
Abstract
Purpose:
To compare photoselective vaporization of the prostate (PVP) using the 120W GreenLight™ laser with transurethral resection of the prostate (TURP) in terms of their cost to the Greek National Health Service (NHS) or to the Public Insurance Sickness Funds (PISF).
Patients and Methods:
A prospective cost evaluation with 1-year follow-up of 60 patients with infravesical obstruction of benign prostatic hyperplasia origin who underwent o either TURP (n=30) or PVP (n=30). The cost of equipment, consumables, anesthesia, drugs, inpatient hospitalization, and complication management within 1 year postoperatively were used to calculate the cost for the NHS. PISF reimbursements to hospitals and PISF opportunity cost from the lost days of work were used to calculate PISF perspective.
Results:
From the NHS perspective, the average cost was €1722 ($2371) for PVP and €2132 ($2935) for TURP. From the PISF perspective, the average cost for hospital reimbursement was €1348 ($1856) in the case of PVP and €938 ($1291) in the case of TURP. Nevertheless, in the case of patients still working, total PISF reimbursement cost was €2038 ($2806) for PVP and €2666 ($3671) for TURP.
Conclusions:
PVP for 40 to 70 cc prostates is preferable from the perspective of the NHS. From the perspective of PISF, PVP is less costly only in the case of patients who are still working, because patients who undergo PVP stay much less out of work. Further investigation in larger populations as well as in different protocols of PVP hospitalization and return to work times is deemed necessary to reinforce the conclusions of this study.
Introduction
Because of the relatively high cost of consumables, laser BPH therapies are traditionally considered to be more expensive than TURP. 9,10 In this study, a comparative cost analysis between PVP laser prostatectomy and TURP is being conducted to elucidate whether in the era of escalating healthcare costs, PVP is more costly as a standard care and thus should be deployed only in selected high-risk cases. Both treatment options were compared in terms of their cost to the Greek National Health Service (NHS) or to the Hellenic Public Insurance Sickness Funds (PISF), as well as in terms of the productivity loss imposed on working patients.
Patients and Methods
Patient selection
After Institutional review board approval, between August 2008 and December 2009, 60 patients with infravesical obstruction of BPH origin were treated either with TURP (n=30) or with PVP (n=30) in the University Hospital of Patras by a single surgeon (EL). Written informed consent had been obtained from all patients in the current study. Inclusion criteria for both groups included patients with prostate sizes between 40 and 70 cc and lack of any previous surgical/endoscopic treatment for BPH. Patients were randomly allocated into the two treatment groups on a one-to-one basis. Nevertheless, randomization was restricted in patients with severe cardiovascular or respiratory comorbidities as well as in patients receiving anticoagulant treatment (a total of nine patients). These patients were all included in the PVP group, given the better safety profile of the approach. Because the latter bias in patient selection ended up with selecting a significant (30%) percent of patients in the PVP group, this cannot be considered a randomized study. A follow-up of at least 1 year was achieved in all patients included in the study.
Population characteristics
Mean patients age (69.9 y for PVP vs 67.6 y for TURP) and prostate size (52.8 cc for PVP vs 55.2 cc for TURP) were comparable in both groups. Nevertheless, the percent of patients over 65 years was higher in the PVP group (80% vs 60% for TURP) because patients with severe comorbidities (usually older) were all included in this group. None of the patients in either group had urinary retention preoperatively.
Treatment characteristics
For TURP treatment, a monopolar technology was used in all cases. Regularly, the operation was conducted under general or spinal anesthesia, and the urinary catheter was removed on postoperative day 4 before patient discharge. For the PVP group, the GreenLight HPS laser was used. In our department, PVP is regularly conducted under deep sedation. Patients receiving anticoagulants do not discontinue their treatment preoperatively. After PVP, patients are regularly discharged on postoperative day 1 after urinary catheter removal. In the case of patients who are still working, return to work is addressed 6 days after PVP and 15 days after a TURP procedure.
NHS treatment cost calculation
For each patient, the cost of disposables, anesthesia, drugs, inpatient hospitalization, and complication management within 1 year postoperatively was calculated. To that, the equipment cost per procedure was added to estimate patient cost per procedure from the perspective of the NHS. The equipment cost per procedure was calculated dividing the capital cost of equipment purchasing price with an estimation of total treatments per 7 years (which is an estimation of life span for the electrogenerator and the laser generator 11 ) and the cost of equipment maintenance per year with an estimation of the total number of treatments per year. Laser consumables cost reflected the cost of only one fiber per procedure, according to the manufacturer charge policy. Moreover, because in Greece, medical and nursing staffs are being paid by the NHS on a salary basis, the marginal cost of personnel per procedure was considered to be zero. The resources consumed were priced at true hospital cost in accordance to data collected from the hospital.
