
Abstract
Purpose:
To compare the perioperative and oncologic outcome between hand-assisted nephroureterectomy (HARNU) and transurethral bladder cuff incision-assisted nephroureterectomy (TUINU), which manage the bladder cuff with different methods.
Patients and Methods:
From January 2005 to December 2008, 325 patients with upper urinary tract urothelial carcinoma (UUT-UC) underwent nephroureterectomy at our institution. A total of 208 patients were enrolled in this retrospective study.
Results:
A total of 208 patients, including 102 men and 106 women, were analyzed in this retrospective study. Ninety-eight patients underwent HARNU for UUT-UC, and110 patients underwent TUINU. The HARNU group has less operative time and hospital stay, and fewer postoperative ileus episodes. There were trends of less blood loss in the HARNU group. There were no statistical differences in the total bladder tumor recurrence, local recurrence, contralateral recurrence, distant metastasis, and cancer-specific survival between HARNU and TUINU. There was a significantly higher incidence of bladder tumor recurrence in TUINU group, however, than in the HARNU group (P=0.008) if the tumor was located at the low third of the ureter.
Conclusion:
There were more oncologic concerns about bladder tumor recurrence for the low third ureteral tumor in the TUINU group. In addition, the perioperative outcomes such as operative time, blood loss, hospital stay, and ileus rate were better in the HARNU group. Therefore, surgeons can manage UUT tumor with less oncologic concern and better perioperative results with HARNU.
Introduction
There is no detailed comparison in oncologic outcomes, however, between HARNU and TUINU that have only one incision wound. HARNU and TUINU for bladder cuff management have been used at our institution; hence, analysis of perioperative and oncologic outcomes by cohort study was reasonable.
Patients and Methods
Patients
From January 2005 to December 2008, 325 patients with UUT-UC underwent nephroureterectomy at our institution. Ninety-seven patients were excluded because of having received treatments that were two-incision, extended lumbodorsal, midline nephroureterectomy, bilateral nephroureterectomy, or nephroureterectomy with cystectomy. Patients who have a larger low ureteral tumor with intravesical invasion were selected for two-incision, extended lumbodorsal, midline nephroureterectomy. The other 20 patients were excluded because of pT4 disease. A total of 208 patients were enrolled in this retrospective study.
Nephroureterectomy was performed either by HARNU or TUINU to manage the bladder cuff (Fig. 1). Patients who could afford to pay for retroperitoneoscopic instruments were arranged to undergo HARNU; the others underwent TUINU.

Surgical techniques
In the HARNU technique group (Fig. 2), patients were placed in a semioblique position. 3 A Gibson incision was made as an access for the surgeon's hand. One 10-mm long trocar insertion was made for retroperitoneoscopy on the suprailiac crest along the midaxillary line; the other 12-mm long trocar insertion was made for an operative or suction instrument on the subcostal area along the posterior axillary line.

Hand-assisted retroperitoneoscopic nephroureterectomy. Low ureter was ligated as low as possible through the Gibson wound, and then the surgeon performed a hand-assisted retroperitoneoscopic nephrectomy with open bladder cuff excision.
After dissecting the retroperitoneal space, the distal ureter was first identified and then ligated as low as possible to prevent tumor spreading. Two trocar insertions were made under manual guidance in the retroperitoneum through the Gibson incision. The operating table was then rotated to place the patient in a true lateral position. After ligation of the renal pedicle by an Endo-GIA stapler, two to three Deaver retractors were used to expose the bladder cuff thoroughly and enable performance of excision with a harmonic scalpel. The final step was use of the catgut suture or to secure the bladder cuff.
