
Abstract
Purpose:
To evaluate the feasibility of a novel transvesical port (TVEP) for natural orifice translumenal endoscopic surgery (NOTES) in the porcine model.
Materials and Methods:
The TVEP consisted of an internal guide core and external sheath design using computer-aided design software. Transvesical peritoneoscopy, renal biopsy, as well as combined transvesical/transgastric nephrectomy were performed through the TVEP in a porcine model. Operative parameters and port performance were measured.
Results:
Twelve procedures were successfully performed by four surgeons. No complications occurred with introduction of the TVEP. The mean time for placement was 5.6 minutes. Steady pressure controlled CO2 pneumoperitoneum up to 15 mm Hg with a flow of 2 L/min was achievable. The average scoring by physician of the TVEP was 4.75 for ease of placement, 5 for ability to maintain pneumoperitoneum, 4.25 for convenience of inserting instruments, and 4.5 for overall satisfaction. The average score regarding instruments exchangeability, however, was relatively low: 3.25.
Conclusions:
Real surgery using a novel TVEP is feasible in performing transvesical NOTES.
Introduction
The development of an effective closure device demonstrated in a porcine model might enable the widespread adoption of the transvesical approach in NOTES. 6 To our knowledge, only a specialized transvesical over tube was reported to be designed and successfully applied 4 ; nevertheless, transvesical NOTES is still an investigational approach in urology because of the immaturity of an appropriate transvesical port. The aim of this study was to evaluate the feasibility and effectiveness in vivo of our novel transvesical port (TVEP) for NOTES.
Materials and Methods
Design
The TVEP device was designed using computer-aided design software and manufactured by Weigao Medical Instruments Co., Ltd (Shandong, China). TVEP consists of an internal guide core and external sheath, which can accommodate a 8/9.8F ureteroscope or 5-mm conventional laparoscopic instruments (Figs. 1, 2). The external sheath has a length of 20 cm, internal diameter of 20F, and external diameter of 22F. The sheath can be sealed with a silica gel cap. The external sheath has an insufflating inlet with the diameter of 9F, which can also be covered with a plastic sealing cap or connected to a pneumoperitoneum insufflator (Fig. 3). The 22-cm internal guide core has a wire guide in the center (Fig. 4).

The transvesical port consists of
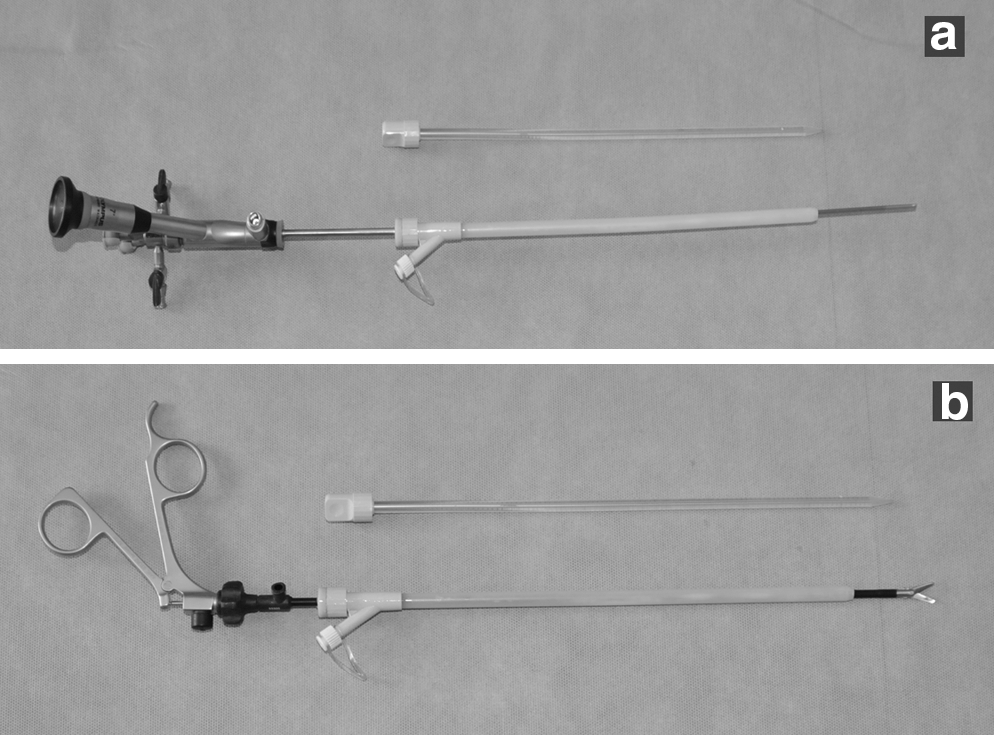
The external sheath can accommodate
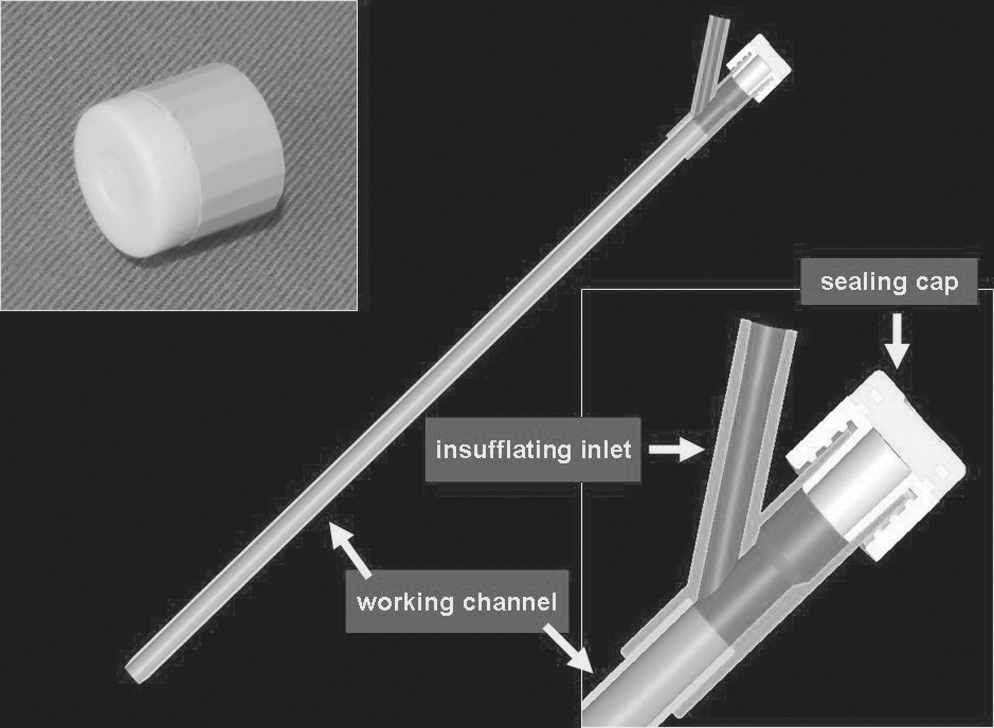
Engineering drawing of the external sheath of the transvesical port.