PISF reimbursement cost calculation
PISF reimburses Greek hospitals for each operation using standard reimbursement tariffs individually designated for each treatment. In addition, PISF reimburses hospitals for patient hospitalization using standard reimbursement tariffs per day of hospitalization. Finally, in the case of patients still working, PISF reimburses the opportunity cost of lost productivity using standard reimbursement tariffs per day lost from work. All reimbursement tariffs were obtained from the Hellenic National Gazette.
Statistical analysis
Because of the small sample size, the single hospital origin of data and because resource and treatment cost data were skewed, bootstrapping was used. 12,13 To compute the bootstrap standard error for the difference in sample means, we performed the bootstrap procedure in R, 14 resampling separately from the two original samples, as follows: Starting with an initial PVP sample of size 30, we drew 1000 resamples with replacement. Similarly, 1000 resamples were drawn with replacement from the initial TURP sample of size 30. From each pair of resamples, the difference in sample means was calculated. The significance of the cost difference of the two approaches (PVP, TURP) was investigated by calculating the mean and the confidence intervals of the bootstrap distributions; 99% confidence intervals not including the value zero declare a statistically significant difference at the α=0.01 level. To confirm that the results are valid, the bias (ie, the difference between the mean value of the original data and the mean value of the bootstrap distributions) was also calculated.
For the comparison of the two treatments, a cost-minimization analysis was performed, which is applicable in cases in which treatments are considered even with regard to efficacy. 15,16 To address the issue of surgeon dependent parameter of patient's discharge from hospital time and return to work period, a further analysis using simple matrix was conducted varying the hospital stay and return to work time. A P value of less than 0.01 was set as the level of statistical significance.
Results
Mean hospitalization was 1.2 days in the PVP group and 4.9 days in the TURP group. In the PVP group, short-term adverse events where encountered in nine (30%) patients, including mild hematuria (which did not necessitate blood transfusion) in two patients, both of whom were receiving anticoagulation treatment, LUTS in four patients, and transient urinary retention after catheter removal in three patients. The latter three cases were managed by recatheterization and postponement of discharge for 1 additional day. On postoperative day 2, all three patients were catheter free and were discharged from the hospital. During the first year of follow-up, two cases of BPH recurred and necessitated reintervention via TURP, while one case of urethral stricture was managed successfully by urethrotomy.
In the TURP group, short-term adverse events were encountered in 13 (43%) patients, including hematuria in four patients, two of whom needed blood transfusion, LUTS in six patients, and transient urinary retention after catheter removal in three patients accordingly. Postponement of discharge was deemed necessary in four cases. During the first year of follow-up, two cases of BPH recurred and needed reintervention via TURP, while two cases of urethral strictures were managed successfully by optical urethrotomy. A summary of the main clinical parameters of each group is presented in Table 1.
PVP=photoslective vaporization of the prostate; TURP=transurethralresection of the prostate; SD=standard deviation; LUTS=lower urinary tract symptoms.
Based on the actual purchasing price and the cost of equipment maintenance, the equipment cost per case was estimated at €28 and €64 and the cost of consumables per procedure €288 and €1142 for TURP and PVP, respectively. Mean cost for anesthesia was €66 for TURP and €45 for PVP. The average hospital cost per day (excluding staff) was estimated at €280. Bootstrapping sensitivity analysis is presented in Table 2. Based on these data, from the NHS hospital perspective, the total cost was €1722 in the case of PVP and €2132 in the case of TURP, indicating a statistical significant difference in 95% level of significance (P<0.001). Based on the data collected, from the PISF perspective, the cost for hospital reimbursement was €1347 in the case of PVP and €937 in the case of TURP, indicating a statistical significant difference in 95% level of significance (P<0.001).
Observed: The sample mean difference of the original data.
Mean: The mean of the bootstrap distribution of the sample mean differences.
Bias: The difference between the Mean and the Observed. When this difference is small compared with the magnitude of the measured quantity (sample mean), there is evidence that the normality assumptions are met. SE: Standard error, ie, the standard deviation of the bootstrap distribution. Its value is taken into account for the Confidence Interval calculation based on the t-statistic.
