
Abstract
Purpose:
We evaluated the usefulness of laparoendoscopic single-site (LESS) ureterolithotomy with a homemade single port device for upper ureteral stones in patients in whom previous shockwave lithotripsy or ureteroscopic stone surgery had failed or the stone was suspected to be impacted.
Patients and Methods:
LESS ureterolithotomy was performed on 30 patients by using a homemade single port device composed of an Alexis wound retractor and surgical glove. The mean age of the patients was 42.47±11.15 years (range 24–65 y), and the male-to-female ratio was 13:17. The mean stone diameter was 1.77±0.47 cm. One patient underwent a bilateral operation for bilateral ureteral stones.
Results:
The LESS surgery was converted to conventional laparoscopic surgery in one case. The mean operative time was 110.43±43.75 minutes. The mean length of hospital stay was 3.40±1.54 days. None of the patients used patient-controlled anesthesia, and none presented with major complications. The visual analog pain scale score improved significantly by postoperative day 7 (from 6.87±1.61 preoperatively to 1.67±1.16; P<0.001), and 28 (93.3%) patients said they were satisfied with the postoperative outcome. Postoperative radiologic evaluation revealed that the stones had been removed completely in 28 cases. There were no cases of urinary leakage.
Conclusion:
LESS ureterolithotomy using a homemade single port device can be considered to be a feasible and safe alternative to conventional laparoscopic ureterolithotomy.
Introduction
Most conventional laparoscopic ureterolithotomy procedures use three or four transcutaneous ports. For bilateral surgeries, one or two additional instrument ports should be installed on the affected side. 3 A recently reported novel technique, however, the laparoendoscopic single-site (LESS) surgery technique, has recently garnered considerable attention. This technique involves a single incision site through which the laparoscopic instrument is inserted. The objective of this technique is to minimize scarring, and indeed, feasibility studies have shown that the LESS technique improves the esthetic outcomes and can be used for various conventional laparoscopic surgery procedures. 4 To date, however, there have been no reports on the usefulness of LESS ureterolithotomy to remove ureteral stones with large patient samples.
To address this, the present study was performed to investigate the efficacy and safety of ureterolithotomy using a homemade single port device in patients who were suspected to have an impacted stone or whose previous URS or SWL procedure failed to remove their stone.
Patients and Methods
Patients
In total, 30 patients who underwent LESS ureterolithotomy in four medical centers in Korea between April 2009 and December 2010 were enrolled. All four medical centers followed the same study protocol. The surgical decisions were made after obtaining informed consent from the patients and Institutional Review Board approval from the ethical committee of the hospital. Before surgery, patients were fully informed about the various surgical methods that were available (open, laparoscopic or LESS ureterolithotomy) and the homemade single port device. The mean patient age was 42.47±11.15 years (range 24–65 y), and the male-to-female ratio was 13:17. To make a diagnosis, a preoperative work-up that consisted of abdominal ultrasonography, CT, and/or intravenous urography was performed. Patients who were suspected to have an impacted upper ureteral stone or whose previous SWL or URS procedure failed to remove their stone were selected. LESS ureterolithotomy was performed in 16 left-sided cases and 15 right-sided cases. In one case that was surgically indicated, bilateral surgery was performed. The mean stone size was 1.77±0.47 cm, and the mean body mass index was 23.07±3.58 (Table 1).
Surgical procedure
A homemade single port device was prepared by using a small-sized Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA) and a powder-free surgical glove. To eliminate scarring, a crescent-shaped 2 to 3-cm long incision was made along the lateral or lower margin of the umbilicus, and the wound retractor was inserted (Fig. 1A). The upper wound retractor ring was covered with a size 6½ surgical glove, and the surgical glove was rolled down around the ring to eliminate any empty space between the abdominal wall and the glove. Three fingers of the glove were then cut off. Two 12-mm trocars and one 5-mm trocar were then fixed to the cutoff finger remnants by using a silk 1-0 or rubber band (Figs. 1B and C).
