
Abstract
Purpose:
This study compared the characteristics and outcomes of percutaneous nephrolithotomy (PCNL) in patients with and without renal malformations using the Clinical Research Office of the Endourological Society (CROES) PCNL Global Study database.
Patients and Methods:
The CROES PCNL Global Study collected prospective data for consecutive patients who were treated with PCNL at centers around the world during 1 year. Patient characteristics, operative data, and outcomes of PCNL in patients with renal anomalies and those with normal kidneys were compared.
Results:
Of 5542 patients whose renal anatomy was recorded, 202 (3.6%) patients had a renal malformation. The most frequent anomalies were horseshoe kidneys (1.8%) and malrotated kidneys (1.3%). The prone position was the most frequently used position for patients with renal anomalies as was upper pole puncture. PCNL achieved stone-free rates of 76.6% in patients with anomalous kidneys and 76.2% in those with normal kidneys. The frequency of complications was similar in the two groups. Median operative time was significantly longer (87 min vs 75 min, P=0.037), and access for PCNL was unsuccessful in significantly more patients (5% vs 1.7%, P=0.001) in whom renal anomalies were present.
Conclusion:
In patients undergoing PCNL, the presence of renal malformation is likely to extend operative time. Stone-free rates as well as incidence of complications after PCNL are similar irrespective of the presence of renal anomalies.
Introduction
Ectopic kidneys occur in approximately 1 in 900 live births. 1 The abnormal position of such kidneys can be pelvic, iliac, abdominal, thoracic, or crossed, which may then become fused. Most ectopic kidneys are malrotated to some extent.
The abnormal anatomy, rotation, and vasculature of horseshoe and ectopic kidneys contribute to an increased risk of renal stone formation. The incidence of stone formation in patients with horseshoe kidneys, for example, is up to 60%. 2 Extracorporeal shockwave lithotripsy has been the treatment of choice for patients with calculi in horseshoe kidneys. 3,4 In recent years, a reduction in morbidity together with stone-free rates of >90% have established percutaneous nephrolithotomy (PCNL) as a primary management option for large and complex renal stones in normal kidneys. 5 Notably, recent retrospective case series report comparable stone-free rates for PCNL in anomalous kidneys. 6 –10
The purpose of the Clinical Research Office of the Endourological Society (CROES) PCNL Global Study was to establish a prospective global database for the current indications and outcomes of PCNL. The present study evaluated patient characteristics, operative characteristics, and outcomes of PCNL in patients with renal malformation using the CROES PCNL Global Study database.
Patients and Methods
The CROES PCNL Global Study was a prospective observational study during which data were collected for consecutive patients who were treated at each participating center over a 1-year period. The study organization and methods are described in detail elsewhere. 11 The patient was considered stone-free when all stones had been taken out and he/she was stone free by 30 days post-treatment.
Patients were assigned to groups depending on the presence or absence of renal malformations.
Study objectives
The objectives of this analysis were to compare the patient characteristics, surgical procedure data, and outcomes of PCNL in patients with and without renal malformation.
Analytical and statistical methods
Data were compared descriptively in the two patient groups. The level of significance for differences between groups was estimated using chi-square tests and Mann-Whitney U tests for categorical and continuous variables, respectively. Perioperative complications were assessed and graded according to the modified Clavien system 12 as applied to PCNL. 13 For patients with nonstaghorn calculi, renal stone load was calculated by aggregating the estimated volume of each stone using the formula: total stone load=∑ (length×width×Π×0.25). 14
Results
In the CROES PCNL Global Study, data were obtained for a total of 5803 patients at 96 study centers in Europe, Asia, North America, South America, and Australia. Renal malformation status was recorded for 5542 patients. Renal stones were present in 202 (3.6%) patients with anatomical kidney malformations, including horseshoe kidneys (n=102 [1.8%]), malrotation anomalies (n=74 [1.3%]), and ectopia (n=26 [0.5%]). In addition, 189 (3.3%) patients who were treated for renal stones had a functional monokidney and will be reported separately. Other renal anomalies such as caliceal diverticuli, ureteropelvic junction obstruction, and megacalycosis were not specifically captured in this database.