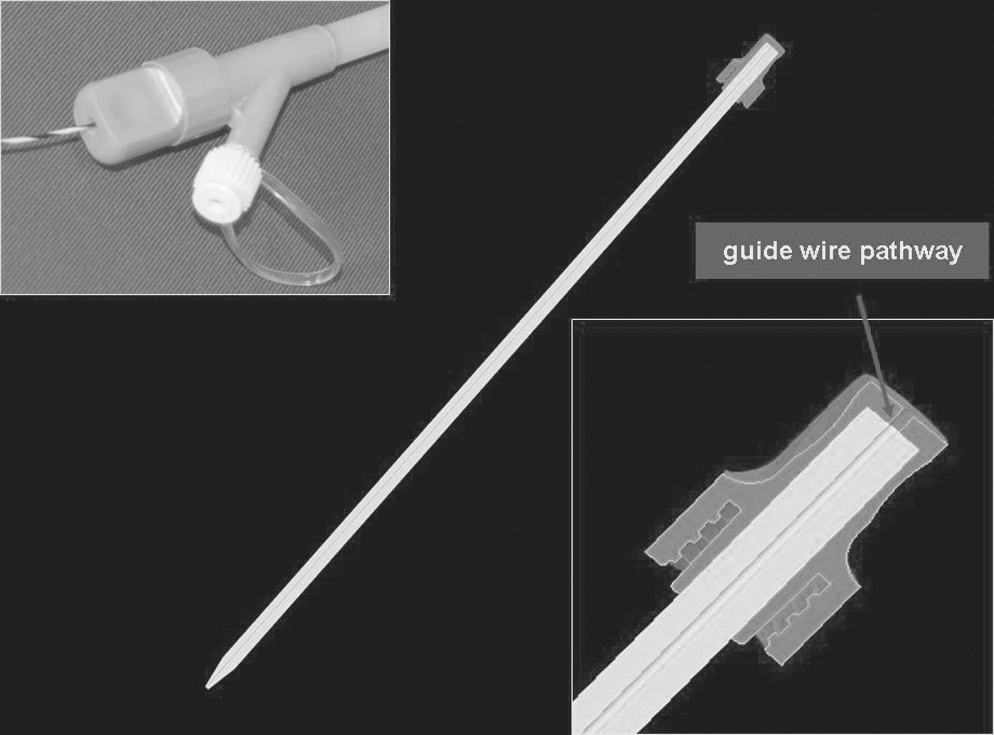
Engineering drawing of the internal guide core of the transvesical port.
Animate model
The ethical review boards of Changhai Hospital, Shanghai, China, approved this nonsurvival study. All procedures were performed in four 1 to 2 years old, 30 to 40 kg female pigs, which were provided by Miaodie Biotechnology Co., Ltd (Shanghai, China). The animals were withdrawn from food for 24 hours and from water for 6 hours before the procedure. All procedures were performed under general anesthesia at Asian and Pacific training center of Covidien Ltd (Shanghai, China) in 2010.
Surgical technique
Surgical instruments
Basic endoscopic instruments included a 8/9.8F rigid ureteroscope (Olympus, Tokyo, Japan), a double-channel GIF-2T160 gastroscope (Olympus), a A2576 scissors for ureteroscope (Olympus), a KD-11Q-1 high-frequency needle-shape electrome for gastroscope (Olympus), and a 5837 dilator (Cook, USA). Basic laparoscopic instruments included a 5-mm harmless grasper, a 5-mm Maryland dissecting forcep, a 5-mm common scissors (Karl Storz, Tuttlingen, Germany), and a 5-mm Endoclip, a 5-mm ultrasonic scissors, a 5-mm flexible scissors (Covidien, Princeton, NJ).
Transvesical access, peritoneoscopy, and biopsy
Four experienced laparoscopic surgeons, having previously performed at least 50 laparoscopic nephrectomies, undertook the transvesical procedure on four pigs. The transvesical approach was established with animals in the supine position after general anesthesia (Figs. 5 a–c), as described previously. 4 A 8/9.8F rigid ureteroscope was introduced through the urethra into the bladder along the guidewire, and then the bladder was emptied of urine and refilled with saline. A 0.8 to 1.0-cm mucosal incision was performed on the ventral bladder wall caudal to the bladder dome, with A2576 scissors introduced by the working channel of the ureteroscope. The ureteroscope was withdrawn after a 0.035-inch flexible tip guidewire was introduced into the peritoneal cavity through the incision site. Then the integrated TVEP was introduced into the peritoneal cavity over the guidewire.
