
Abstract
Purpose:
To evaluate a materials model for laparoscopic ultrasound identification and partial nephrectomy of kidney tumors.
Methods:
Five urology fellows performed laparoscopic ultrasonography (LUS) examination of the tumor model, and the time for identification was recorded. After identifying the tumor, they performed a laparoscopic partial nephrectomy using the target tumor with measurement of operative parameters. They completed a questionnaire and rated the quality of the renal tumor model on a 5-point Likert scale.
Results:
The participants were able to identify 49 tumors by LUS (98%). The mean time to identify the renal tumors by LUS was 1.12 minutes±0.93 standard deviation (SD). A partial nephrectomy was successfully completed on 49 tumor models (98%). The mean resection time was 7.69 minutes±3.8 SD. All of the participants considered that this model was helpful in the practice of LPN. The fellows would recommend this model as a teaching tool for residents/fellows to perform tumor imaging by LUS and for practicing LPN in a simulated environment.
Conclusion:
We have developed a unique model that simulates small kidney tumors that can be used for training surgeons in the clinical skills of laparoscopic partial nephrectomy.
Introduction
Appropriate training is mandatory for urologists considering performance of LPN. 8,9,10 Laparoscopic trainers and simulators play an important role in the acquisition of laparoscopic skills. 10 –12 The creation of solid organ artificial tumors or “tumor mimics” has been described as a viable training model for imaging and surgical techniques. 13 –17 There are reports of models that are injected into a porcine kidney, 18 developing effective surgical education tools. 13 Polyvinyl alcohol cryogel (PVA-C) is a material with tissue-mimicking properties that can be modeled into anatomic structures and can be tailored for very realistic imaging with ultrasonography (US), CT and MRI. 19 –21 We describe the assessment of a PVA-C model for renal tumors used for LPN training of fellows in urology.
Materials and Methods
PVA model preparation
PVA model preparation has been described previously by our group for renal tumor modeling. 19 –21 Commercial PVA powder (Airvol Grade 165, Air Products and Chemicals, Inc, Allentown, PA) is used to prepare the PVA liquid.
To make a 10% PVA solution, 900 mL of distilled water and 100 g of PVA powder are mixed in a 1 L tempered glass kettle and heated for 30 minutes to up to 75°C with a heating mantle on 80% power. Temperature is measured constantly with a digital thermometer and stirred with a mechanical mixer at 300 to 350 revolutions per minute (Fig. 1). The heater is then turned down to 5% to 15%, keeping the temperature no higher than 87°C for 1 hour. The resulting clear liquid is then poured into a plastic container, cooled to room temperature, and rested for 24 hours to allow air bubbles to rise to the surface. The PVA liquid is poured into an aluminum mold custom designed by the authors with five 1.5 cm spherical spaces (Fig. 2) and is cooled in a commercial chest freezer to −25°C for 12 hours. At the end of the 12 hours, the freezer is turned off and its lid kept open 3 cm with a wedge; a small commercial fan circulates the air out of the freezer, allowing a gradual return to room temperature over 12 hours.

Glass kettle, digital thermometer, heating mantle and mechanical mixer in polyvinyl alcohol preparation setting. Reprinted with permission from Fernandez et al. J Endourol 2011;25:1371–1375.