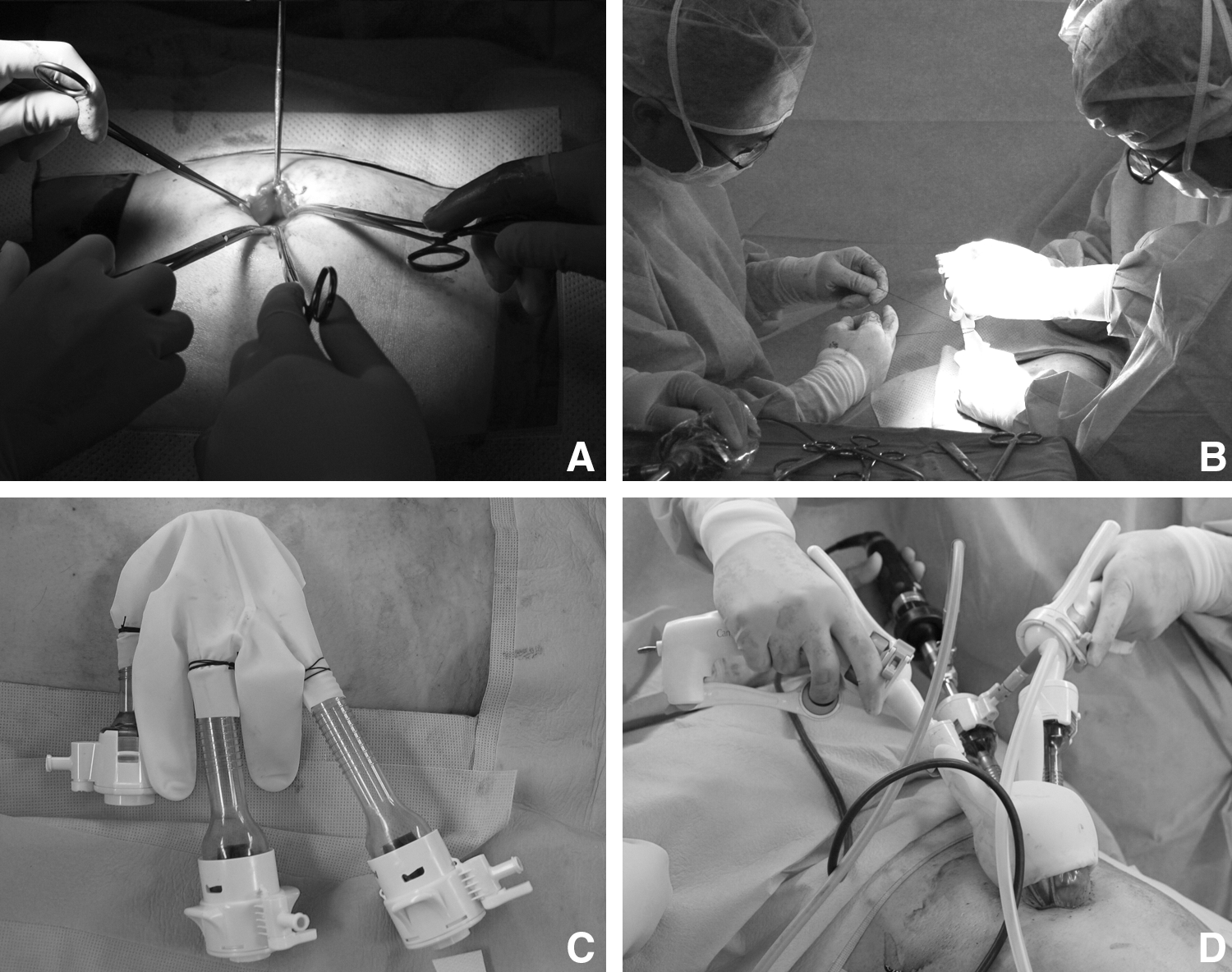
Laparoendoscopic single-site ureterolithotomy.
