
Abstract
Purpose:
To determine laparoscopic and robotic surgical practice patterns among current postgraduate urologists.
Materials and Methods:
There were 9,095 electronic surveys sent to practicing urologists with e-mail addresses registered with the American Urological Association.
Results:
Responses were received from 864 (9.5%) urologists; 84% report that laparoscopic or robotic procedures are performed in their practice. The highest training obtained by the primary laparoscopist was fellowship (31%), residency (23%), or 2- to 3-day courses (22%). Eighty-six percent report performance of laparoscopic nephrectomy in their practice, and 71% consider it the standard of care. Sixty-six percent of practices have access to at least one robotic unit, and 9% plan on purchasing one within a year. Attitudes toward robotics are favorable, with 80% indicating that it will increase in volume and potential procedures. Thirty-one percent state that robot-assisted prostatectomy is standard of care, while 50% believe this procedure looks promising. Respondents think that optimal training in minimally invasive techniques is fellowships (23%), minifellowships (23%), or hands-on courses (23%). Twenty-nine percent think that they were trained adequately in laparoscopy and robotics from residency, and 62% believe residents should be able to perform most laparoscopic procedures on completion of residency.
Conclusions:
The practice and availability of laparoscopic and robotic procedures have increased since previous evaluations. Opinions regarding these techniques are favorable and optimistic. As the field of urology continues to see a growing demand for minimally invasive procedures, training of postgraduate urologists and residents remains essential.
Introduction
Materials and Methods
In the spring of 2009, an Internet survey was sent to practicing urologists with e-mail addresses that were registered with the American Urological Association (AUA). The survey, approved by the AUA Laparoscopy Committee, consisted of 31 questions (see Appendix). Two follow-up reminders were sent to persons who had not completed the questionnaire the following week, and the survey ended 2 weeks after initial invitations were sent. Results were collated and descriptive statistics calculated by the AUA Office of Education.
Results
Demographics
There were 9,095 survey invitations sent and 864 surveys were completed for a response rate of 9.5%. Table 1 lists respondent demographics. Results were well distributed for age, practice length, and AUA section, while sex was predominantly male. Respondents were mostly associated with partnerships or academic institutions.
More than one answer accepted.
AUA=American Urological Association.
Practice patterns of laparoscopy
The majority of respondents (84%) reported that laparoscopic or robot-assisted surgery is performed in their practice, with 56% devoting at least 5% of their practice to these procedures. Forty percent use multiple approaches, including conventional, hand-assist, or robot-assisted. As shown in Figure 1, the highest level of training obtained by the primary laparoscopists was fellowship (31%), residency (23%), or 2- to 3-day hands-on courses (22%). Table 2 describes referral patterns for those who do not practice laparoscopy/robotics. These respondents primarily refer patients to tertiary/academic centers (49%) or to another private urology practice (31%). Only 10% of those urologists indicate the surgery is instead performed in an open fashion. The main reason laparoscopy is not performed is because of lack of (38%) or limited training (39%).

Highest level of training achieved by the primary laparoscopist or robotic surgeon in practice.
Laparoscopic nephrectomy
Eighty-six percent indicate that laparoscopic nephrectomy occurs in their practice, with 68% reporting that the procedure was performed within the last 12 months. Nearly three-fourths of respondents plan on performing the procedure within the next 12 months, with 24% predicting more than 15 procedures in that time span. Seventy-one percent believe it is the standard of care, while 25% state the procedure looks promising. Laparoscopic donor nephrectomy is not performed in the majority of practices (81%), with most occurring at outside institutions (55%).
Percutaneous needle ablation
Fifty-two percent report performance of laparoscopic needle ablations and percutaneous ablations in their practice. Percutaneous ablation is performed by radiologists alone (49%) or in concert with urologists (40%), with only a few being performed by urologists alone (11%). The majority plan on performing fewer than five ablative cases within the next year (34%) or none at all (49%). Attitudes are favorable, with 68% stating that ablation looks promising.