Patient characteristics
The overall characteristics of two patient groups were generally similar (Table 1). Patients with kidney malformation were, on average, slightly younger when they underwent PCNL, and there was a significantly higher proportion of males in this group. The median stone burden that was associated with a renal anomaly was significantly higher than that of normal kidneys (P=0.024), but a significantly lower proportion of anomalous kidneys were found to contain a staghorn calculus (P=0.021).
SD=standard deviation; BMI=body mass index; IQR=interquartile range; ASA=American Society of Anesthesiologists; SWL=extracorporeal shockwave lithotripsy; PCNL=percutaneous nephrolithotomy; URS=ureteroscopic stone removal.
Intraoperative characteristics
Comparing the number of patients undergoing PCNL in the supine or prone positions revealed that significantly more patients with renal anomalies underwent the procedure in the prone position (P=0.01; Table 2). The proportion of patients undergoing PCNL in the prone position was greater in those with horseshoe kidneys compared with no renal malformation or other type of renal malformation. Significant differences were observed between patients with abnormal and normal renal development with regard to puncture site (Table 3). A substantially greater proportion of PCNL procedures used an upper pole or middle caliceal puncture site in patients with renal malformation, whereas the lower pole site was used in the majority of patients with normal kidneys. The patterns of cutaneous access point (above 11th or 12th rib or below 12th rib) and guidance method used for PCNL were generally similar in the two groups. In terms of access, there was no clinically significant difference if the access was obtained by a urologist or by a radiologist.
Outcomes of PCNL
Outcomes of the procedure are shown in Table 4. Outcomes for the two groups were similar in terms of the frequency of common complications of PCNL, such as excessive bleeding, necessity for blood transfusion, and fever. Success rates in terms of stone-free rates of more than 76% were achieved in both patient groups. For surgery involving patients with renal malformation, the median duration of surgery was significantly longer (P=0.037), and a significantly higher proportion of procedures failed to obtain satisfactory percutaneous renal access (P=0.001) compared with the normal kidney group. Nevertheless, the stone-free rates were similar in the two groups. The mean length of hospital stay was 3 days.
IQ=interquartile range.
Comparison of different renal anomalies
Patients with a malrotated kidney were, on average, slightly older than patients with other renal malformations (Fig. 1). Mean stone burden was also highest in malrotated kidneys and lower in ectopic kidneys compared with other renal abnormalities (Fig. 2). Duration of surgery was longer for procedures involving horseshoe kidneys compared with those on normal kidneys, while operating times for malrotated kidneys were similar to normal (Fig. 3). Clavien scores in all four patient groups were similar (Fig. 4). The average period of hospitalization was longest for patients after PCNL of ectopic kidneys and shortest for those with malrotated kidneys (Fig. 5).