Under general anesthesia, the patient was placed in a flank position at a slanted angle of 70 degrees. An intra-abdominal CO2 pressure was maintained at 15 mm Hg. A 10-mm rigid laparoscope was inserted into one of the three trocars, and flexible laparoscopic instruments, namely the LaparoAngle® (CambridgeEndo, Framingham, MA) and the Roticulator® (Autosuture, Norwalk, CT), were inserted into the remaining two trocars (Fig. 1D). These laparoscopic instruments were staggered into the abdomen through the single incision wound. Thereafter, surgery was performed with the tip of LaparoAngle® flexed at an angle of 90 degrees so that it resembled the basic 5th movement of ballet. 5
Within the peritoneum, the large intestine was retracted and placed on the medial side, and the ureter was exposed. After locating the ureteral stone, a longitudinal incision that was big enough to remove the stone was made by using a pair of laparoscopic Metzenbaum scissors, and the stones were removed with laparoscopic forceps (Fig. 2A). Subsequently, the guidewire that had been placed below the stone before starting surgery was advanced upward and a Double-J stent was inserted using the guidewire (Figs. 2B and C), if possible. The vertically resected ureter was subjected to continuous suture using 4-0 or 5-0 polyglactin (Fig. 2D). Surgicel® (Ethicon Inc., Somerville, NJ) was then placed onto the suture area. Large stones were placed into a Lap-bag® (Sejong Medical, Paju, Korea), which was then extracted.

After confirming the absence of hemorrhage, a drain was placed in the vicinity of the ureter. In cases of failed Double-J stent insertion, the patient was then placed in the lithotomy position, and a Double-J stent was inserted by using the guidewire that had already been inserted through the ureter under fluoroscopy.
Statistical analysis
The preoperative and postoperative visual analog scale (VAS) pain scores of all subjects were analyzed by paired t test. In VAS, the severity of pain is classified according to a 0 to 10 point scale that indicates the degree of pain, where 0 indicates a complete lack of pain and 10 indicates the most severe pain. Patient satisfaction was analyzed by using four criteria: “Very satisfied,” “somewhat satisfied,” “somewhat dissatisfied,” and “very dissatisfied.” In our study, the term satisfied included both very satisfied and somewhat satisfied. Comparison of the operative time was analyzed by Mann-Whitney U test. The data were analyzed by using Open
Results
None of the surgical procedures needed conversion to open surgery, but in one case, a transcutaneous port had to be placed in addition to the homemade single port device. The mean duration of LESS ureterolithotomy was 110.43±43.75 minutes, and the mean estimated blood loss was 61.17±3 6.40 mL. For the first 15 cases, the mean operative time was 136.87±48.29 minutes, but for the later 15 cases, it had shortened significantly to 84.00±11.66 minutes (P=0.001) (Fig. 2). Thus, the operative time shortened as the surgeons' experience grew. The mean length of hospital stay was 3.40±1.54 days. There were three cases of minor postoperative complications (10.0%): Two cases of fever (6.7%) and one case of mild ileus (3.3%). There were no major complications.
The mean preoperative VAS score of flank pain was 6.87±1.61. This dropped to 4.37±1.52, 2.60±1.52, and 1.67±1.16 on postoperative days 1, 2, and 7, respectively. The day 7 postoperative score was significantly lower than the preoperative score (P<0.001). In addition, while the day 2 score did not differ significantly from the day 1 score (P=0.807), the day 3 score was significantly lower than the day 1 score (P<0.001). None of the patients used patient-controlled anesthesia postoperatively. In all 30 patients, a normal diet was initiated on the day of surgery. On average, the patients were able to return to normal activity after 3.12±1.98 days. A survey of the degree of patient satisfaction showed that 17 were very satisfied, 11 were somewhat satisfied, and two were somewhat dissatisfied. Thus, 28 (93.3%) patients were satisfied with their postoperative outcomes. The patient who underwent bilateral ureterolithotomy had no complications and felt very satisfied. By postoperative month 1, the mean wound size was 2.96±0.52 cm.
In all but two cases, the stones were removed successfully. In one case, a small 0.3-cm stone had migrated to the renal pelvis, and in another case, a 0.4-cm impacted stone was not extracted after the main 2.1-cm stone was removed. On postoperative follow-up, which included simple radiography and intravenous urography, all patients were asymptomatic and did not exhibit obstruction or stricture formation.