State of robot-assisted surgery
Seventy-five percent of respondents' hospital/practice own at least one robotic unit (66%) or plan on purchasing one in the next year (9%). The highest level of robotic training achieved is fellowship (23%), 2- to 3-day hands-on course (20%), or residency (13%). Twenty-seven percent report no robotics training. As depicted in Figure 2, attitudes toward robotics are favorable, with 80% indicating that robotics will grow and increase in volume and potential procedures. A similar number (71%) believe that robotics is not a fad, and 45% report that robot-assisted procedures will become the standard of care within the next 10 years.
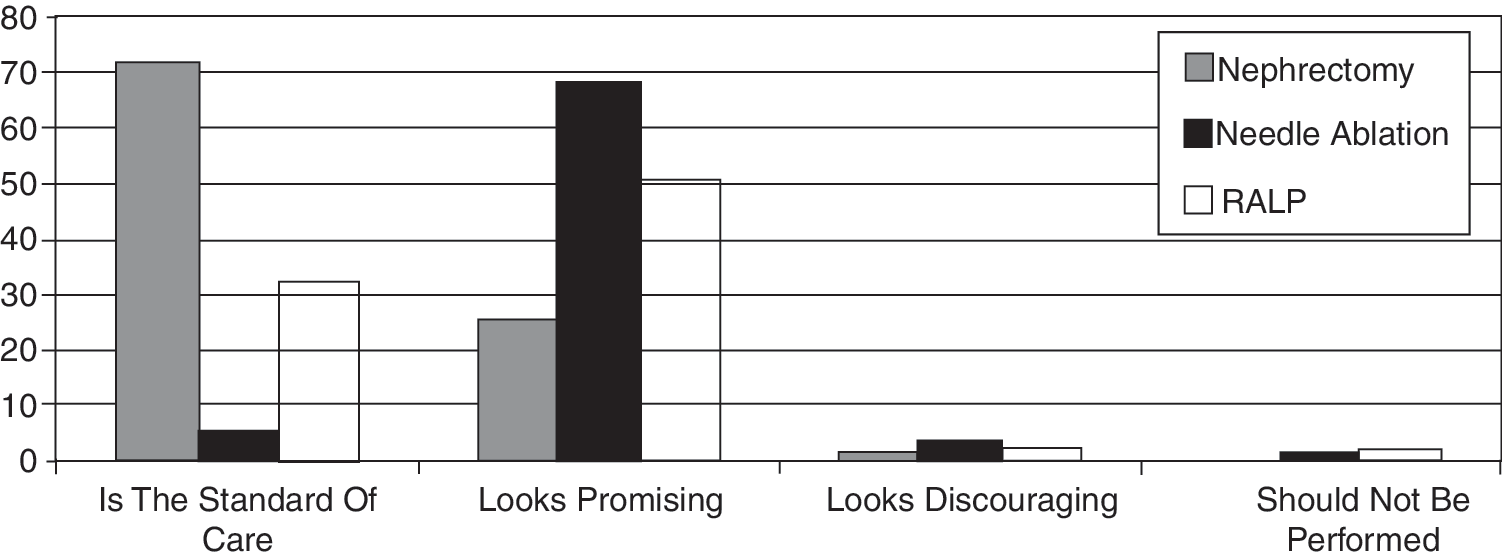
Practicing urologists opinions on the status and future of laparoscopic nephrectomy, laparoscopic needle ablation, and robot-assisted laparoscopic prostatectomy (RALP).
Robot-assisted laparoscopic prostatectomy (RALP)
Nearly two-thirds (65%) of respondents or someone in their practice has performed this procedure in the last 12 months. Nearly one-third (31%) state that it is the standard of care or looks promising (50%). Interestingly, 60% do not plan on performing the procedure within the next 12 months.
Additional laparoscopic/robotic procedures
More than one-third of urologists are performing laparoscopic and/or robotic-assisted partial nephrectomy, pyeloplasty, and/or renal cyst decortication. Laparoscopic adrenalectomy and pelvic lymphadenectomy are being performed by more than 25%.