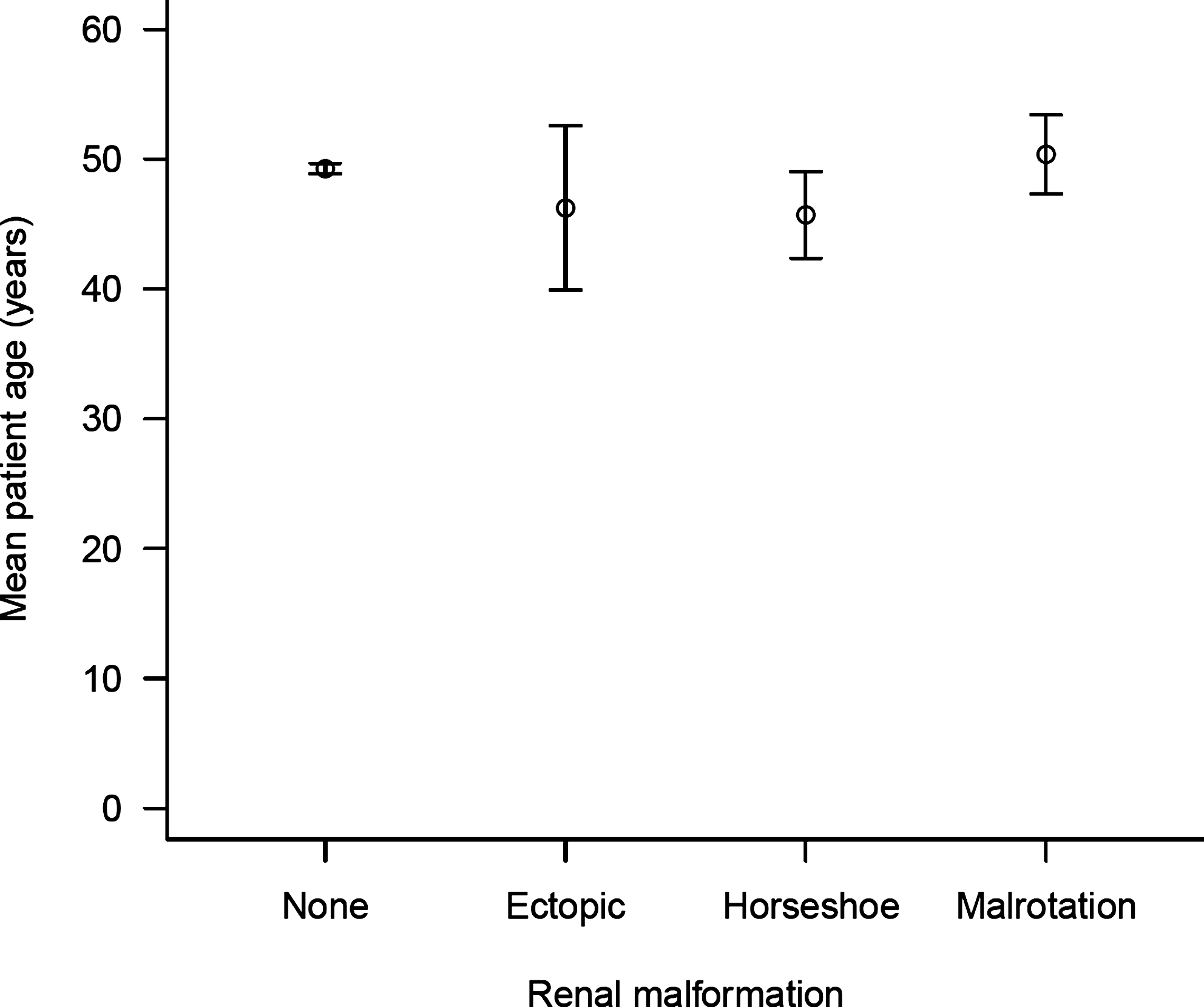
Age of patients according to renal malformation. Data are shown as mean±95% confidence interval.
