
Abstract
Background and Purpose:
Robot-assisted laparoscopic pyeloplasty has become more widely used. Intraoperative placement and confirmation of ureteral stent position can be cumbersome with the robotic arms in place. We present a technique of percutaneous antegrade stent placement that is reliable with minimal morbidity.
Patients and Methods:
A retrospective cohort study was performed. Patient demographics, radiographic imaging, intraoperative details, and surgical outcomes were abstracted from the medical record. A 14-gauge angiocatheter was placed through the abdominal wall. A ureteral stent was guided over a wire down the dismembered ureter. Stent position was confirmed by retrograde reflux of methylene blue. A urethral catheter was left in place for 12 to 36 hours.
Results:
Twenty-nine patients (15 male, 14 female) were identified. Average age was 10 years. Average follow-up was 14 months. Fifteen left- and 14 right-sided procedures were performed. Two patients needed retrograde stent placement. Mean time to correctly position the stent was less than 5 minutes. Postoperatively, one patient had a urine leak managed by an indwelling urethral catheter and did not need percutaneous drainage. All stents were removed approximately 4 to 6 weeks postoperatively. One patient had retrograde migration of the stent managed by ureteroscopy at the time of stent retrieval.
Conclusions:
Antegrade ureteral stent placement through a percutaneous angiocatheter, during robot-assisted laparoscopic pyeloplasty, is a rapid and effective technique. Intraoperative confirmation of stent position can be obtained, using methylene blue bladder distention, without repositioning the patient or undocking the surgical robot.
Introduction
We present a technique of percutaneous antegrade stent placement that is reliable with minimal morbidity and does not necessitate patient repositioning.
Patients and Methods
A retrospective cohort study was performed of all patients who were treated at a single institution with robot-assisted laparoscopic dismembered pyeloplasty. The procedure was performed by one of three treating surgeons. Inclusion criteria included severe hydronephrosis (Society for Fetal Urology grade III or IV) and an obstructed washout pattern on a well-tempered diuretic renogram. Indications for operative intervention included asymptomatic delayed washout on diuretic renography, pain, stones, and infection.
The majority of patients presented with intermittent flank pain. No patient was excluded from antegrade stent placement because of the severity of hydronephrosis. We do not believe our patient population is a favorable cohort for antegrade stent placement. Patient demographics, radiographic imaging, intraoperative details, and surgical outcomes were abstracted from the medical record.
The patient was positioned in a modified lateral decubitus position. An 8-mm robotic camera trocar was placed into the peritoneal cavity, after access was obtained using a Veress needle through a curvilinear incision just below the umbilicus. Two additional 5- or 8-mm working ports were placed in a triangular configuration approximately 8 to 10 cm from the camera port under laparoscopic guidance. The da Vinci S HD surgical system robot (Intuitive Surgical, Inc, Sunnyvale, CA) was then docked to the trocars, and the operating surgeon then performed the procedure from the console.
The renal dissection was performed through a transmesenteric approach if feasible or after mobilizing the colon at the white line of Toldt. The UPJ was dismembered in all cases. The ureter was transposed anterior to lower pole crossing vessels when present. The proximal ureter was spatulated for intrinsic obstructions, and the anastomosis was performed with running 6-0 or 5-0 monofilament absorbable suture.
Intraoperatively, the stent was placed after the apical and posterior portion of the anastomosis was completed. Antegrade stent placement was amenable, regardless of the degree of hydronephrosis, at some point during the anastomosis. The bladder was filled to approximately 50% to 75% of calculated bladder capacity with methylene blue through a sterile Y-connector to the urethral catheter by the circulating nurse. A percutaneous 14-gauge angiocatheter was placed through the abdominal wall under direct laparoscopic guidance by an assistant at the bedside (Fig. 1A).