Education and training
Most believe that optimal training in minimally invasive techniques comes from fellowships (23%), minifellowships (23%), or postgraduate hands-on courses (23%). Twenty-one percent rely on new partners to instruct or perform the procedure. Nearly two-thirds believe that virtual-reality simulators are of significant benefit in minimally invasive training. Twenty-nine percent think that they were trained adequately in laparoscopy, with more than half of persons stating that laparoscopy cases were either not performed (39%) or limited in number (24%) during their training. Only 6% thought their hands-on exposure was inadequate despite exposure to large caseloads during their training. Figure 3 depicts opinions on who should perform these procedures. Sixty-two percent believe that the majority of laparoscopic urologic procedures should be performed by residents trained in urology, while 42% indicate the majority of robot-assisted laparoscopic urologic surgery should be performed by residents in urology.

Opinions on who should perform the majority of laparoscopic or robot-assisted urologic surgery.
Discussion
This AUA survey was distributed to evaluate current minimally invasive practice patterns and training needs of postgraduate urologists. Specific objectives were to (1) obtain demographic profiles of respondents; (2) determine general practice patterns and attitudes regarding laparoscopic and robot-assisted urologic surgery; (3) investigate practice patterns that involve specific procedures, including laparoscopic nephrectomy, needle ablation therapy, and RALP; (4) assess the current and future state of robot-assisted surgery; and (5) assess attitudes regarding training and fellowship.
The total response rate for this study was 9.5%, with the sample size of 864 being accurate within 3.4% of the calculated 95% confidence interval for survey accuracy. Despite a relatively low response rate, our demographic data show a survey population that is well distributed in terms of practice type, length, and location. Because nearly 85% of respondents report that laparoscopic procedures are performed in their practice with nearly two-thirds containing a robotic unit, the current availability of laparoscopic and robot-assisted procedures within the practicing urologic community is the highest reported in the literature to date. 2,5,7 –9 Our data show that well over half of respondents are devoting more than 5% of their practice to laparoscopy, a number that has grown within the past decade. 7,9 The increased availability and devotion to minimally invasive surgery demonstrate the effects of changes in training exposure that have developed to meet the demand of this growing field.
The majority of those who do not perform laparoscopy refer patients to either tertiary/academic centers or to other urologists who perform these procedures. Past studies have established lack of or limited exposure during training as a common reason why minimally invasive procedures are not performed, 8 and we see similar responses from our sample population. Well-placed effort is currently being devoted to determining optimal training modalities both in and out of residency. Recent evaluation of residency training revealed laparoscopic and robotic training to be well integrated in training programs. 3 Our survey respondents acknowledge this, with the majority stating that most residents should be able to perform laparoscopic and robotic procedures by the end of their training. Many also state that practicing urologists should obtain additional hands-on training to familiarize themselves and feel more comfortable with minimally invasive techniques.
Postgraduate training in laparoscopy has come under scrutiny because the effects of various training modalities on minimally invasive urologic practices have been mixed to date. 4 –7 Whereas past investigation into the long-term impact of 2- to 3-day seminars showed decreased use of laparoscopy 5 years after postgraduate training, 5 recent study into week-long “mini”-robotic fellowships appear to have a positive impact on participants' minimally invasive practices on 3-year follow-up. 6 This type of training focuses less on didactic material and instead on providing multiple hands-on experiences, ranging from use of models and cadavers to observing and performing procedures on live patients. 1,6 Although more intensive training programs such as minifellowships appear promising as a way for postgraduate practitioners to familiarize themselves with minimally invasive surgery without a formal fellowship, the cost and accessibility of resources and teaching practitioners severely limits the availability of training programs such as these.
The prostate is a challenging organ to approach from a minimally invasive perspective because of its position deep within the pelvis. While laparoscopic prostatectomy was introduced in the United States in the early 1990s, it was not until the late 1990s that urologists in France proved its feasibility. The lack of adoption of this technique in the United States was primarily because of the steep learning curve that is associated with maneuvering in the pelvis using counterintuitive motion controls with limited degrees of freedom. 10 In our study population, only 3% report the use of pure laparoscopic prostatectomy in their practice. The introduction of RALP in 2001 allowed for greater visibility through three-dimensional magnification and a robotic wrist that mimics the degrees of freedom of a human wrist. This allowed for the successful transfer of open and laparoscopic skills to the robotic platform. 11 Since its introduction, the field of urology has seen rapid adoption of robotics as an accepted minimally invasive approach to prostatectomy and now sees expanding use geared toward disease processes in other organs. Current opinions and attitudes toward robotics as applied to RALP are favorable and quite optimistic in our study population; 45% of our population believe that it will become the standard of care, with the majority stating that the field of robotics will only continue to expand.