95%/99% t-CI: Confidence Interval based on the t-statistic for α=0.05 and α=0.01 significance level, respectively. They are calculated as Mean±t30,0.05 *SE and Mean±t30,0.01 *SE, respectively. If these confidence intervals do not include the value 0, the difference in Means is significant at the corresponding level of significance.
95%/99% Bootstrap Percentile CI: Confidence Interval based on the 2.5%/97.5% or the 0.5%/99.5% percentiles of the bootstrap distribution respectively. If these confidence intervals do not include the value 0, the difference in Means is significant at the corresponding level of significance. When t-CI and BP-CI are close, there is evidence that the normality assumptions are met.
PVP=photoselective vaporization of the prostate; TURP=transurethral resection of the prostate; PISF=public insurance sickness funds.
Nonetheless, in the case of patients who were still working, PVP was proved less expensive from a PISF perspective; patient opportunity cost from the lost days of work was higher in the case of TURP because patients who underwent PVP returned to work earlier. In this perspective, the cost was €2038 in the case of PVP and €2666 in the case of TURP, indicating a statistical significant difference in 95% level of significance (P<0.001). Mean cost estimations from NHS and PISF perspective are summarized in Figure 1.
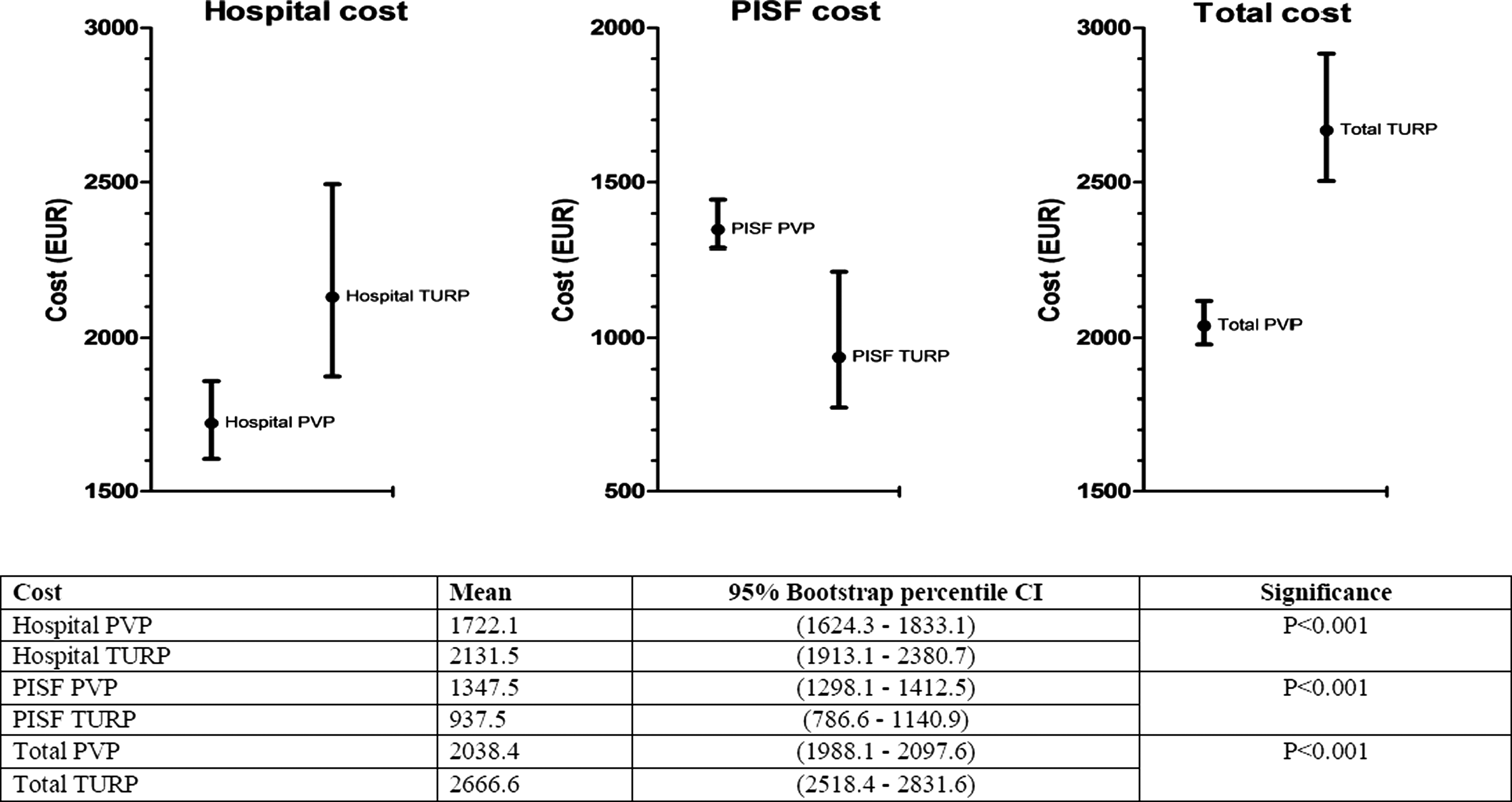
Hospital, Public Insurance Sickness Funds (PISF), and total cost comparison between photoselective vaporization of the prostate (PVP) and transurethral resection of the prostate (TURP). Calculated based on the bootstrapped population. CI=confidence interval.
