
Abstract
Objectives:
To assess the compliance of endourologists with radiation safety measures and to determine the prevalence of orthopedic complaints among practicing endourologists.
Methods:
An Internet-based survey was sent to all members of the Endourological Society. Baseline characteristics on practice patterns (geographical region, age, years of practice, days per week of endourology, and number of cases in the previous year), compliance with various radiation protection measures (thyroid, chest and pelvic shields, gloves, glasses, and dosimeters), and prevalence of various orthopedic complaints (neck, back, hand, and joint problems) were assessed. Furthermore, open-ended questions assessed reasons for noncompliance.
Results:
Out of 160 surveys returned, 24 were excluded because of incomplete data. There was good compliance with chest and pelvic shields with 97% of endourologists reported wearing these. However, compliance with thyroid shields was only 68%. Furthermore, only 34.3%, 17.2%, and 9.7% of endourologists reported using dosimeters, lead-impregnated glasses, and gloves, respectively. Overall, 86 (64.2%) respondents complained of orthopedic problems. Specifically, 51 (38.1%) complained of back problems, 37 (27.6%) neck problems, 23 (17.2%) hand problems, and 19 (14.2%) complained of hip and knee problems. The prevalence of orthopedic complaints was significantly higher among African endourologists, older endourologists (>40 years), longer duration of practice (>10 years) and combined annual caseload of ureteroscopies (URS) and percutaneous nephrolithotomies (PCNL).
Conclusions:
Compliance in the use of thyroid shields, dosimeters, and lead-impregnated glasses and gloves could be improved. Orthopedic complaints among practicing endourologists are common and correlate with the annual caseload of combined URS and PCNL.
Introduction
Recent studies on interventional radiologists who wear heavy lead aprons demonstrated high prevalence of axial skeletal disease and orthopedic problems, particularly those relating to spine. 1,7,8 For interventional cardiologists, spine problems were reported in 42% and correlated with annual procedural caseload and number of years in practice. 2 In fact, “interventionalist disc disease” was found in 17.4% of interventional cardiologists and correlated with the use of heavy lead aprons. 9 However, there is no data on compliance of endourologists with radiation safety measures or on consequences of using such heavy protective gear. Therefore, the aim of the present study was twofold: to assess the compliance of endourologists with radiation safety measures and to determine the prevalence of orthopedic complaints.
Methods
An Internet-based survey was sent to all members of the Endourological Society (Appendix 1). The Web site remained open for 6 weeks (November 1 till December 15, 2010) to allow members an opportunity to visit and complete the online survey. Baseline characteristics on practice patterns (geographical region, age, years of practice, days per week of endourology, and number of cases in the previous year), compliance with various radiation protection measures (thyroid, chest and pelvic aprons, gloves, glasses, and dosimeters), and prevalence of various orthopedic complaints (neck, back, hand, and joint problems) were assessed (Appendix 1). Furthermore, open-ended questions assessed specific orthopedic complaints and reasons for noncompliance with radiation safety measures.
Data were analyzed using the commercially available SPSS for windows version 17 (Chicago, IL). Descriptive data were presented in terms of number of responses, percentages, ranges, and medians. Fisher's exact test was used for comparing discrete variables, whereas the nonparametric Mann–Whitney U-test was used for non-normally distributed continuous variables with significance defined as two-tailed p<0.05. Factors with significant impact on orthopedic problems by univariate analysis were further analyzed in multivariate analysis using general linear model.
Results
There were 160 respondents within 6-week period from November 1 to December 15, 2010. Twenty-four responses were excluded for having incomplete answers, so that complete data were available for 134 respondents. Most of the endourologists were located in North America, Europe, and Africa (45%, 22%, and 20%, respectively; Table 1). Furthermore, most endourologists were 40–60 years old (63.4%), practiced 10–20 years (37.3%) with 2–3 days/week of endourology (65.9%) (Table 1).
URS = ureteroscopy; PCNL = percutaneous nephrolithotomy; RGUG = retrograde urography, SWL = shock-wave lithotripsy.
There was a wide range of endourology caseloads with a minority of endourologists performing high volume of cases; thus, the data had positive skewed distribution. Therefore, medians together with ranges rather than means and standard deviations are reported. Furthermore, Mann–Whitney U-test was performed to compare groups.
Over the last 12 months of practice, the respondents performed a median of 60 ureteroscopies (URS), 25 percutaneous nephrolithotomies (PCNL), 40 retrograde urograms (RGUG), and 27 shock-wave lithotripsies (SWL) (Table 1).
With regard to radiation protection measures, there was good compliance with chest and pelvic shields (97%). However, only 68% wore thyroid shields. There was noncompliance with the use of dosimeters and lead-impregnated glasses and gloves with only 34.3%, 17.2%, and 9.7% reporting their use, respectively. Forty-nine respondents provided several reasons for lack of compliance with radiation protection measures. Unavailability was reported by 81.6% of noncomplaint endourologists. Surprisingly, 36.7% of noncomplaint respondents reported carelessness and denied the harmful effects of radiation exposure. Lack of knowledge about radiation hazards and the proper measures of protection was reported by 10.2%. Another 26.5% cited discomfort and heaviness of lead aprons as reasons for noncompliance. Finally, 22.4% “tried” to avoid radiation exposure by minimizing fluoroscopy times.