Discussion
At present, SWL, retrograde ureteroscopy, and percutaneous antegrade ureteroscopy are accepted as treatment modalities for ureteral stones that are 1 cm or larger. 6 Sometimes endourologic management fails, however, or appropriate facilities needed for the management of large impacted ureteral stones and upper ureteral stones (ie, a flexible ureteroscope and a laser) are not available. In such cases, ureterolithotomy becomes the next option. 7
The development of laparoscopic procedures and techniques means that laparoscopic surgery has now replaced the standard open surgery of the past. In 1992, Raboy and associates 8 reported a transperitoneal laparoscopic ureterolithotomy. This procedure then became frequently used after Gaur and colleagues 9 developed a retroperitoneal approach for laparoscopic ureterolithotomy in 1994. Goel and coworkers 10 have reported that while laparoscopic ureterolithotomy is similar to open ureterolithotomy in terms of operative time and blood loss, it is superior with regard to narcotics use, hospital stay, and the duration needed for recovery to normal activity.
Since these developments, conventional laparoscopic surgery has undergone various changes that have aimed to reduce the invasiveness of the surgery. These developments have recently resulted in new techniques such as natural orifice transluminal endoscopic surgery and LESS. Since the Laparoendoscopic Single-Site Surgery Consortium for Assessment and Research was founded in 2008, the term LESS surgery now is used to describe laparoscopic surgery through a single incision site. 11
LESS surgery has several major advantages over conventional laparoscopic surgery. The latter requires three to four transcutaneous ports, and in some cases, an additional opening is needed to extract a resected organ. In contrast, LESS surgery evokes little pain and a barely noticeable wound, because the single incision is made around the umbilicus. In addition, conventional laparoscopic surgery needs additional transcutaneous ports for contralateral procedures after one side is operated on, whereas additional wounds are not needed in LESS in the case of bilateral concomitant operations. 12 Because there is only a port device around the umbilicus, however, the LESS procedure is technically more difficult to perform than the conventional laparoscopic procedures and the techniques of the past. 13
In the urologic field, during the 2007 World Congress of Endourology Meeting, Rane and colleagues 14 reported a LESS nephrectomy using the R-port (Advanced Surgical Concepts, Dublin, Ireland) for the first time. Thereafter, many surgeons have used this technique to treat various urologic diseases and have reported its usefulness and safety. Table 2 summarizes the studies on conventional laparoscopic and LESS ureterolithotomy.
L/M/U=lower/middle/upper ureter; CRP=conventional retroperitoneal laparoscopic ureterolithotomy; CTP=conventional transperitoneal laparoscopic ureterolithotomy; LESS-TP=laparoendoscopic single-site surgery transperitoneal ureterolithotomy; LESS-RP=laparoendoscopic single-site surgery retroperitoneal ureterolithotomy.
The first report of LESS ureterolithotomy was published in 2008 by Rane and associates, 15 who described one patient with a 2.5-cm stone in the upper ureter who was treated by LESS ureterolithotomy using an R-port that was placed in the umbilicus. 15 In 2010, Jeon and coworkers 16 reported 50 cases of LESS and robot-assisted LESS surgery using a homemade single port device composed of a wound retractor and a surgical glove; these 50 cases included one LESS ureterolithotomy case, in which the patient was treated for a 2-cm ureteral stone. The operative time was 310 minutes, and the hospital stay was 6 days. Around the same time, Ryu and associates 17 reported that of their 14 patients who were treated by LESS surgery using a homemade single port device, two cases involved LESS ureterolithotomy using a retroperitoneal approach. Micali and colleagues 18 also recently reported 11 cases of retroperitoneal LESS renal and ureteral surgery; of these, three cases of ureterolithotomy were performed by using TriPort (Advanced Surgical Concepts, Bray, Ireland) and a 5-mm flexible laparoscope. After stone extraction, three or four ureteral interrupted stitches were made with a 5-mm rigid needle holder using 4-0 polyglactin.