In the TUIINU method group (Fig. 3), patients were initially placed in the lithotomy position. Transurethral bladder cuff circumferential incision (TUI) to the perivesical fat was performed with a Collings knife. The ureteral orifice opening was electrocoagulated to prevent tumor spreading. After the TUI procedure, a Foley catheter was placed for urinary drainage and urine extravasation prevention during the operation. The patient was then turned to the lateral decubitus position. A flank incision was made to complete the nephrectomy after ligation of ureter as low as possible, and the whole ureter was stripped manually. The entire bladder cuff was removed and examined after stripping of the ureter.

Transurethral bladder cuff incision-assisted nephroureterectomy. The surgeon performed a transurethral incision of the bladder cuff first. A flank incision was then made to complete the nephrectomy, and the whole ureter with bladder cuff was stripped manually.
Tumor staging, follow-up, and outcome statistics
All patients who were undergoing nephroureterectomy received preoperative and postoperative CT imaging as well as regular fibercystoscopic examination. Fibercystoscopy was performed every 3 months for the first 2 years. CT imaging was performed annually to assess local recurrence or regional lymph node status. Pathologic staging was recorded as the 2002 Tumor-Node-Metastasis staging system, and tumor grade was classified according to the 1998 World Health Organization classification. Tumor location and histologic type were obtained from pathologic records.
SPSS v.17 software was used for statistical analysis. The distribution of these two groups and comparison of perioperative quantitative data was conducted with chi-square test or two sample t test; recurrence-free, distant metastasis, or cancer-specific survival duration was estimated by the Kaplan-Meier method with log-rank test. Patients who had previous bladder tumors were excluded for evaluation of bladder recurrence. The results were statistically significant if P<0.05.
Results
This retrospective study enrolled 208 patients, including 102 men and 106 women. Average age was 66.30±10.51 years, and median follow-up duration was 26.7 months. The detailed characteristics regarding smoking history, tumor location, tumor number, postoperative stage, and tumor grade are listed in Table 1. Most patients received a diagnosis of renal pelvis tumor (75.96%). Ureteral tumor locations in the upper, middle, and low ureter were 17.79%, 12.98%, 15.87%, respectively. Stage distribution in this study revealed 57.21% pTa/pTis/pT1, 18.27% pT2, and 24.52% pT3 disease. Patients with pT4 disease were excluded in this study. The follow-up duration, smoking history, tumor number, postoperative stage, and tumor grade showed no significant difference between these two groups. There were fewer low ureteral tumors in the TUINU group compared with the HARNU group.
HARNU=hand-assisted nephroureterectomy; TUINU=transurethral bladder cuff incision-assisted nephroureterectomy.
Ninety-eight patients underwent HARNU, and 110 patients underwent TUINU for UUT-UC. Median follow-up duration for the HARNU group was 25.28 (2.17∼64.7) months and 27.88 (0.17∼62.6) months for the TUINU group. The perioperative data, such as operative time, blood loss, hospital stay, and postoperative ileus incidence are listed in Table 2. The HARNU group had less operative time, hospital stay, and postoperative ileus episodes (P=0.006, P<0.0001, P<0.016, respectively); this group also had a trend of less blood loss (P=0.09).
HARNU=hand-assisted nephroureterectomy; TUINU=transurethral bladder cuff incision-assisted nephroureterectomy.
Furthermore, this study also analyzed the total oncologic outcomes, which are listed in Table 3. Total bladder tumor recurrence rate was 27.88 % (26.53% in HARNU and 29.09% in TUINU, respectively); pelvic local recurrence rate was 5.29 % (5.1% in HARNU and 5.45% in TUINU, respectively); contralateral recurrence rate was 5.77% (7.14% in HARNU and 4.55% in TUINU, respectively); and distant metastasis rate was 12.02 % (13.29% in HARNU and 10.00% in TUINU, respectively). No significant difference existed in recurrence or metastasis between these two groups. In addition, cancer-specific death (6.12% in HARNU and 8.18% in TUINU, respectively) also revealed no difference in patients undergoing either HARNU or TUINU.
Patients with previous bladder tumor were excluded.