Surprisingly, 86 (64.2%) endourologists complained of orthopedic problems. Back, neck, and hand problems were reported by 51 (38.1%), 37 (27.6%), and 23 (17.2%), respectively. Nineteen (14.2%) endourologists complained of hip, knee, or ankle problems. The incidence of back and hand problems were significantly higher among African endourologists (p=0.01) (Table 2). Neck, back, and hand problems were significantly higher among older endourologists (Fig. 1). Similarly, neck and back problems increased significantly with years of practice (Fig. 2). However, the number of endourology days per week did not correlate with orthopedic complaints (p>0.05).
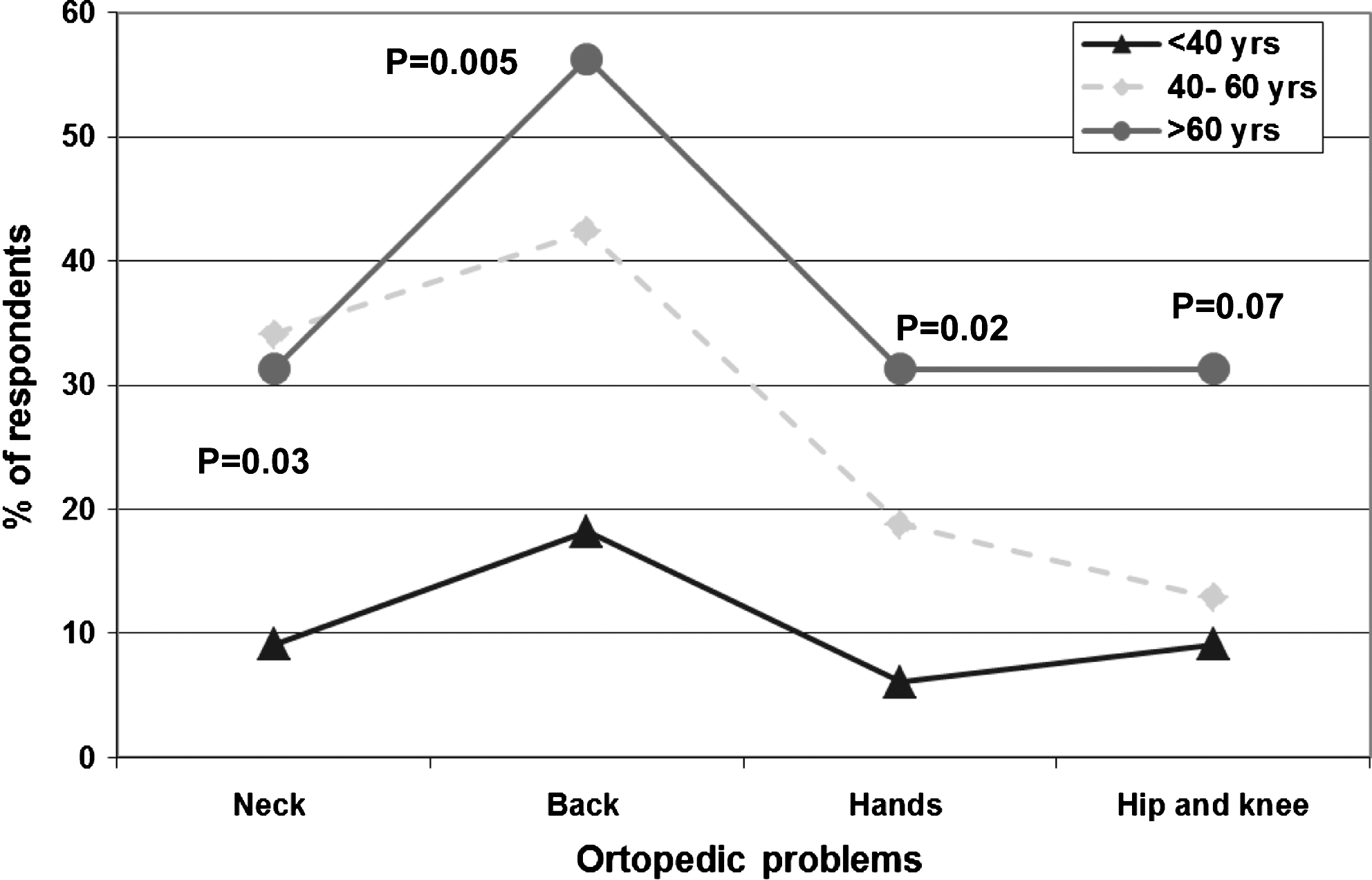
Orthopedic problems stratified by age (years).

Orthopedic problems stratified by the duration of practice (years).
When questioned about specific orthopedic problems, these were the responses obtained: For back problems; chronic intermittent backache, lumber disc prolapse, and lumber spondylosis were reported. For neck problems; recurrent pain, stiffness, cervical spondylosis, and cervical disc prolapse were reported. Hand and knee joints were affected by hand tremors, arthritis, and intermittent pain. About 7% of the respondents had multiple orthopedic problems in the form of recurrent painful joints with rigidity.