Thus, several studies have shown that when URS or SWL fails or an impacted stone is suspected, LESS ureterolithotomy can serve as an alternative to conventional laparoscopic ureterolithotomy. These studies, however, are all based on small sample sizes. One study with a slightly larger sample size is that of Kim and coworkers, 19 who recently analyzed the feasibility and efficacy of LESS ureterolithotomy using a homemade single port device in their first seven cases. The mean operative time was 197 minutes, and the mean hospital stay was 3.3 days. The surgical outcomes were excellent. These investigators commented that compared with conventional laparoscopy, LESS surgery involves a unique learning curve because of the difficulty in manipulating the instruments in the narrow visual field. In addition, when suturing the ureter, they usually used a conventional rigid needle holder. It should be noted that the excellent surgical outcomes of these seven cases reflects the experience of the surgeons, who had performed more than 20 LESS surgeries previously.
The combination of a flexible ureteroscope and a holmium:yttrium-aluminum-garnet (YAG) laser is the most effective therapeutic modality for managing upper ureteral stones via ureteroscopy. In the present study, however, a flexible ureteroscope and a holmium:YAG laser were unavailable. Therefore, in 17 cases in which SWL had failed in removing a ureteral stone completely, the authors then performed LESS ureterolithotomy. In the remaining 13 cases, LESS ureterolithotomy was performed immediately rather than after SWL or ureteroscopic surgery. The reasons for this are as follows: In eight cases, the stones were so large (on average, 2.41±0.29 cm) that repeated SWL would have been necessary; in another case, the stone was located in the upper ureter and would have been hard to remove effectively by using a rigid ureteroscope; in the remaining four cases, an impacted stone was suspected.
There was one case of laparoscopic conversion early in the series, but for the remaining 29 cases, LESS surgery was conducted successfully by the four surgeons in the four participating centers. The most obvious advantage of LESS ureterolithotomy is that only one incision is made during surgery. This results in high esthetic satisfaction and reduced postoperative pain. The single incision is particularly advantageous for bilateral surgeries, because LESS surgery does not need the installation of additional ports after the position of the patient is changed. Indeed, as observed by other studies, in the present study, there was a marked improvement in VAS pain scores after the operation, and 28 (93.3%) patients said they were satisfied. Moreover, the single patient who underwent bilateral surgery reported very high satisfaction.
Apart from the success of the surgery itself, the mean operative time was 110.43±43.75 minutes, which is similar to or shorter than the operative times reported for conventional laparoscopic surgery. Notably, the first 15 cases took considerably longer on average than the subsequent 15 cases (137 vs 84 min, respectively), which reflects the sharp learning curve of the four surgeons. In addition, all 30 patients were able to eat on the day of the surgery and returned to their ordinary life within 4.12±1.98 days after surgery, which indicates a fast recovery. Complications that can be caused by LESS ureterolithotomy include peritoneal organ injury, ureteral stricture, and urine leakage. There were no major complications after surgery in this study, however.
In summary, LESS ureterolithotomy in our hands was associated with reasonable operative times, reduced pain, good esthetic satisfaction, and fast recovery. Another advantage of LESS ureterolithotomy is that large upper ureteral stones can be removed completely by a single surgical procedure. Thus, LESS ureterolithotomy is suitable as an alternative to open or conventional laparoscopic ureterolithotomy for the management of large impacted upper ureteral stones. Moreover, in the case of SWL or URS failure, it may be the most effective alternative. Our study on LESS ureterolithotomy has some limitation, however. First, we only evaluated the feasibility of LESS ureterolithotomy, not comparing it to conventional laparoscopic ureterolithotomy. Second, 30 cases were not performed by a single surgeon.
Relative to other LESS surgeries that have been conducted by the authors, there were a few problems associated with LESS ureterolithotomy. First, the surgery itself was difficult. Although the surgeons already had experience in conventional laparoscopic surgery, including ureterolithotomy, they found it difficult in the first few cases to repair the ureter by using the flexible instruments and the rigid needle holder. Second, the homemade single port device used by the authors was easily damaged: in five cases, the surgical glove was torn when the needle was inserted into the port device during ureter suturing. With increasing experience, however, these problems occurred less and less frequently.
Conclusion
Because of technologic advances in SWL and URS, it has become less and less necessary to perform ureterolithotomy. In cases of incomplete stone removal via SWL or URS, or the unavailability of appropriate facilities to manage large impacted ureteral stones or to conduct endourologic minimal invasive treatment, however, LESS ureterolithotomy can be considered as a safe and effective surgical method that can replace open or conventional laparoscopic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.