HARNU=hand-assisted nephroureterectomy; TUINU=transurethral bladder cuff incision-assisted nephroureterectomy.
Kidney tumor, upper/middle ureteral tumor, and low ureteral tumor were further identified in each group (Table 4). Higher rate of bladder tumor recurrence in the TUINU group (P=0.008) was noted if the tumor was located at the lower third of the ureter (Fig. 4). No difference in pelvic local recurrence, however, was observed between these two groups when tumor location was considered.
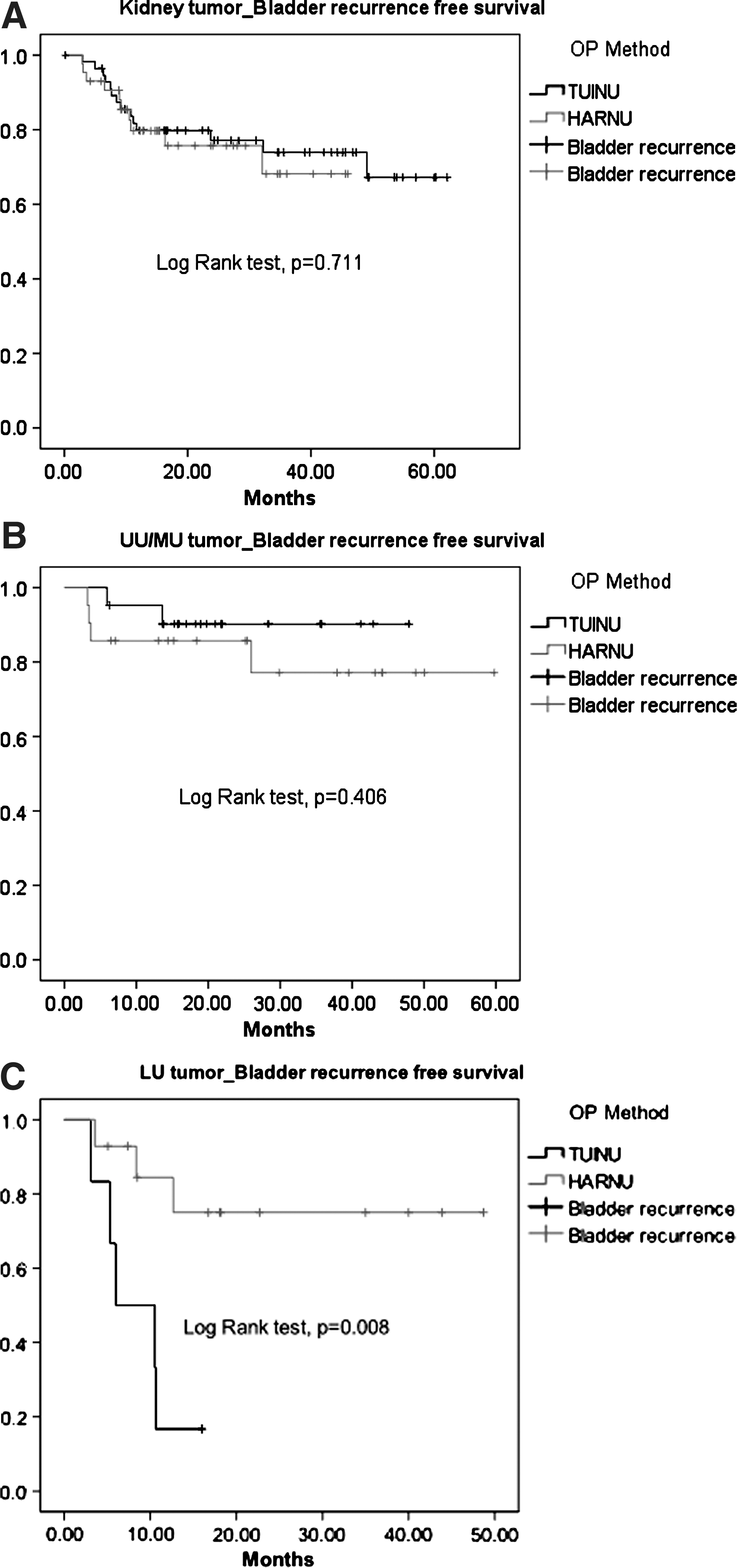
Patients with previous bladder tumor were excluded.