Training exposure remains a key influential element because past studies have shown its impact on future practice patterns. Shay and associates 2 demonstrated that persons trained in laparoscopy were more likely to perform laparoscopic procedures in postgraduate practice. When asked the highest level of training, 23% of practicing laparoscopists report their maximum level of training was obtained in residency compared with 13% of practicing robotic surgeons. Similarly, slightly more laparoscopists are fellowship trained compared with robotic surgeons in our respondents (31% vs 23%, respectively). These are not surprising findings, because one would expect a procedure that has been available for nearly twice as long to be better established in training programs. Recent study has shown the integration of robotics to be expanding within training institutions, with more than 50% of residency programs incorporating robotics into their curriculum 3 ; 46% of our respondents seem to acknowledge this, stating that most residents should be able to perform robotic procedures on completion of their training. Twice as many, however, believe that robotics should be performed by fellowship-trained urologists compared with laparoscopy. While this may indicate that some believe that residency training in robotics is in an early stage, these opinions will likely change with the progress that has been made in residency training within a brief period. With improvements in training, coupled with optimistic attitudes seen in our study, robotics has quickly come into the forefront of minimally invasive urologic surgery and has integrated itself into practice faster than laparoscopy did after its introduction nearly 20 years ago.
Our study has several limitations that warrant mention. Our response rate was relatively low compared with other laparoscopic survey studies whose rates ranged from 15% to 60%. 3,5,7 –9 Potential causes include the two-week availability of the survey, the number of questions comprising the survey, or the use of the Internet to distribute the questionnaire. The fully electronic nature of this questionnaire may introduce bias to those who regularly use e-mail. These persons may be more likely to embrace technology and answer questions favorably regarding technology-driven procedures. Because our study focuses on American urologists only, differences in availability of these technologies in the United States may result in practice patterns and opinions that are not representative of urologists who practice in other countries. Further devoted investigation into international practice patterns and opinions are needed to better address this topic.
The survey targets practice patterns regarding specific methods of treatment, so those who actively perform these procedures may be more inclined to respond as shown by the relatively high number (31%) of primary laparoscopists in the group with fellowship training. Similarly, the age and differences in time out from training in our respondents who participated in our study may have influenced our results. Our survey construct did not allow further statistically meaningful subanalysis of this issue. To more accurately assess the influence of age and time on training on opinions and practice patterns, additional focused studies are needed. With 916 da Vinci® robotic consoles available in the United States, this possible selection bias is further supported by the fact that two-thirds of urologists report access to a robotic platform. 12 This positive bias, coupled with the large nonresponse rate and strong representation from younger urologists associated with academia likely has resulted in an overestimation on the current use of laparoscopic and robotic surgery in urology.
Conclusions
Minimally invasive urologic practice patterns have expanded since previous evaluations. The availability and practice of laparoscopy and robotics have increased, and current attitudes regarding these treatment modalities are more favorable and optimistic. As the field of urology continues to see a growing demand for minimally invasive procedures, practice patterns must continue to evolve. This can be accomplished through continued focus on increasing training exposure for urologists and residents and the development of scientifically validated simulators for training, practice, and evaluation.
Footnotes
Acknowledgments
The AUA Laparoscopy and Robotic Surgery Committee (Janice Baum, Jeffrey A. Cadeddu, Allen M. Chernoff, Matthew D. Dunn, Inderbir S. Gill, Anil Kapoor, Louis R. Kavoussi, Jaime Landman, Ravi Munver, Stephen Y. Nakada (Chair), John L. Phillips, Richard D. Scott, Steven J. Shichman, R. Ernest Sosa, Chandru P. Sundaram, Robert M. Sweet, Raju Thomas, Howard N. Winfield) provided guidance and contributed to this study, and Todd Carrick assisted with statistical analysis.
Disclosure Statement
No competing financial interests exist.