From the NHS perspective, analysis taking into consideration varying days of hospitalization revealed that TURP would have the same cost as PVP if mean hospitalization was restricted to 3.5 days. Alternatively, in the case that PVP had been conducted on a day-case basis (zero days of hospitalization), then TURP would have had the same cost only if patients were discharged after a mean of 2.2 days of hospitalization (Fig. 2). From the PISF perspective, in the case of patients who were still working, analysis taking into consideration varying days of returning to work periods revealed that TURP would have had the same cost as PVP patients when TURP patients did return to work 5.91 days later that that of PVP patients. Consequently, when TURP and PVP patients had the same time of recovery, then TURP would be less costly from the PISF perspective as well (Fig. 3).
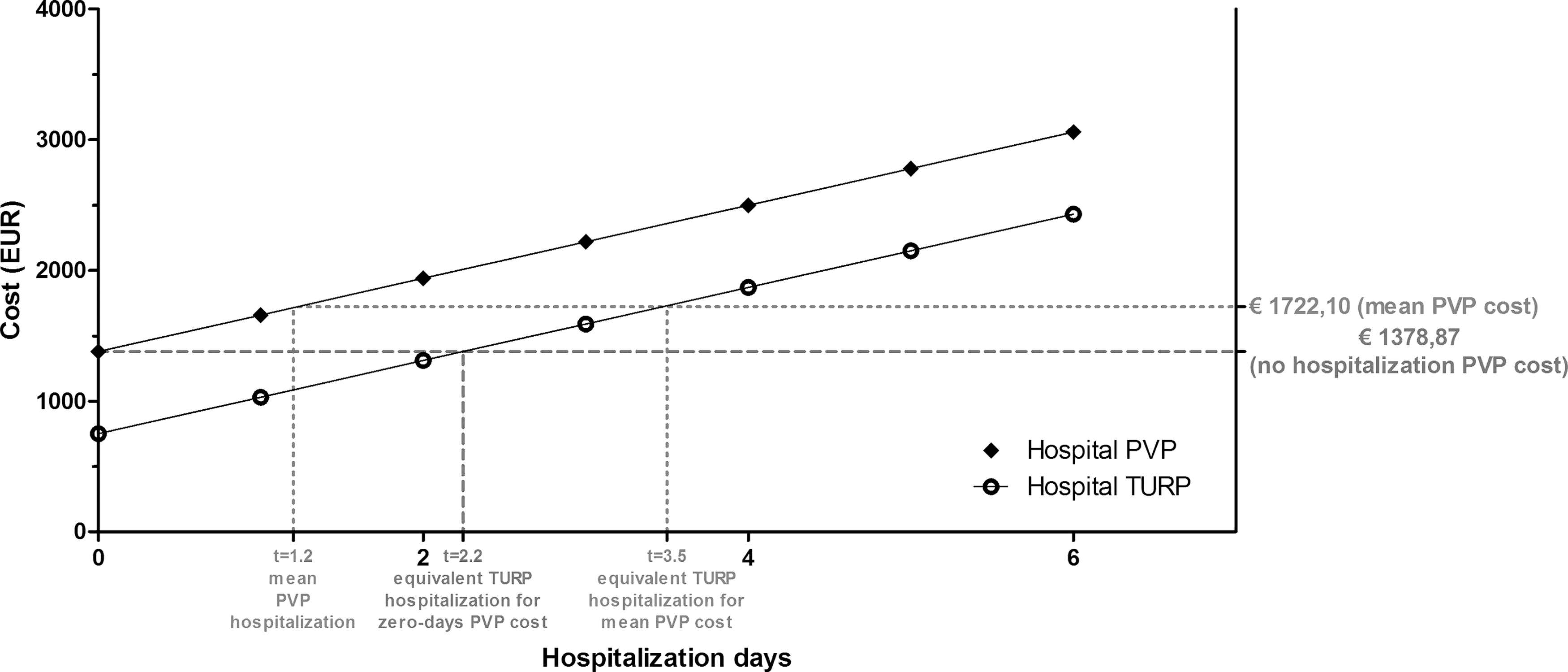
Hospital cost of photoselective vaporization of the prostate (PVP) and transurethral resection of the prostate (TURP) based on the days of hospitalization.