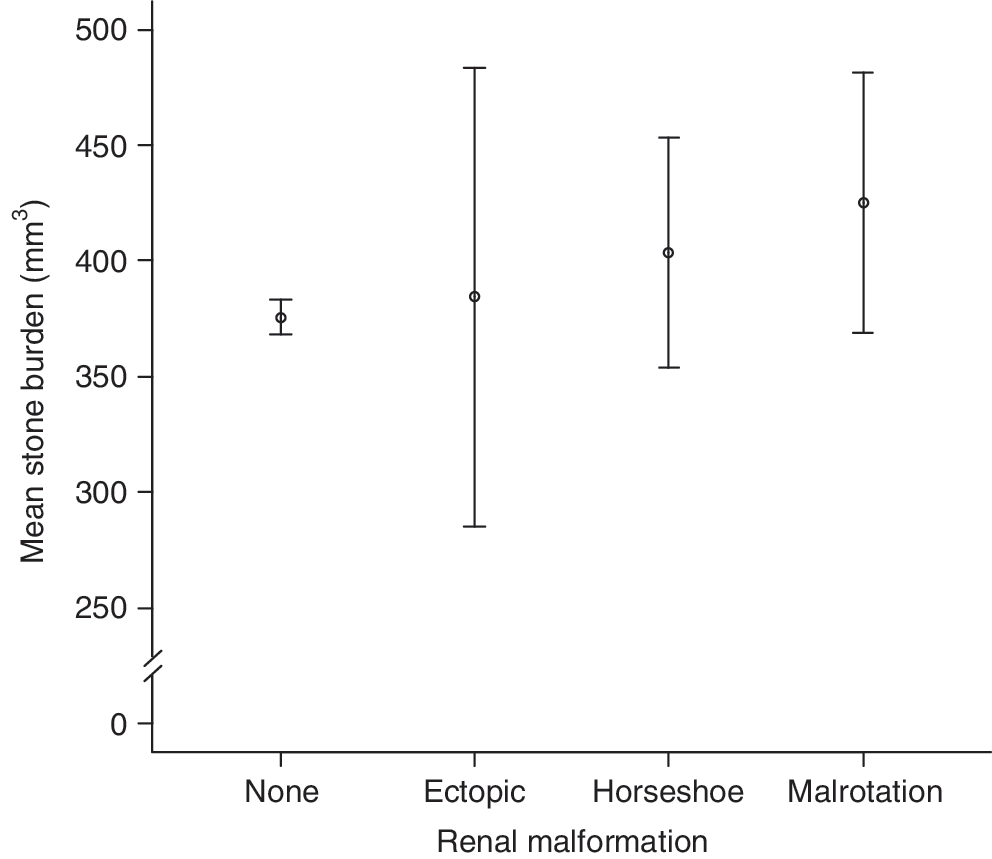
Stone burden according to renal malformation. Data are shown as mean±95% confidence interval.
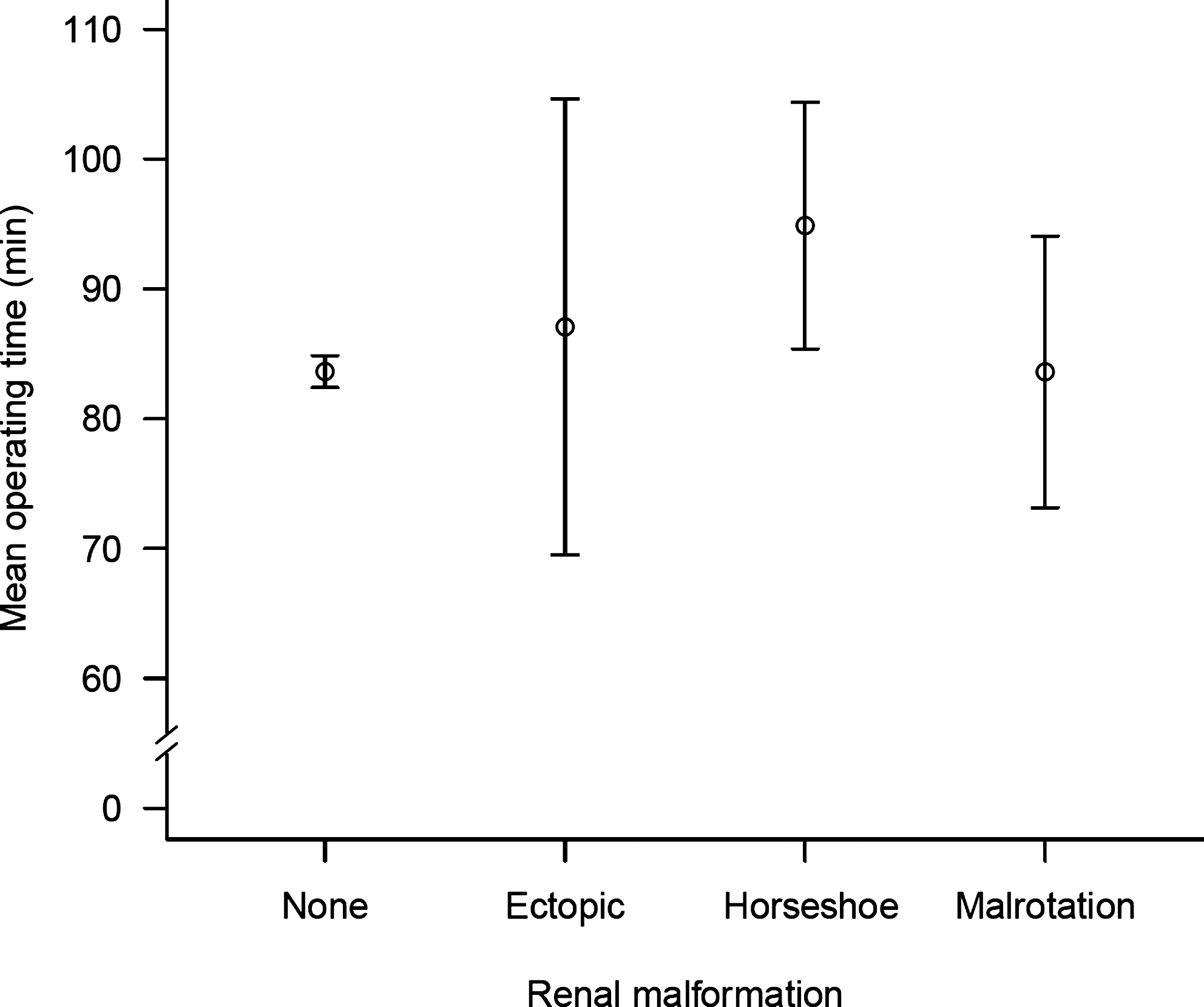
Duration of surgery according to renal malformation. Data are shown as mean±95% confidence interval.

Comparison of modified Clavien score in patients with normal and malformed kidney. Data are shown as mean±95% confidence interval.
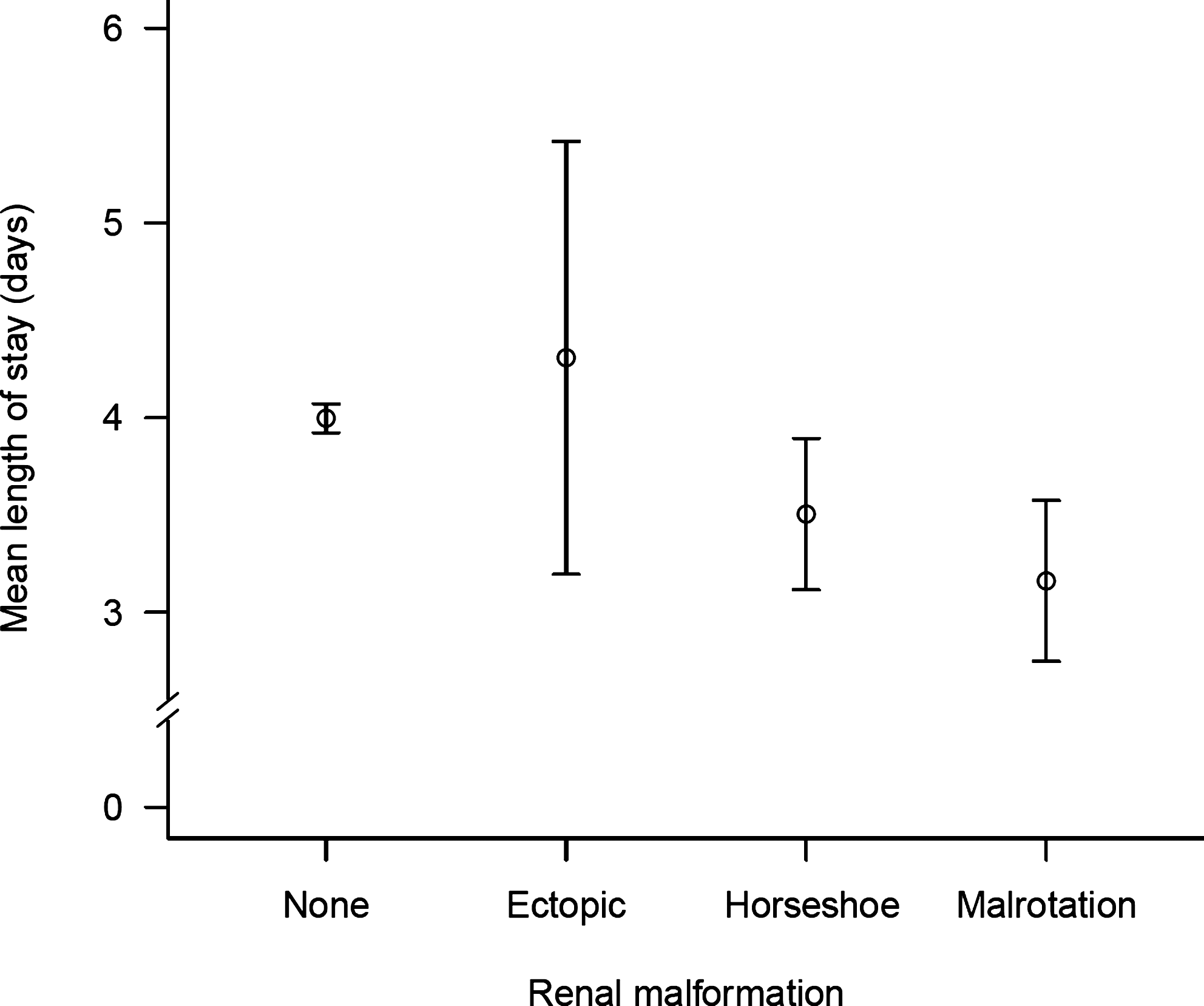
Duration of hospitalization according to renal malformation. Data are shown as mean±95% confidence interval.
Discussion
The CROES PCNL Global Study collected data from patients with a variety of indications for PCNL during routine clinical use in a wide range of clinical centers worldwide. To the best of our knowledge, the study database of patients who were treated with PCNL is the largest to be reported to date. Similarly, the present study represents the biggest series of patients with renal malformation undergoing PCNL for stone removal to be described to date. Consistent with known epidemiology of kidney malformations, 15 renal anomalies were found more frequently in males than in females. Horseshoe kidney, the most frequent kidney malformation seen in this study, has been reported as occurring twice as frequently in males than in females. 