
Abstract
A secure and hemostatic renorrhaphy is the primary challenge of minimally invasive nephron-sparing surgery (MINSS). The laparoscopic surgeon's ability to maintain constant tension on the suture while oversewing the transected parenchyma and collecting system is difficult, even when using robotic technology. A self-retaining barbed suture (SRBS) is a recent innovation that maintains tissue apposition and tension using a novel “self-cinching” mechanism. We describe our technique for SRBS use during MINSS. In our experience, the use of SRBS in this setting is safe and improves suturing efficiency during the time constraint of warm ischemia. We believe that intracorporeal suturing with SRBS during MINSS may help shorten the learning curve associated with this technically challenging step and have adopted it in our standard practice.
Introduction
A complementary approach to improving suturing efficiency during minimally invasive partial nephrectomy is innovation in suture design. Murtha and colleagues 10 recently described the use of self-retaining barbed suture (SRBS) in wound closure during plastic surgery procedures. This absorbable suture contains unidirectional barbs along its shaft that deploy and anchor as the suture is pulled through tissue, maintaining tension of the suture line and eliminating the need for slack management or knot tying (“self-cinching” mechanism) (Fig. 1). In a preclinical study that evaluated the use of SRBS during porcine LPN, Shikanov and associates 11 found that it performed equivalently to absorbable polyglactin suture in vascular and collecting system repair of the renal defect. Since July 2009, we have used SRBS (V-Loc™ 180; Covidien, Mansfield, MA) clinically during minimally invasive partial nephrectomy and describe our surgical technique.

Self-retaining barbed suture.
Technique
Patient preparation
All patients undergo bowel preparation with magnesium citrate on the day before surgery. For LPN, the patient is placed in a partial flank position with the anterior superior iliac spine over the table break. The table is flexed and placed in a slight Trendelenburg position to maximize the distance between the costal margin and the pelvic girdle. The ipsilateral arm is secured in a neutral, flexed position over the chest. For robot-assisted laparoscopic partial nephrectomy (RALPN), the patient is similarly placed in lateral flexion as above, but the ipsilateral arm is secured in a neutral, straight position to the patient's side, to accommodate docking of the robot arms (Fig. 2).

Patient positioning for robot-assisted laparoscopic partial nephrectomy.
Port placement
We use the transperitoneal approach in all cases. After insufflation of the abdomen, a 12-mm periumbilical Visiport™ (Covidien, Mansfield, MA) trocar is inserted. A total of three additional ports are placed: 12-mm ports in the ipsilateral upper and lower quadrants, subcostal along the midclavicular line, and inferolateral to the umbilicus along the anterior axillary line, respectively. Before hilar occlusion, an additional 12-mm suprapubic port is inserted for insertion of the laparoscopic Satinsky clamp. For RALPN, after insertion of a periumbilical camera port, 8-mm robotic ports are placed in the upper and lower quadrants as described above. Two 12-mm assist ports are then inserted along the midline, one midway between the umbilicus and xiphoid, and the second in the suprapubic region. For right-sided procedures, a 3-mm liver retractor is used.
Surgical technique
With a 30-degree down lens, medial reflection of the colon and abdominal viscera, including Kocherization of the duodenum for right-sided procedures, is performed. The ureter and renal hilum are identified and mobilized. The Gerota fascia is incised longitudinally, and the kidney is fully mobilized within the Gerota fascia to facilitate both tumor excision and subsequent repair of the defect. Intraoperative laparoscopic ultrasonography is used to aid in the identification of the tumor and in the demarcation of its margins.
Before the tumor is resected, three 3-0 V-Loc sutures, each anchored with a single Lapra-Ty™ (Ethicon, Cincinnati, OH) clip at the tail end, and three oxidized cellulose bolsters are preplaced in the abdomen. After intravenous infusion of 12.5 g mannitol, the renal hilum is cross-clamped en bloc using a Satinsky clamp during LPN, or two laparoscopic bulldog clips during RALPN. The mass is then sharply excised with cold scissors, placed in an Endocatch™ bag (U.S. Surgical Inc, Norwalk, CT), and retained in the abdomen pending completion of the procedure. The V-Loc sutures are used in a running closure of the resection bed, oversewing transected blood vessels and, if necessary, the collecting system. Tension on a suture line is maintained by cinching up on the suture after each bite (Fig. 3). The final bite is brought out through the renal capsule, and the needle is retrieved.