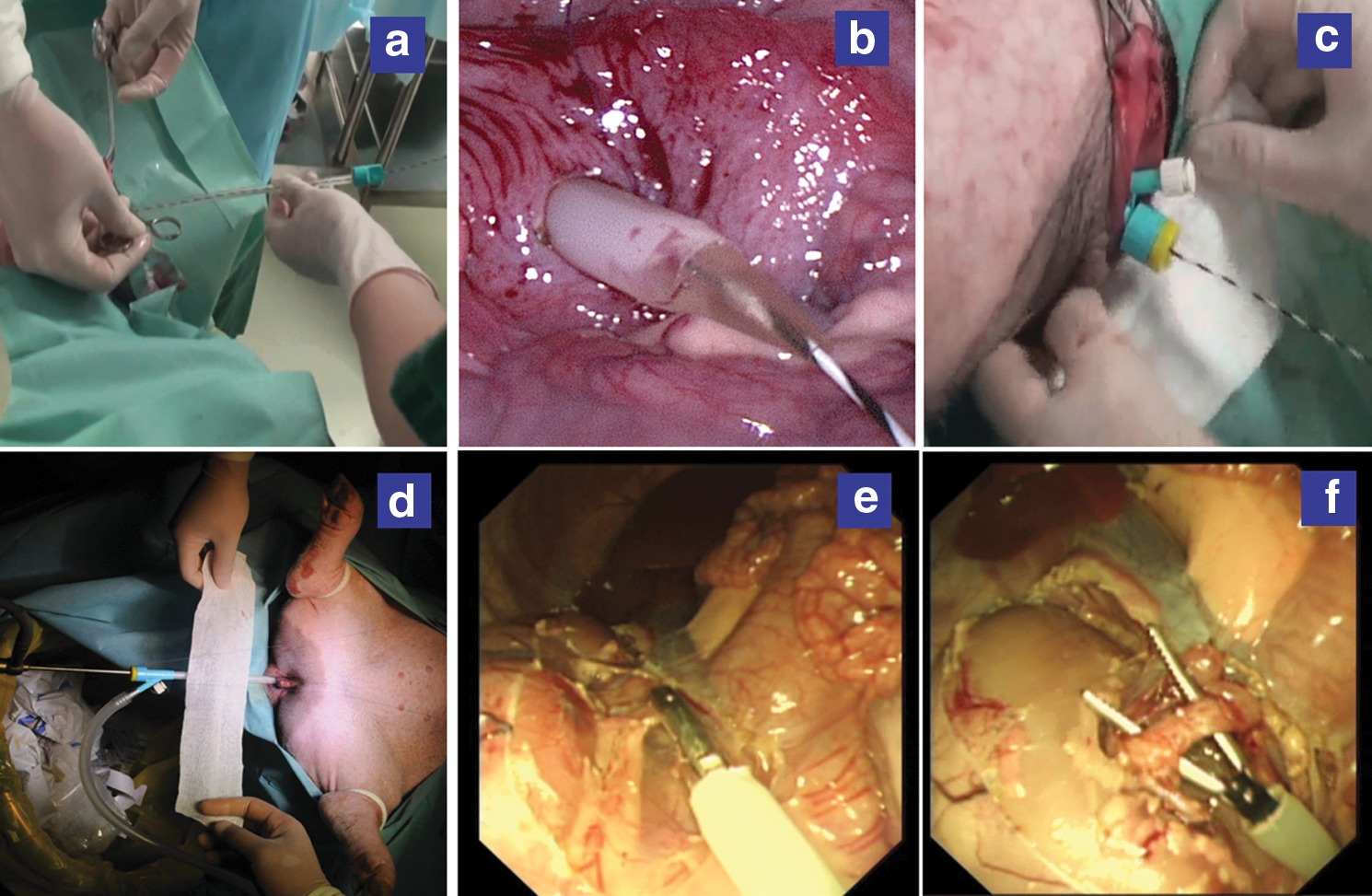
After withdrawing the internal guide core, the TVEP and its insufflating inlet were connected with a silica gel sealing cap and an Olympus® UHI-3 insufflator, respectively. The guidewire was withdrawn after a stable CO2 pneumoperitoneum up to 15 mm Hg was achieved. The ureteroscope was introduced (Fig. 5d). Through the TVEP, transvesical peritoneoscopy was performed to identify organs of the upper abdomen, including the liver, spleen, and kidneys. A transvesical kidney biopsy was performed on all pigs in the lateral decubitus position: Incision of the Gerota fascia was made with A2576 scissors introduced by the working channel of the ureteroscope, and kidney biopsy the size of 0.5×0.5 cm was taken.