16 Overall, the renal stone burden was higher in anomalous kidneys than in normal kidneys. Because the presence of a large or complex stone is likely to have been the indication for PCNL, a high stone burden across the study is not unexpected. In contrast, staghorn calculi were encountered less commonly in anomalous kidneys. Previous studies have reported successful PCNL in anomalous kidneys with stone sizes of mean surface area of 450 to 920 mm2 and with individual stone burdens as high as 4900 mm2. 17 –21
The results show that the duration of surgery for PCNL removal of stones from malformed kidneys was longer than for PCNL on normal kidneys. This probably reflects the greater care taken by the surgeon or urologist in adapting the surgical technique to the abnormal anatomy of malformed kidneys. Abnormal renal position, abnormal renal and caliceal orientation, abnormal relationships of the calices to the renal pelvis and upper ureter, aberrant renal vasculature, relative renal immobility, and atypical relationships between kidney and other organs are all factors for concern in urologic procedures involving kidney abnormalities. 8,10
The study revealed that patients with renal anomalies underwent PCNL more frequently in the prone position and this was particularly noted for those patients with horseshoe kidneys. The prone position allows upper pole puncture to be performed more easily. It follows therefore that upper pole percutaneous access was performed in markedly more patients with a renal malformation than those with normal kidneys. In the horseshoe kidney, upper pole access is generally preferred because it allows access to the upper pole calices, renal pelvis, lower pole calices, pelviureteral junction, and proximal ureter and it is closer to the skin. Upper pole access can also decrease blood loss and can generally be performed via a subcostal approach. 18,22 Some studies have reported use of upper caliceal puncture in all patients with a horseshoe kidney. 8 Lower caliceal puncture may be more appropriate for PCNL access of malrotated kidneys. 8,10 In clinical practice, which is reflected in the results of the present study, the choice of puncture site needs to be made according to the anatomy of each kidney and the urologist's or surgeon's preference and may only be finally determined intraoperatively during dynamic visualization.