On univariate analysis, all orthopedic complaints significantly correlated with the annual combined caseloads of URS and PCNL (p<0.01 for all variables), whereas neither SWL nor RGUG showed any significant correlations with orthopedic complaints. On multivariate analysis, the combined annual caseloads of URS and PCNL maintained its significant correlation with all orthopedic complaints (p=0.001) except for hand problems (p=0.68).
Discussion
Although there are no prospective studies examining the amount of radiation exposure that urologists are exposed to on annual basis, urologists may be exposed to up to 0.1 mSv radiation per case of PCNL. 10 Furthermore, there are no previous published reports on compliance of radiation safety measures among urologists. In the present Internet-based survey of endourologists, there was good compliance with chest and pelvic shields. In a recent survey of California radiologic technologists, there was 70.5% compliance with personnel safety practices. 11 This is similar to the 68% compliance with thyroid shields found in the present study. It is still better than 4% compliance with thyroid shields reported in one orthopedic study. 12 Thyroid shields are important since they have been shown to decrease radiation exposure to the thyroid by 23 times down to background levels, thus reducing the risk of thyroid cancer. 13 Although a cluster of thyroid cancers among Australian orthopedic surgeons was reported, epidemiologic studies especially of urologists and radiologists are lacking. 14 In the present study, 9.7% of respondents reported using lead-impregnated gloves. Although cumbersome, in one study lead-impregnated gloves reduced radiation exposure to hands by 75%. 15 In the present study, only 17.2% of respondents reported using lead-impregnated glasses. Recent studies have shown that cataracts may develop at much lower radiation exposures than previously thought. 16 –18 Therefore, better compliance with radiation safety measures is encouraged among endourologists.
On the other hand, wearing heavy and uncomfortable personal protective lead aprons has been associated with orthopedic injuries. 19 In fact, wearing a 15-pound (6.8-kg) lead apron can apply pressures of 300 lbs (136 kg)/square inch on the intervertebral discs. 20 In the present study, there was a surprisingly high prevalence of orthopedic complaints reported by 86 (64.2%) respondents. This rate is higher than that reported by interventional cardiologists and radiologists. Among interventional cardiologists, spine problems were reported in 42% of the 424 respondents; 70% were lumbosacral and 30% were cervical. Furthermore, more than one-third of them indicated that their spine problems had caused them to miss work. 2 Among interventional radiologists, back problems were reported by 52% of 236 respondents. 8 One of the hypotheses for the higher reported rates of orthopedic complaints among endourologists compared with interventional cardiologists or radiologists could be related to the fact that endourologists frequently have to change their body position to accommodate the course of the urinary system. This is especially exaggerated with the lack of video cameras and the use of rigid instrumentation (rigid ureteroscopes and nephroscopes).
In the present study, the prevalence of orthopedic complaints were significantly higher among African endourologists, older endourologists (>40 years), and longer duration of practice (>10 years). Furthermore, orthopedic complaints correlated with the combined annual caseloads of URS and PCNL. Similarly, spine problems among interventional cardiologists correlated with annual caseloads. 2 Furthermore, interventional cardiologists who wore aprons for longer periods had a substantially greater frequency of skeletal complaints, and more missed days from work because of pain compared with the control groups. 9
This study is the first of its kind examining the compliance of endourologists with radiation safety measures and their orthopedic complications. Radiation exposure and orthopedic injuries caused by heavy protective gear are important occupational hazards that endourologists face every day. Although there was good compliance with chest and pelvic shields, compliance with other radiation protective measures needs to be improved by education and open forum on the long-term consequences of radiation exposure. This is important since one-third of the noncomplaint respondents denied the harmful effects of radiation. Furthermore, the development of affordable lightweight and ergonomic radiation protective gear is desperately needed to further reduce noncompliance because of cost and discomfort.
There are several limitations to the present study. The Internet-based survey was sent to the e-mail accounts of all members of the Endourological Society. Therefore, members with incorrect or out-dated e-mail accounts did not receive the survey. Furthermore, the survey was available for 6 weeks. Thus, it is possible that some members were not available during this time to fill out the survey. Another bias is that those members with specific interest in radiation safety or members with orthopedic complaints may have been more inclined to fill out the survey than members who were less concerned about radiation safety. Ideally, dosimeters could have been used to measure annual radiation exposures among urologists and correlate them with orthopedic complaints. However, this was beyond the scope of the present survey.
Conclusion
There is good compliance among endourologists in the use of chest and pelvic shields. However, compliance in the use of thyroid shields, dosimeters, lead-impregnated glasses and gloves could be improved. Orthopedic complaints among practicing endourologists are common and correlate with the annual caseload of combined URS and PCNL.
Footnotes
Acknowledgments
This work was supported in part by the Northeastern AUA Young Investigator Award and Montreal General Hospital Foundation Award to Sero Andonian.
Disclosure Statement
No competing financial interests exist.