone culture and pelvic urine culture may be more useful than preoperative bladder urine culture, 26,27 which often fails to identify stone-colonizing pathogens. 28
The presence of comorbidity, such as renal insufficiency, diabetes, morbid obesity, and pulmonary or CVD, has been reported to increase the risk of complications during or after PCNL. 19 Major complications after PCNL have been reported to be at least 2.5 times more common in patients with diabetes mellitus. 29 In the present analysis, while the presence of CVD was associated with an increase in mean Clavien score of more than 11%, the presence of diabetes conferred only a slightly higher risk of postoperative complications. Similarly, while it is accepted that obesity generally places surgical patients at greater risk of complications, several studies including the present indicate that complication rates after PCNL in obese patients are similar to those in nonobese patients 30 and are independent of body mass index. 31,32
Patients whose operations lasted longer than 75 minutes (76–115 minutes) had statistically significantly more severe postoperative complications (odds ratio 1.58) compared with those whose operative time was shorter than 50 minutes. The risk of more severe postoperative complications increased even further for those whose operative times were more than 115 minutes (odds ratio 2.06). The difference in the risk for more severe postoperative complications between those patients who had 50 minutes or less and those whose operative times were between 51 and 75 minutes was not statistically significant.
Similarly, patients who had ASA scores of 3 and 4 had statistically significantly more severe postoperative complications (odds ratio 1.17 and 2.27, respectively) compared with those who had an ASA score of 1. There was, however, no significant difference between patients with ASA scores of 1 and 2 as far as the risk of more severe postoperative complications is concerned.
Studies of surgical management of urolithiasis have tended to focus on radiologic outcomes, 33 and published clinical trials contain significant deficiencies in reporting adverse events outcomes. 33 This study suggests that further analysis of the risk factors that affect PCNL outcome is needed. Postoperative complications directly impact patient quality of life, but there is currently no disease-specific quality of life instrument. 34 Refinement of the modified Clavien classification system, as suggested elsewhere, 6,14,13 perhaps with incorporation of validated risk factors, would support better targeting of PCNL.
Conclusion
Further analysis of the risk factors that affect PCNL outcome and refinement of the modified Clavien classification system are needed to enable better identification of patients at increased risk of complications after PCNL. The development of a disease-specific tool to predict risk of postoperative complications would help to improve further the already low major complication rates of this important urologic technique.
Footnotes
Acknowledgment
The PCNL Global Study was supported by an unrestricted educational grant from Olympus.
Disclosure Statement
No competing financial interests exist.