Transgastric access
As described previously, 7 a GIF-2T160 gastroscope was introduced into the peritoneal cavity through a gastrotomy established on the anterior stomach wall. All procedures were monitored by the ureteroscope positioned through the TVEP.
Transvesical and transgastric procedure
Unilateral nephrectomy was performed in four pigs in the lateral decubitus position with combined transvesical and transgastric access. Opening the parietal peritoneum, dissecting and clipping renal vessels, dividing renal vessels, and complete isolation of the kidney were performed with a 5-mm ultrasonic scissors passed through the TVEP, which was the only working channel (Figs. 5e–f). During these steps, the gastroscope was the viewing channel. The kidney was not extracted. After placing the animal in a contralateral decubitus position, nephrectomy was again performed. On completion of the procedure, all animals were sacrificed.
Operative and postoperative evaluation
Operative time of TVEP introduction and CO2 pneumoperitoneum pressure and flow in the procedure were recorded. Immediately after surgery, the feasibility and effectiveness was evaluated by the surgeon using a modified rating scale. 8 Five categories were assessed: Ease of placement, ability to maintain pneumoperitoneum, convenience of inserting instruments, instruments exchangeability, and overall satisfaction. Each category was rated on a 1 (worst) to 5 (best) scale.
Results
Twelve procedures were successfully performed by four surgeons, including four transvesical kidney biopsies, and eight combined transvesical and transgastric nephrectomies. No complications occurred with the introduction of TVEP during gastric incision or gastroscope placement into the peritoneal cavity under the guidance of the ureteroscope. Average operative time of TVEP introduction was 5.6 