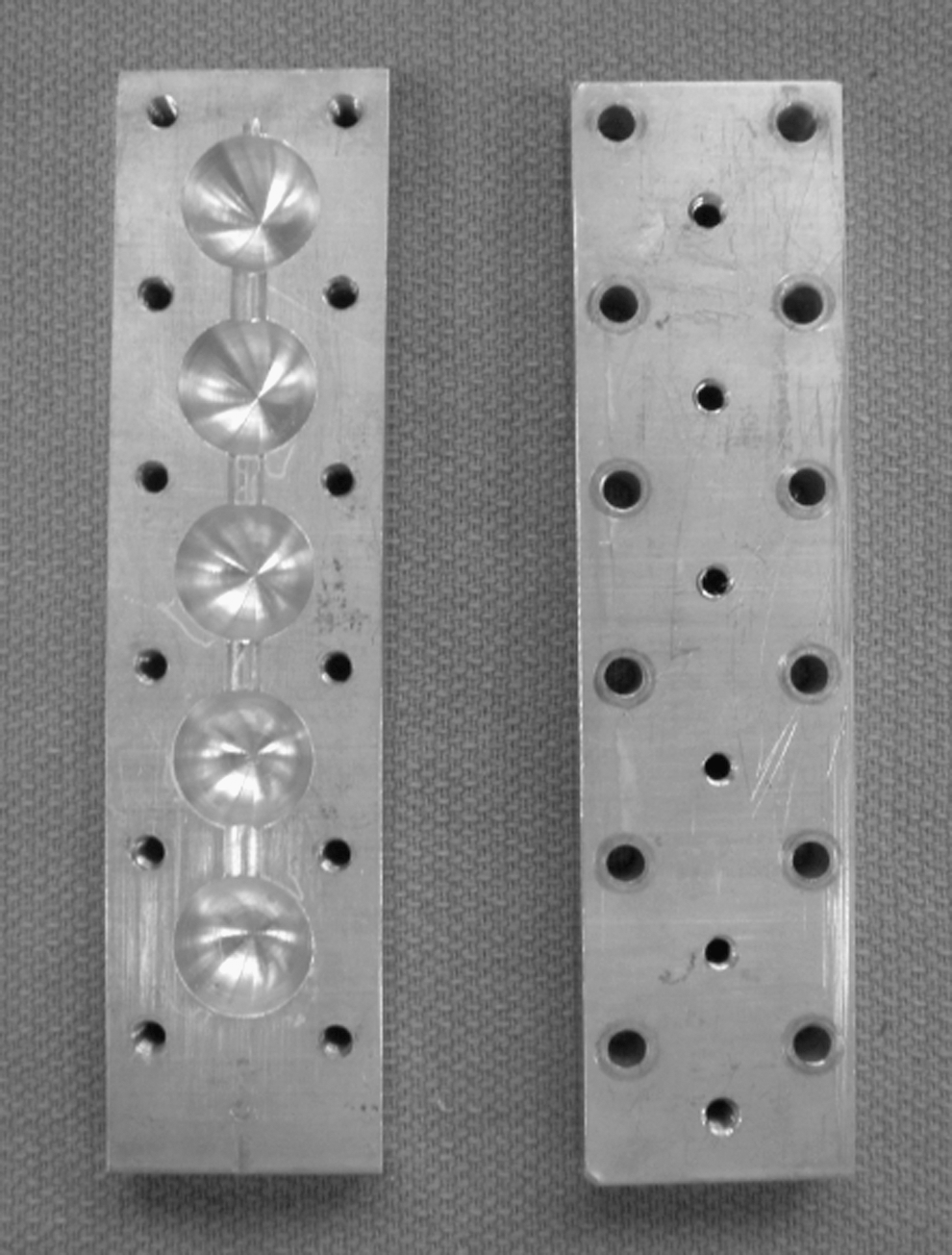
Aluminum tumor mold.
Two tumor models are threaded with a regular cotton suture and straight needle that is used to suspend the tumor model inside a custom designed kidney mold (Fig. 3). The kidney mold with the tumor models is sealed and filled with liquid PVA using a 60 mL syringe, and the freeze-thaw cycle described above is repeated. This process results in double freeze-thaw cycles for the tumors and a single freeze-thaw cycle for the kidney model. The final model is removed from the mold and stored in a container with clean tap or distilled water at room temperature (Fig. 4). The model's echogenic characteristics are shown in Figure 5.