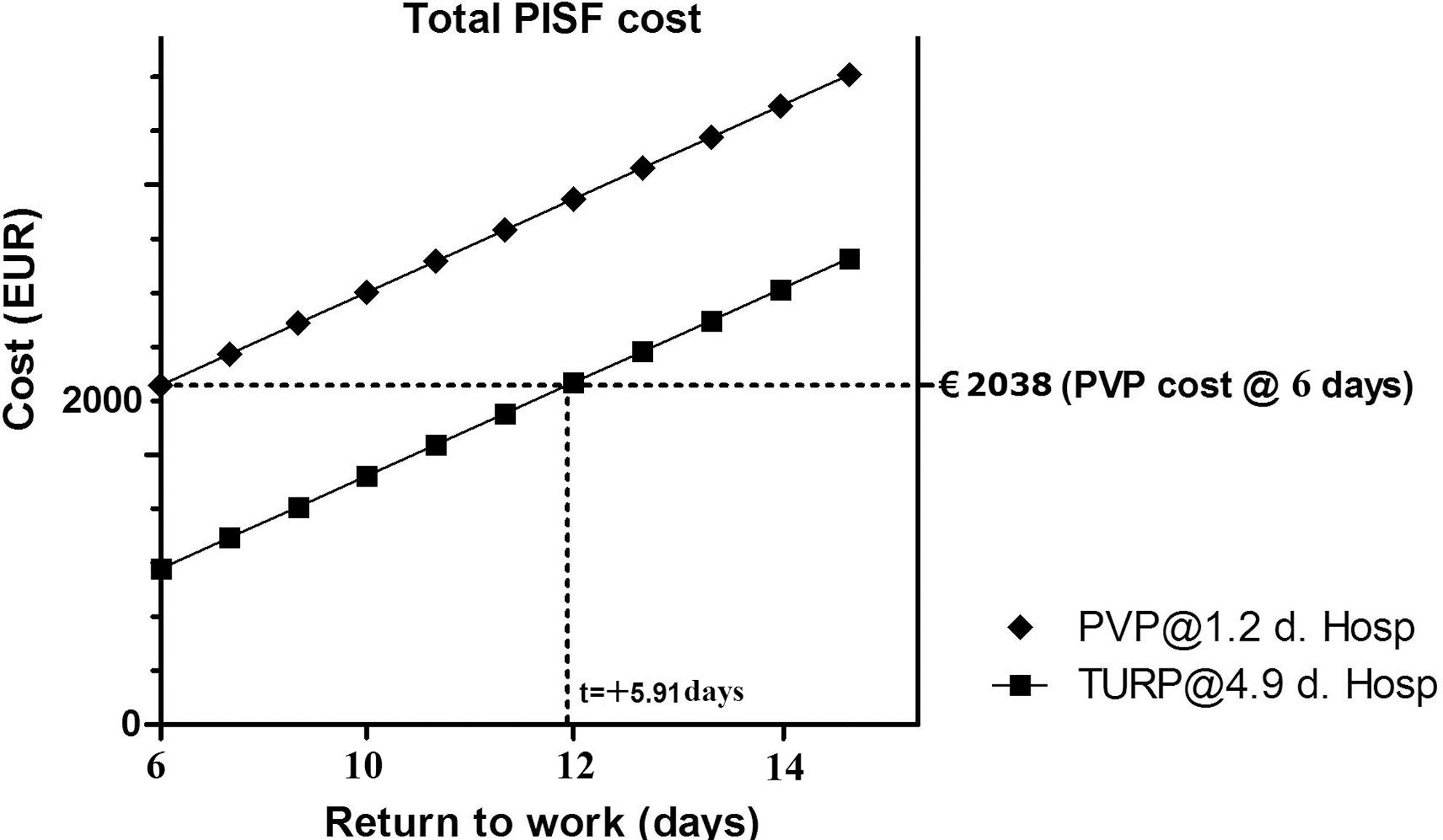
Public Insurance Sickness Funds (PISF) for photoselective vaporization of the prostate (PVP) and transurethral resection of the prostate (TURP) based on the days that patients are returning to work.