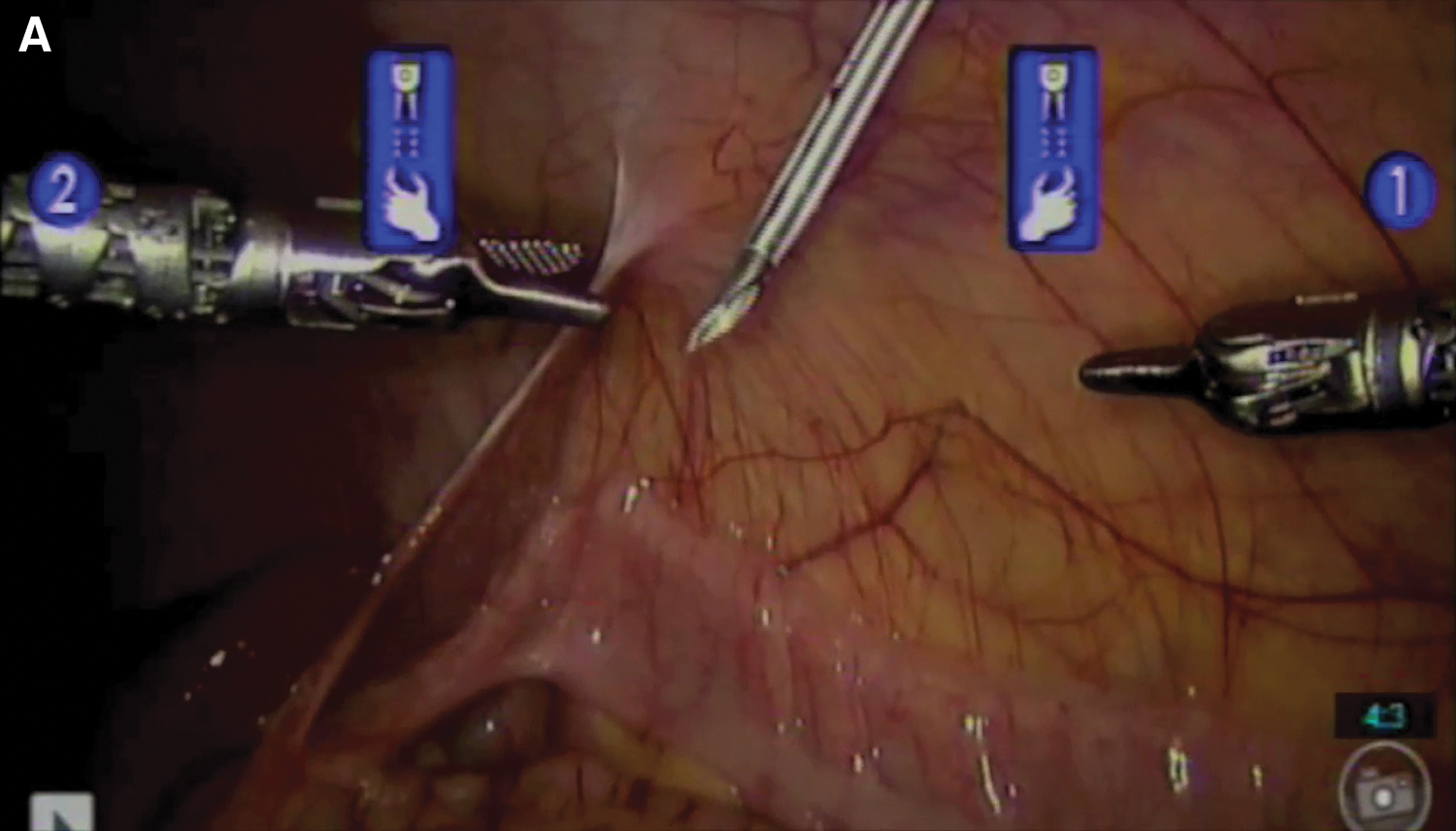
Angiocatheter introduced percutaneously into the abdomen under direct vision.
The surgeon then used a grasper to guide the ureteral stent over a guidewire down the dismembered ureter into the bladder (Figs. 1B, 1C). The stent position was confirmed to be in the bladder by retrograde reflux of the dye along the stent. The guidewire was removed, and the proximal loop of the stent was placed into the renal pelvis (Fig. 1D). The anterior portion of the anastomosis was then completed in a watertight fashion. No perinephric drain was routinely used.