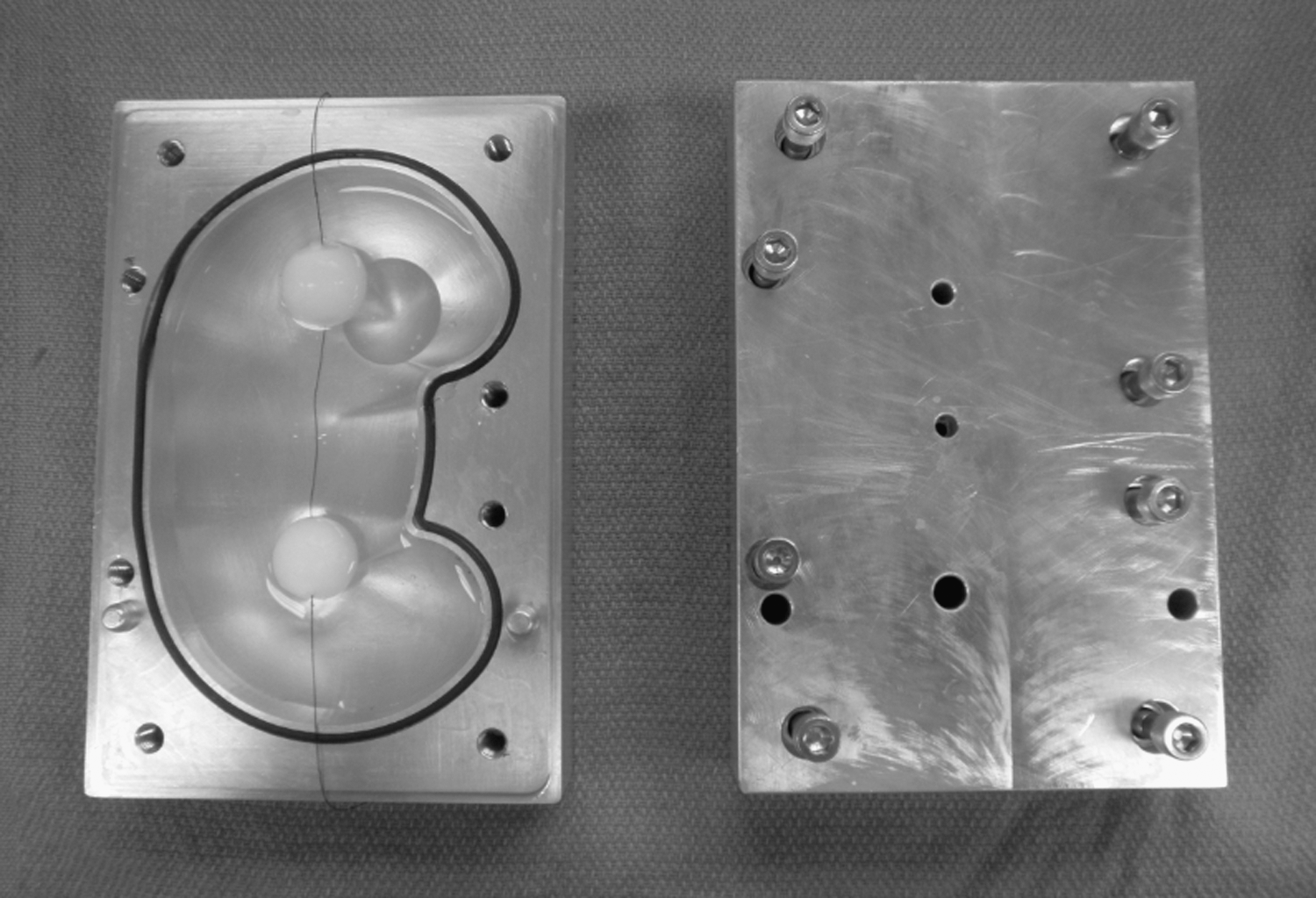
Aluminum kidney mold; note the suspended threaded tumor models. Reprinted with permission from Fernandez et al. J Endourol 2011;25:1371–1375.
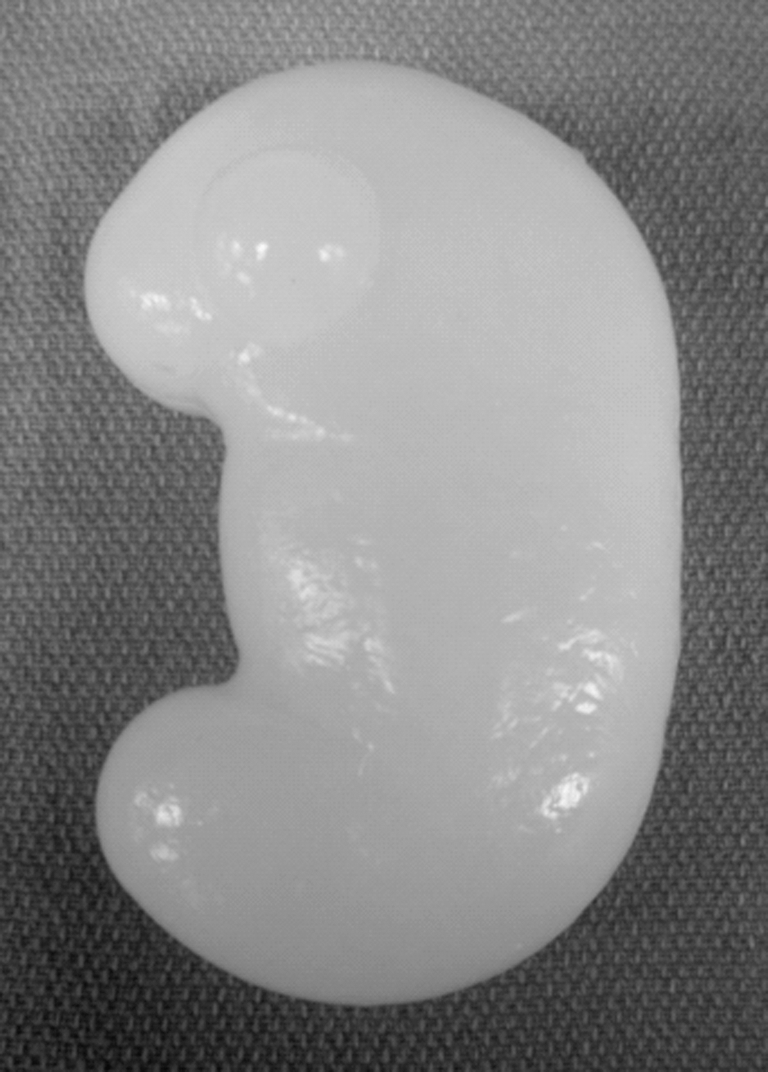
Final polyvinyl alcohol kidney model. Reprinted with permission from Fernandez et al. J Endourol 2011;25:1371–1375.