Discussion
Several studies have evaluated the cost of PVP laser prostatectomy in comparison with alternative surgical approaches. Ruszat and associates 17 have reported comparable medical costs of PVP and TURP. In Australia, Canada, and Texas, three relative studies have found that the cost of PVP per case was less than that of TURP, while in Turkey, PVP cost was significantly higher than that of TURP treatment. 18 –21 A limitation of the aforementioned studies was that only the cost of the initial procedure was taken into consideration and not the costs of mid- and long-term complications as well as the costs of potential reintervention procedures.
Stovky and colleagues 22 developed a decision-analytic Markov model to estimate the costs of five alternative procedural interventions for BPH including PVP, microwave thermotherapy, transurethral needle ablation, interstitial laser coagulation, and TURP. The estimated cost was found to be significantly lower for PVP than any other treatment modality at a 6-, 12-, and 24-month time horizon. Stafinski and coworkers, 23 in a meta-analysis of available economic evaluations of PVP and TURP, concluded that in Canada, in a center performing 1500 PVP procedures annually on an outpatient basis, the cost of PVP is estimated to be about one-half that of TURP, even after accounting for start-up cost (purchase and installation of the equipment).
In this study, from the Greek NHS perspective, PVP was found to be preferable as less costly than TURP because it was related to shorter hospitalization. In contrast, from the PISF perspective, PVP was more expensive than TURP when patients who were not working were treated, which is the case in the majority of BPH patients. Nevertheless, in the case of younger patients who were still working, which in our cohort accounted for 30% of the studied population, PVP was still less expensive because reimbursed lost days of work were much less in the PVP group.
Particular aspects of the current analysis are applicable only in the Hellenic NHS. Medical and nursing staff payment was excluded given that it is stable, not dependent on the number of executed cases, the applied technique, or the days of patient hospitalization. If this cost was taken into consideration, then inpatient cost would have been even higher and longer hospitalization of TURP would have had a greater impact on total cost. In addition, PISF reimbursement to hospitals for each day of hospitalization in Greece is based on a standard reimbursement tariff (€73) that covers only 26% of the true inpatient cost (mean cost per day of hospitalization was €280). Thus, longer hospitalization, related to TURP, does not increase significantly the total cost for PISF reimbursement. In contrast, if PISF reimbursement would cover the true hospital cost, then PVP would be preferable from the PISF perspective as well.
Limitations of the current study include the relatively small number of cases and the single institute origin of data. The cost differences in the TURP group seem to be largely driven by the longer hospital stay and recommended delay in returning to work, both of which are somewhat surgeon dependent. Thus, the particular analysis is valid only for surgeons in Greece, following the same protocol of hospitalization and return to work period. Further analysis taking into consideration varying times of hospital stay and return to work revealed that when PVP is conducted on a day-case basis, then TURP would be more expensive whenever patients were discharged later than postoperative day 2.2. In the case of PVP patients being discharged on postoperative day 1.2 (the outcome of the current cohort), then TURP would be equally expensive in patients being discharged after postoperative day 3.5. From the PISF perspective, PVP was found less costly whenever patients who were still working were allowed a recovery period of 5.9 days less than TURP patients.
In addition, the bias against PVP treatment, generated via including all patients with significant comorbidities in that group, might have a negative effect on the outcome of this study. Re-treatment rate (secondary TURP) within the first postoperative year in the PVP group, accounting for 10% of patients, is relatively high when compared with the rest of the literature reporting overall re-treatment rates up to 8.9% at 5 years postoperatively. 7 More favorable results in the latter group would have led to a more cost-effective profile of PVP. As in every economic evaluation, our study is based on particular assumptions (eg, all patients were readdressed to our institution for any postoperative complication, estimation of life span of equipment, etc), and sometimes even small mistakes in these could lead to a totally wrong conclusion. Still, our results are in accordance with most of the literature, which reinforces the conclusions drawn in this study.
Conclusions
PVP is preferable from the perspective of the NHS with regard to cost. Given the high number of cases per annum, the use of PVP can result in significant saving of resources, in addition to the well-established excellent safety profile of the approach. From the perspective of Hellenic PISF, PVP is less costly only in the case of patients who are still working, because patients who undergo PVP stay much less time out of work. Further investigation in larger populations as well as in different protocols of PVP hospitalization and return to work times is deemed necessary to reinforce the conclusions of this study.
Footnotes
Disclosure Statement
Authors have nothing to disclose.