Patients with multiple tumor sites were excluded.
HARNU=hand-assisted nephroureterectomy; TUINU=transurethral bladder cuff incision-assisted nephroureterectomy; UU=upper ureter; MU=middle ureter; LU=low ureter.
Discussion
Nephroureterectomy with bladder cuff excision is standard surgical intervention for patients with UUT-UC. Many minimally invasive procedures have been developed in which transperitoneal or retroperitoneal methods were used. According to the literature reviewed, however, the incidence of ileus after use of the transperitoneal approach ranged from 5% to 17% 5 –7 while the incidence of incisional hernia was reported up to 7.6%. 8 Retroperitoneal approaches were used to prevent gastrointestinal morbidities. Retroperitoneal nephroureterectomy could be divided into the two-incision method, extended lumbodorsal method, retroperitoneoscopic method, and the TUI-assisted method. The rate of ileus is only 2.04% in the HARNU group and 10% in the TUINU group. To minimize wound-related morbidities, HARNU and TUINU were used for patients with UUT-UC at our institution.
Previous studies have indicated that the bladder recurrence rate after nephroureterectomy was 15% to 55%, pelvic local recurrence rate was 0% to 25%, and contralateral recurrence rate was around 5% to 11%. 9 –13 It is thought that management of the bladder cuff was associated with local or residual ureteral stump recurrence, and tumor seeding was related to bladder recurrence. The traditional open surgery is the two-incision method (flank incision and Gibson wound), which causes more postoperative pain and delayed recovery. Use of the endoscopic method to perform bladder cuff excision was first presented by McDonald and associates, 14 and several minimally invasive surgical approaches either by laparoscope or transurethral endoscope were developed. 3,15
Hand-assisted laparoscopic nephrectomy was first introduced in 1997. 16 This method was widely accepted and further applied to not only surgical intervention of urothelial tumor but also living donor renal transplantation. 4,17 We have proposed the modified method by gasless hand-assisted retroperitoneoscopic removal of the kidney, ureter, and bladder cuff since 2005. 3 The Gibson incision of HARNU enhances the early control of the distal ureter and provides an easier approach for bladder cuff excision. Another two trocar incisions could complete the nephroureterectomy with low abdominal Gibson incision. 3
Although the above mentioned two methods have changed nephroureterectomy from two-incision to one-incision, the perioperative and oncologic outcome with adequate follow-up duration have not been reported. Early return of ambulation and oral intake are advantages of HARNU. 18 Analysis of the perioperative data in the study indicated that the HARNU group presented with less operative time, hospital stay, postoperative ileus episodes, and blood loss. Changing position during the operation is unnecessary in this group, and this may shorten the operative time. Less incision length (fit with surgeon's hand width) could reduce wound pain; lower position of the wound may enhance chest care and shorten length of hospital stay.
The bladder cuff wound was sutured with catgut or secured with Endoloop in the HARNU group. No suture of the bladder cuff was performed in the TUINU group, however. Therefore, the Foley catheter and pelvic drain could be removed 1 day after surgery in the HARNU group. The supposition is that focal urinary extravasation would cause peritoneum irritation, resulting in more ileus incidence in the TUINU group. Harmonic scalpel was used to excise the bladder cuff in the HARNU group, and a better result of hemostasis was observed.