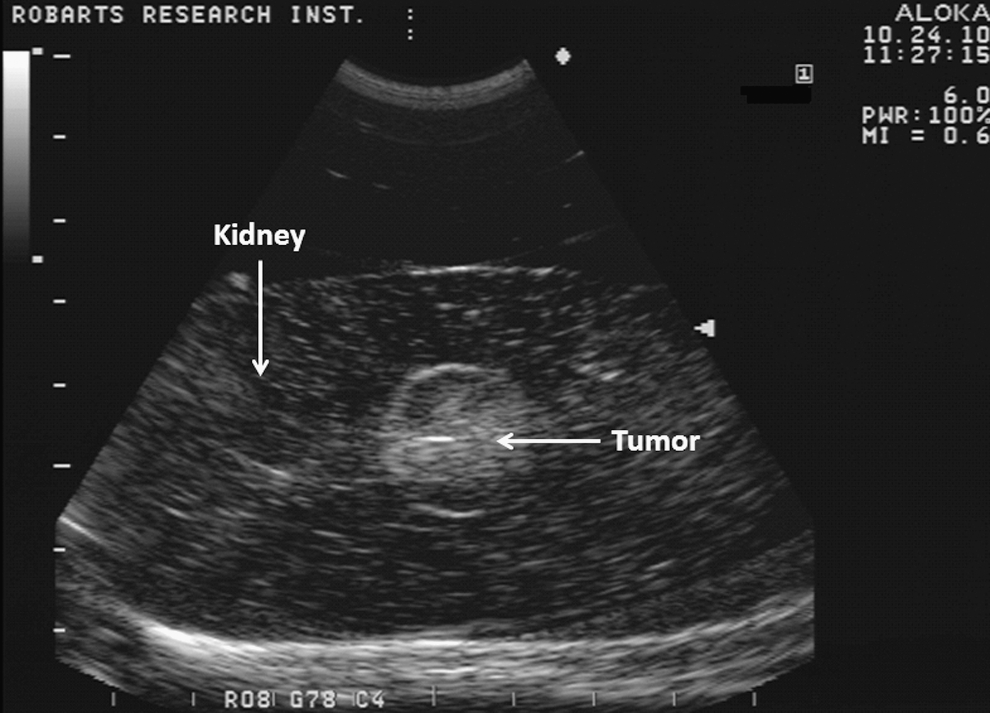
Final kidney and tumor echogenic appearance using the laparoscopic ultrasound probe.
Evaluation of the PVA model
After ethical approval from The University of Western Ontario (REB 17322E), five urology fellows performed standard two-dimensional laparoscopic ultrasonography (LUS) assessment with a 7.5 MHz probe of the kidney/tumor model placed in a laparoscopic simulator. The participants have varying levels of experience with LPN in the clinical setting. Each model had two tumors with a different location within the kidney model. The time to identify the tumor, the ability of the participant to do so, and the tumor location were recorded. The participants performed a LPN resection using standard laparoscopic instruments. The subject's ability to complete the LPN and the resection time were recorded. After completion of the resection, the margin status (positive or negative) was assessed. After the resection, the participants completed a questionnaire regarding the ease of visualization of the tumor within the model on LUS and the ease and realism with which they were able to perform the simulated LPN. They were also asked to rate the quality of the renal tumor model on a 5-point Likert scale.