The trend toward more frequent use of fluoroscopy and ultrasonography together to guide puncture of anomalous kidneys is consistent with the care needed to avoid injuring aberrant vessels or overlying abdominal viscera and nerves. Other guidance techniques used with PCNL include laparoscopy, which permits direct visualization of the kidney, to facilitate safe puncture and tract placement. 23 Laparoscopic-assisted PCNL has been used successfully in stone removal from ectopic pelvic kidneys. 7,8 Because a significant number of horseshoe kidneys are associated with ureteropelvic obstruction, one may consider a laparoscopic approach in these circumstances and combine the stone removal with ureteroplasty rather than performing PCNL only. 24
The similar frequency of common complications in the two patient groups supports the observation that with appropriate care, PCNL can be accomplished as safely in abnormal kidneys as in normal kidneys. Similar rates of successful stone clearance also support this observation. Identical low rates of perforation of the renal pelvis indicate that although the procedure is demanding in anomalous kidneys, technically it is surmountable as also observed elsewhere. 8,18 The now widely implemented upper pole puncture in patients with renal anomalies might also be an explanation for the lack of increased complication rates. The absence of any cases of colonic injury is also noteworthy; several previous reports have suggested a higher incidence of this complication for patients with horseshoe kidneys undergoing PCNL. 25
The proportion of procedures that failed to gain satisfactory access to the collecting system, although low, was higher in abnormal kidneys. This suggests that further adaptation of the PCNL technique is needed in some centers. Full radiologic evaluation and surgical planning are essential in all PCNL cases. The choice of caliceal puncture should be selected according to the anatomy of each renal unit and the urologist's judgment. An important technical modification needed for performing PCNL in the horseshoe kidney, for example, is the establishment of the nephrostomy tract in a more inferior and medial position than normal. 22
The results show that the stone burden in all three types of renal anomalies was higher than in normal kidneys, and was highest in malrotated kidneys. Despite this, mean operative time in the malrotated kidney group was similar to that of the normal kidney group (approximately 84 min). Operative times were longest in the horseshoe kidney group (approximately 96 min), suggesting a greater complexity of the procedure in this group, including more difficulties in gaining access, need for greater reliance on flexible nephroscopy, and laser intracorporeal lithotripsy. For comparison, Mosavi-Bahar and associates 8 reported mean operating times of 56 min for horseshoe kidney, 61 min for malrotated kidney and 121 minutes for ectopic kidney.
Mean hospital stay of patients was 3 days in both normal and abnormal kidney groups. This is similar to that reported by other studies of normal and abnormal kidneys. 7 –9,22 Within the abnormal kidney group, length of stay was longest for patients with ectopic kidneys and shortest for those with a malrotated kidney, which probably reflect the degree of abnormality.
Several small studies have reported that PCNL is a safe and effective treatment option for removal of renal stones, particularly those larger than 1.5 to 2 cm, 1,10 from horseshoe kidneys, 6,8 –10,21,22,26,27 malrotated kidneys, 8 –10 and ectopic kidneys. 1,7 –10,28 This study confirms the high efficacy and acceptable tolerability of PCNL as a minimally invasive procedure for the removal of renal stones in malformed kidneys. In addition, the study illustrates the potential usefulness of the CROES PCNL Global Study database as a source of readily analyzable clinical data from patients with relatively rare disorders who undergo PCNL.
Footnotes
Acknowledgment
The Global PCNL Study was supported by an unrestricted educational grant from Olympus.
Disclosure Statement
H. Razvi is a consultant for Cook Urological and Olympus-Gyrus. He has research collaborations with Nerites Corporation and Allergan. T. Averch acts as a consultant for Bard Urologic. The remaining authors have no competing financial interests.