Hetherington and colleagues 19 indicated that the major concern regarding TUINU is bladder recurrence and local retroperitoneal recurrence. Hence, HARNU was designed to ensure that the bladder cuff is excised under visual guidance without the risk of residual ureteral stump and early control of the distal ureter for tumor spillage. Previous studies stated neither differences on bladder and pelvic recurrence between open cystotomy and transurethral incision of bladder cuff, 2,4 nor specific mention of the risk of low ureteral tumor spreading between TUI and the open method. The experience at our institution showed that there is no difference in total bladder and pelvic local recurrence between the TUI method of TUINU and the open bladder cuff excision of HARNU.
TUINU had a higher incidence of bladder tumor recurrence, however, if the tumor was located at the lower third of the ureter. We supposed that ligation of the distal ureter as low as possible from the tumor lesion during the HARNU or TUINU procedure in our cases prevented tumor spreading if the tumor was located above the middle ureter; nevertheless, this method seemed not to control low ureteral tumor adequately in the TUINU group.
It is also worth noting that 52 of 97 patients who were excluded from this study were shifted from TUINU to two-incision, extended lumbodorsal, or midline nephroureterectomy because of low ureteral tumor. In addition, fewer patients with low ureteral tumor in the TUINU than in HARNU group (10.90% and 21.43%, respectively, P=0.038) were observed in the study. To perform perfect bladder cuff excision or nearly partial cystectomy in the cases of distal ureteral tumor, TUINU is not recommended. On the contrary, it is not contraindicated in the HARNU procedure.
This retrospective study provides the largest series to compare perioperative and oncologic outcome between the HARNU and TUINU procedures for such an unusual UUT tumor. Some series indicated that the length of postoperative tumor recurrence was short. According to results from 1363 patient-pool experiences in 12 centers, 10.4 months for cancer recurrence after radical nephroureterectomy was reported. 20 Approximately 7.7 to 12 months for cancer recurrence was reported after laparoscopic nephroureterectomy. 21,22 Our results revealed that the median duration for bladder and local recurrence is 7.05 and 13.07 months after radical nephroureterectomy. We believe that the median follow-up duration (26.7 months) in this series could provide reasonable experience for observation of bladder and local recurrence.
Although our study showed no difference in pelvic local recurrence between HARNU and TUINU, it is necessary to have a larger number of cases for adequate analysis to see whether endoscopic or open bladder cuff excision would influence the pelvic local recurrence rate according to different tumor location.
There were still several limitations in this study. It is possible there was selective bias in the patients with low ureteral tumors. Surgeons may shift TUINU to HARNU, two-incision, extended lumbodorsal, and midline nephroureterectomy for low ureteral tumor to make perfect distal ureter management and bladder cuff excision. The patient numbers with low ureteral tumor are relative low to make a definite conclusion. It should be validated by more case accumulation or multicenter experience concerning the oncologic impact of bladder cuff management in low ureteral tumor.
The technique used to prevent tumor seeding in the TUINU is electrocauterization of the bladder cuff and early ligation of the ureter distal from the tumor lesion at our instution. More precise bladder cuff control such as Endoloop ligation from the transvesical port may lead to a different outcome. 23 In addition, nephroureterectomy could be performed by a different combination of nephrectomy and bladder cuff management.
Only retroperitoneal approaches instead of a pure laparoscopic method were discussed in this article. Further prospective studies with different approaches are necessary for validation of our findings.
Conclusion
There is a higher incidence of bladder tumor recurrence for the low third ureteral tumor in the TUINU group. In addition, the perioperative outcomes, such as operative time, blood loss, hospital stay, and ileus rate, were better in the HARNU group. With the aforementioned data, we concluded there was more oncologic concern for low ureteral tumor by TUI bladder cuff management. A surgeon should pay more attention over bladder cuff management to prevent bladder recurrence for nephroureterectomy combined with the TUI method. HARNU is a safe and effective techinique to manage a UUT tumor with less oncologic concern and better perioperative results in our experience.
Footnotes
Disclosure Statement
No competing financial interests exist.