Results
The fellows each performed 10 renal tumor identifications by LUS and then 10 LPN resections, making a total of 50 procedures. There was one female and four male subjects with a mean age of 33.4 years±1.51 standard deviation (SD) (range 31–35 y). Four participants reported 20 or more laparoscopic procedures as an assistant while one reported 5 or fewer; two participants had performed 20 or more laparoscopic surgeries as the primary surgeon, one reported 5 or fewer, one between 10 and 20, and one between 5 and 10. Twenty-two (44%) tumors were located in the upper pole, 5 (10%) in the midpolar area, and 23 (46%) in the lower pole, all endophytic.
The participants identified 49 tumors by LUS (98%), with one fellow not able to do so on one occasion (2%). This fellow had the least clinical experience. Mean time to identify the renal tumors by LUS was 1.12 minutes±0.93 SD (range 30 s–5 min). The partial nephrectomy resection was successfully completed on 49 models (98%), with one fellow who performed a resection unintentionally containing the two tumors on the kidney model on one occasion (2%).
Mean resection time was 7.69 minutes±3.8 SD (range 2–23 min) with positive margins in 13 (26%) cases and negative margins in 36 (72%) cases. The remaining case was not evaluated for margins because it was not properly identified and resected (2%). The surgical margin was considered positive when the resected specimen was devoid of normal surrounding renal parenchyma or if the base of the resection demonstrated residual tumor. Positive margins increased steadily in the first three resections and then we observed a steep decline in the last seven cases. In the ninth and tenth cases, all participants had negative margins (Fig. 6).
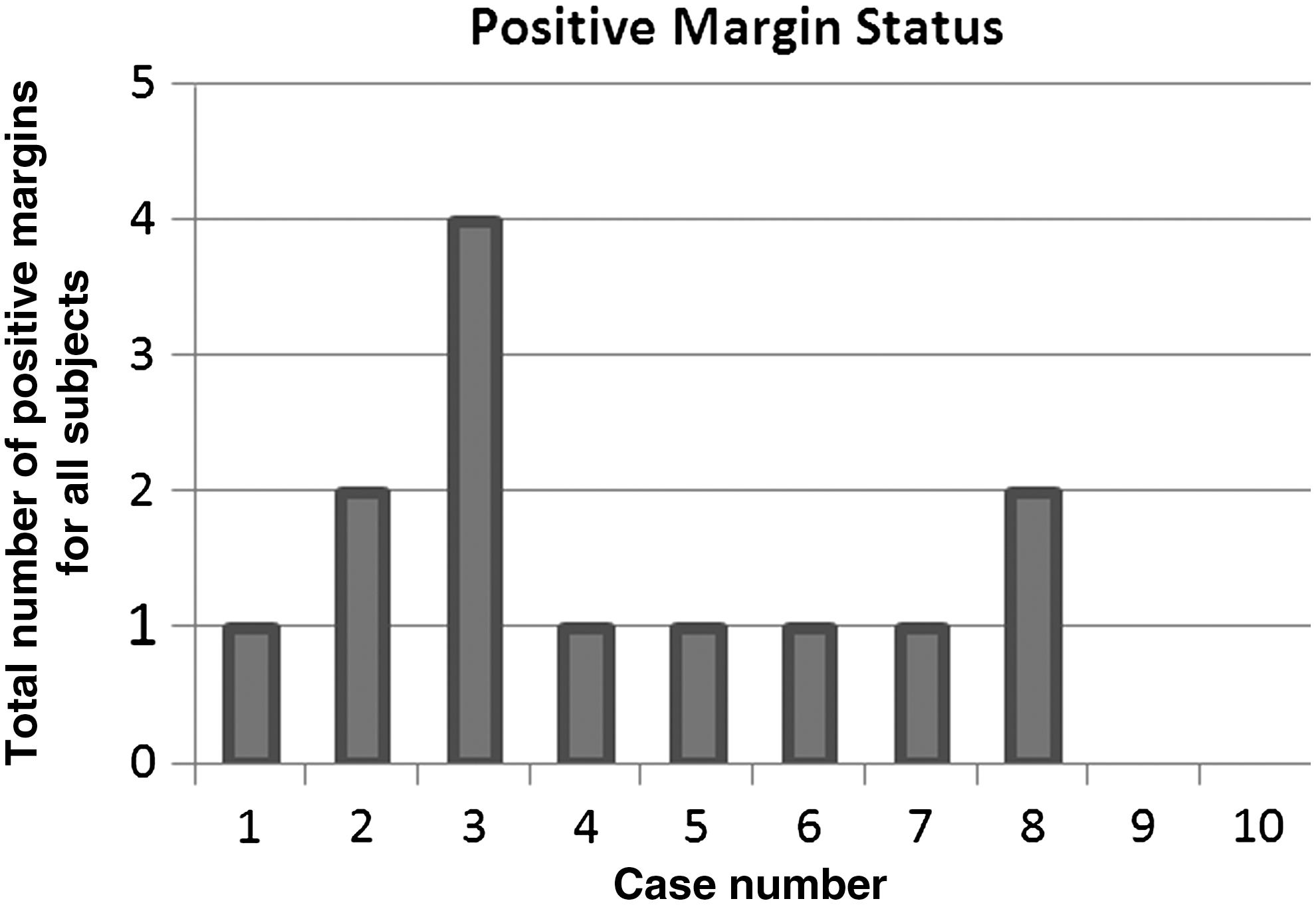
Positive margins by case. There were no positive margins in the last two cases.