minutes. During the procedure, TVEP happened to be withdrawn into the bladder only once and was then readily reintroduced into the peritoneal cavity under the guidance of the ureteroscope. Pressure controlled CO2 pneumoperitoneum up to 15 mm Hg with a flow of 2 L/min was achieved in all procedures.
As shown in Figure 6, the average scores of TVEP were 4.75 (ease of placement ), 5 (ability to maintain pneumoperitoneum), 4.25 (convenience of inserting instruments), and 4.5 (overall satisfaction), respectively. Instruments exchangeability, however, was a relatively lower average score of 3.25. After the evaluation, two improvements were proposed by the present group, including the design of a balloon TVEP and an additional channel for urine drainage.
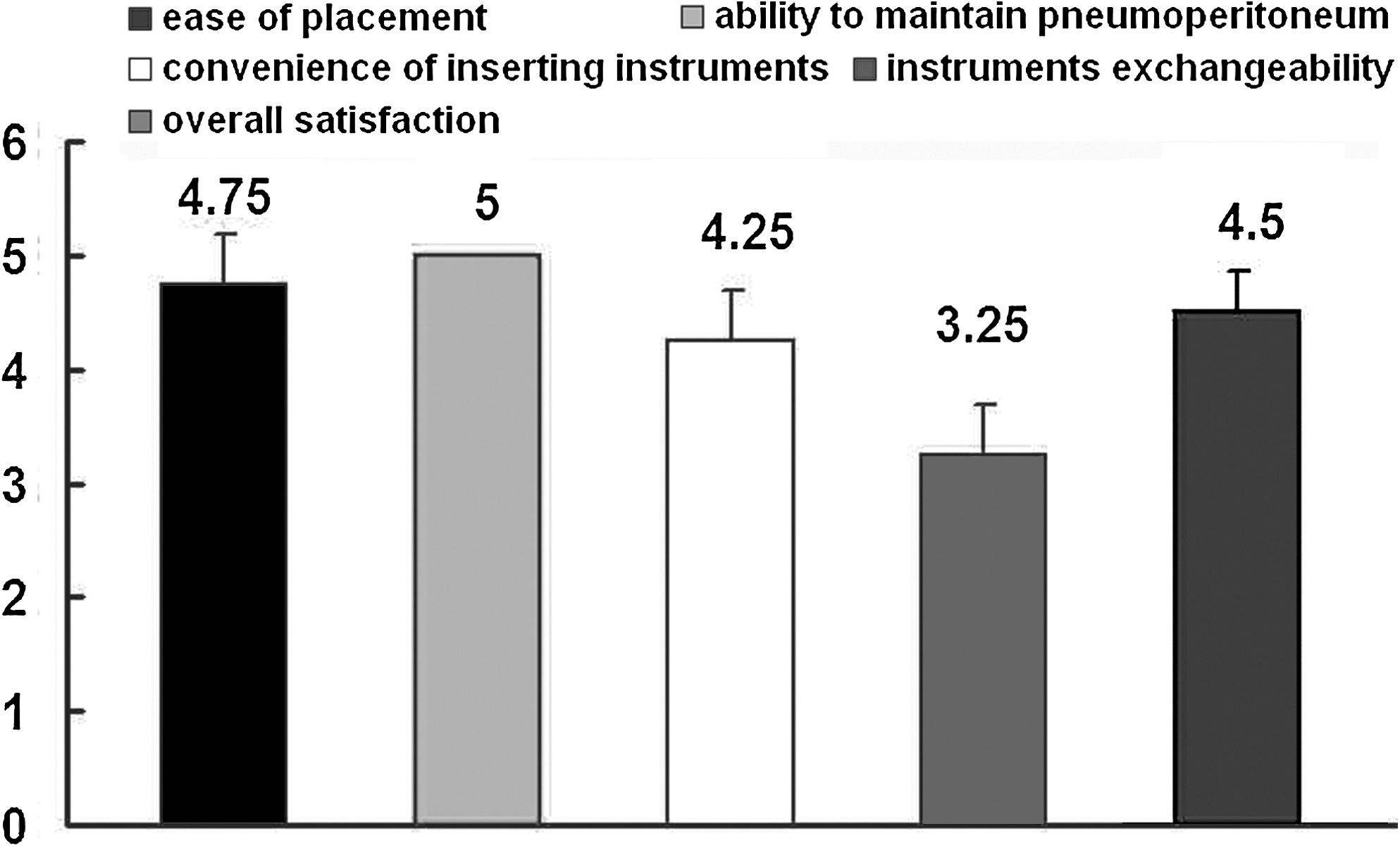
Scores of the transvesical port evaluated by the surgeons, with a modified rating scale including five categories.
Discussion
Minimally invasive techniques are the preferred method for managing most urologic conditions. 9 The latest scarless surgery, NOTES, has evolved greatly with the first clinical “pure” NOTES ectomy in urology reported in 2010. 10 Lima and associates 4 verified that the transvesical approach was a simpler and easier way to overcome most of the limitations of the isolated transgastric port for NOTES. In fact, transvesical access is naturally sterile and anatomically is the most anterior lower abdominal port providing instrument access to the peritoneal cavity above the bowel loops and is available in both genders. 9 This approach to access the peritoneal cavity was demonstrated to be safe and feasible. 9 Subsequently, the other applications of the approach were extended to animal models by several groups 7,11,12 : Reaching the thoracic cavity, and combined transvesical and transgastric cholecystectomy and nephrectomy.