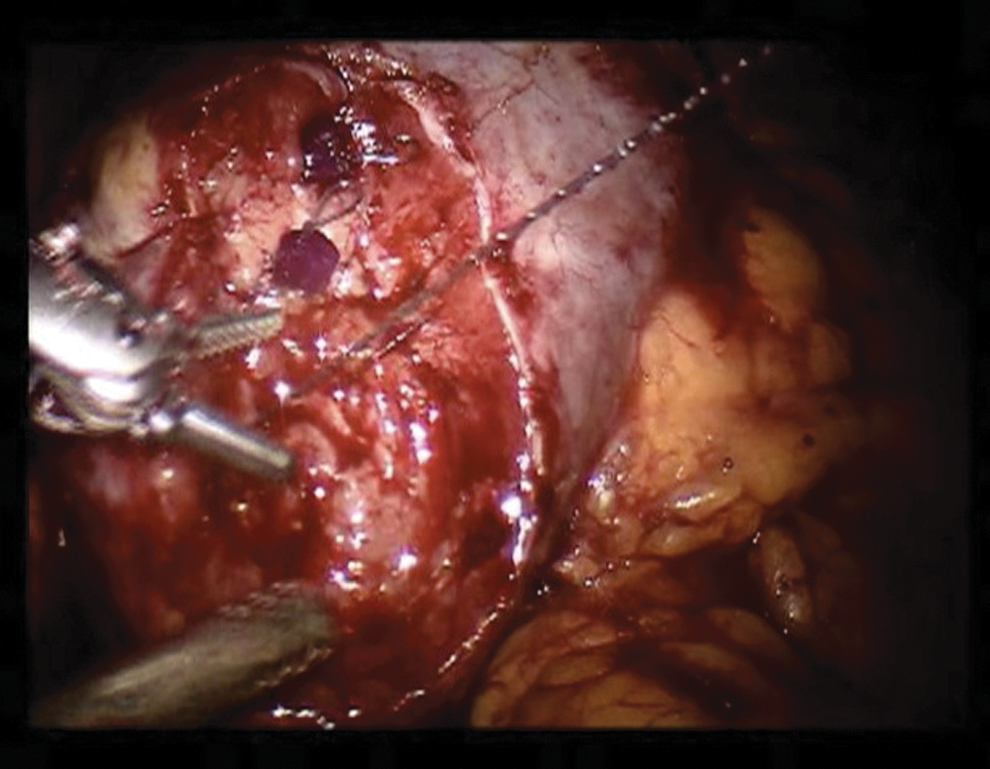
Parenchymal repair using the self-retaining barbed suture.
Gelatin/thrombin hemostatic matrix is applied to the resection bed, following which sliding-clip renorrhaphy 8 over oxidized cellulose bolsters is performed, using 0-polyglactin suture on a CT-1 needle. The hilum is unclamped, and the resection bed is inspected for hemostasis. After verifying adequate hemostasis, the cut edges of the Gerota fascia are reapproximated using 10-mm Hem-o-lok clips. If collecting system repair is needed, a 19F round drain is secured in the perinephric space. All ports are removed under direct vision. The specimen is extracted via the periumbilical port, and the fascia is closed.
Instruments/equipment
For LPN: - Visiport trocar - Three 12-mm trocars - Laparoscopic cautery scissors - Laparoscopic wide-mouthed graspers - Laparoscopic suction/irrigator device - Hem-o-lok clip appliers; 5-mm and 10-mm - Laparoscopic ultrasound - Laparoscopic Satinsky clamp - Laparoscopic needle drivers×2 - Lapra-Ty clip applier and clips - 3-0 V-Loc 180 sutures - 0-polyglactin suture on a CT-1 needle
For RALPN: - Visiport trocar Two 12-mm trocars - Two 8-mm robotic trocars - Robotic Maryland bipolar grasper - Robotic Pro-grasp/Cadiere graspers - Laparoscopic suction/irrigator device - Hem-o-lok clip appliers; 5-mm and 10-mm - Laparoscopic ultrasound - Laparoscopic bulldog clip-applier (for application and removal) - Straight and curved laparoscopic bulldog clips - Robotic 8mm needle drivers×2 - Lapra-Ty clip applier and clips - 3-0 V-Loc 180 sutures - 0-polyglactin suture on a CT-1 needle
Role in Urologic Practice
In our experience, the use of SRBS for parenchymal repair during minimally invasive partial nephrectomy is safe and efficient. By eliminating the need for maintenance of suture line tension using the nondominant hand, intracorporeal knot tying, or Lapra-Ty clip anchoring, the ease and speed of suturing the tumor bed laparoscopically during the time constraint of warm ischemia are greatly enhanced. Indeed, in our preliminary experience, the use of SRBS during LPN was found to be associated with a significant decrease in warm ischemia time and a trend toward fewer postoperative bleeding interventions (article in press). We believe that for less experienced minimally invasive kidney surgeons, SRBS use during LPN or RALPN may be particularly advantageous with regard to shortening the learning curve that is associated with intracorporeal suturing, while for more experienced surgeons, it may help with shortening warm ischemia times.
The incremental procedure costs incurred by substituting polyglactin for V-Loc 180 suture are negligible. A 3-0 V-Loc 180 suture costs $23.65, while a 2-0 polyglactin suture costs $4.25. 12 Given that fewer Lapra-Ty clips, at an estimated cost of $9.06 per clip, are needed when SRBS is used, however, a per-case increase in cost of no more than approximately $30.00 can be expected. We believe that this marginal increase in cost is additionally offset by the advantages mentioned above, resulting in a net cost benefit over several cases.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.