The first LPN performed by the participants took longer, with 12.2 minutes±7.15 SD experiencing a stable decline until the eighth LPN, which took the shortest time with 5 minutes±1.22 SD, and then increasing back slightly to 9 minutes±5.5 SD and 7 minutes±1.22 SD on the ninth and tenth cases, respectively (Fig. 7). Four fellows declared that it was “easy” to identify the tumor within the kidney models with LUS (4 of 5 in the Likert scale), while one declared that it was “very easy” (5 of 5). Four participants considered that the tumor and kidney tissue had “good realism” on LUS (4 of 5), and one thought it was “very realistic” (5 of 5). Regarding the textural consistency of the models, one study participant thought that it was “moderately realistic” (3 of 5), three thought it had “good realism” (4 of 5), and one considered it to be “very realistic” (5 of 5).

Resection time by case.
One participant found it “difficult” to perform the LPN (2 of 5) on the model, and another one thought it was “moderately easy” (3 of 5), while three considered the LPN on the tumor model was “easy” to perform (4 of 5). All of the participants considered that this model was helpful in learning to perform or practice LPN and would recommend this model as a teaching tool to perform tumor imaging by LUS and for practicing LPN in a simulated environment. Four subjects would recommend this model as a teaching tool for residents and fellows to learn the technical skills of the LPN, while one would not.
Discussion
Laparoscopic simulators are an important tool in the acquisition of surgical and laparoscopic skills. 10,11 Tissue mimicking phantoms have been shown to be an important component in medical imaging research. 20 PVA-C is a useful phantom material with US, CT, and MRI characteristics that closely resemble real tissue. 19,22 PVA-C is a recyclable material, so that once a model has been used, it can be melted and remodeled. With the addition of enhancing imaging agents such as gadolinium and barium, this model can also provide effective imaging by CT and MRI.
In this work, we investigated the feasibility of creating a phantom material to reproduce the ultrasonographic characteristics of renal tumors and to create a teaching model for LPN. Renorrhaphy on the models can be accomplished as long as a monofilament suture is used, because braided sutures tear the PVA-C material easily.
In this study, we report a 26% rate of positive margins, but there is a tendency toward a decrease in the number of positive margins over time, until no positive margins were found in the last two cases. Published positive margin rates 23 are widely discordant to our findings, so we hypothesize that training with this model before performing this procedure in the clinical setting potentially reduces the learning curve. Resection time declined over time, and the slight increase in the last two cases can be explained by participants' fatigue.
The limitations to this study are the use of a small, fixed-camera laparoscopic simulator that did not allow a complete view of the kidney model. Second, the glare produced on the surface of the model can be solved simply by changing the model's color. Last, this study involved five participants with varying levels of laparoscopic experience. Future testing with a broader cohort is needed to test the content validity.
Our preliminary results demonstrated that it is possible to re-create the environment encountered during LUS imaging of a renal tumor.
Conclusion
The assessment of a PVA-C renal tumor model for teaching renal tumor identification by LUS and LPN has demonstrated it to be realistic and useful for training purposes. Although PVA-C preparation and model manufacturing are labor intensive, its use is less expensive and with less logistic concerns than those associated with an animal model.
Footnotes
Disclosure Statement
No competing financial interests exist.