In 2007, Gettman and colleagues 13 performed the first clinical transvesical NOTES—a peritoneoscopy. Given the anatomic and physiologicaproperties, the transvesical NOTES represents an exciting new concept in the ever-expanding field of minimally invasive surgery. 14
To our knowledge, three methods for establishing access for transvesical NOTES have been reported: Blunt tip prototype, 14 our previously described ureterorenoscope sheath, 15 and over tube. 4 We have experience using each of these devices. Access obtained using the blunt type prototype necessitated increased force, limiting its application to simple transvesical peritonoscopy or biopsy. 14 In addition to high cost, the ureterorenoscope has the disadvantage of poor maintenance of pneumoperitoneum and a limited aperture that cannot accommodate some 5-mm laparoscopic instruments (Fig. 7). The over tube can maintain adequate pneumoperitoneum; however, because there is no sealing cap at the end of the tube, the risk of losing insufflation is great when there is a space between the instrument and the tube or during exchange of instruments. The over tube also requires introduction via an expensive ureterorenoscope sheath. 4 Given these shortcomings, the development of an improved transvesical port is vital to advancing transvesical NOTES.

Ureterorenoscope sheath was used as a transvesical port for natural orifice translumenal endoscopic surgery.
An ideal novel port should meet the demands, including easy introduction, maintenance of pneumoperitoneum, instruments exchangeability, and so on. We designed the novel specialized TVEP fully considering the principle of establishment of percutaneous nephroscopic access, the structural feature of laparoscopic trocar, and the disadvantages of the over tube. Its 20-cm long external sheath is longer than the percutaneous nephroscopic sheath, and it is necessary for clinical transvesical NOTES research. According to the structural feature of multilumen laparoendoscopic single site TriPort™ platform (Olympus), a detachable silica gel sealing cap was added at the terminal of the external sheath, which would prevent gas leakage even in the process of instruments replacement.
Compared with the over tube, 4 the advantages of the TVEP are epitomized by the following, as shown in Figures 1 to 4. First, the external sheath has an insufflating inlet with the diameter of 9F, which can be covered with a plastic sealing cap, or be connected to pneumoperitoneum insufflators. Stable pneumoperitoneum pressure can be created more precisely, and the ureteroscope can perform more conveniently without connection with insufflators. Second, the terminal of the external sheath is covered by a silica gel sealing cap, which can eliminate gas leakage when the instrument is introduced and performed, or even is replaced. Third, TVEP consists of a specialized internal guide core, which can guide the integrity of TVEP to be introduced along the guidewire. Compared with the dilator of an expensive ureterorenoscope sheath enveloped by the over tube, the internal guide core of TVEP is cost-effective.
The feasibility of the TVEP was then tested in pigs in the present study, and evaluation of the TVEP was completed by four surgeons. The average scores of ease of placement, ability to maintain pneumoperitoneum, convenience of inserting instruments, and overall satisfaction were all higher than 4, and, in particular, ability to maintain pneumoperitoneum got a score of 5. We also discovered that if the incision of the ventral bladder wall was not large enough, it would be difficult to be enlarged only with the dilator of the internal guide core, because of good resilience of bladder tissue. In our experience, a 0.8 to 1.0-cm incision in the bladder wall was better and sufficient for successful introduction of the TVEP and limited the time for establishing access. Furthermore, for the sealing cap made of silica gel, smearing lubricant was needed in the instrument replacement. Further improvement of the terminal cap of the TVEP is needed to optimize its application.
Instruments exchangeability of TVEP, however, was limited by the urethral diameter. Practically, as in our experience, transvesical nephrectomy could be successfully completed using 5-mm conventional laparoscopic instruments with TVEP being the only working channel. Although an endoscopic wire loop was available for specimen extraction in the transgastric NOTES partial nephrectomy in a porcine model, 16 large specimen extraction is still a pending problem for NOTES. In this respect, a tissue pulverizer is likely to drive a major paradigm shift in the extraction of large specimens such as kidneys, while a small-caliber Endocatch bag is worth considering for extraction of smaller ones. The study also led us to believe that an additional urine drainage channel and the balloon TVEP would improve its feasibility and effectiveness.
There are some limitations to this study that should be considered. Although we collected as much objective data as possible to evaluate the TVEP, evaluation by the surgeons was subjective. 17
Conclusion
Our novel TVEP has initially proved to be feasible in transvesical NOTES. It may simplify the process of the transvesical approach and provide an inexpensive and reliable NOTES platform.
Footnotes
Disclosure Statement
No competing financial interests exist.