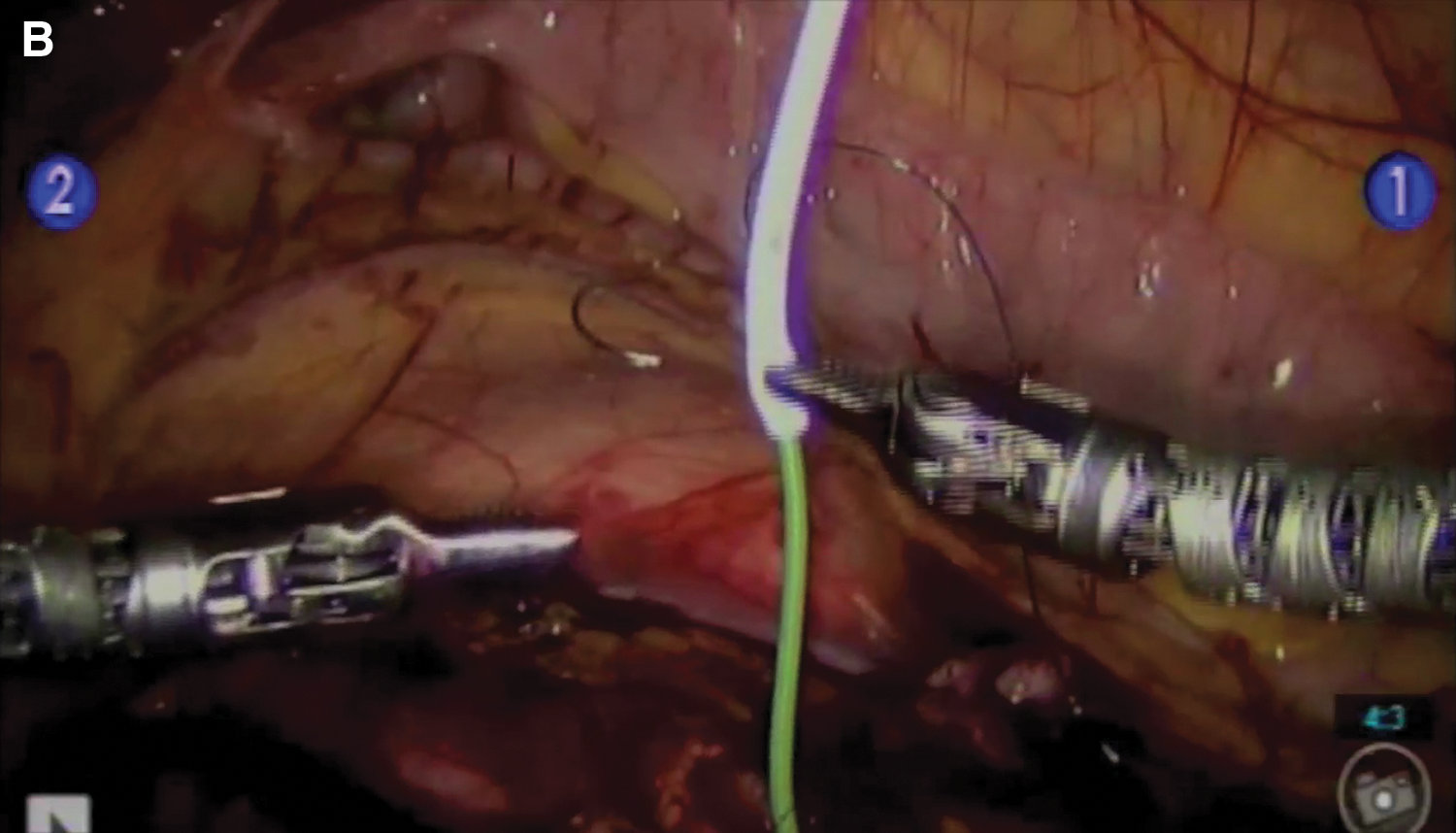
Passing distal end of ureteral stent antegrade over a guidewire.
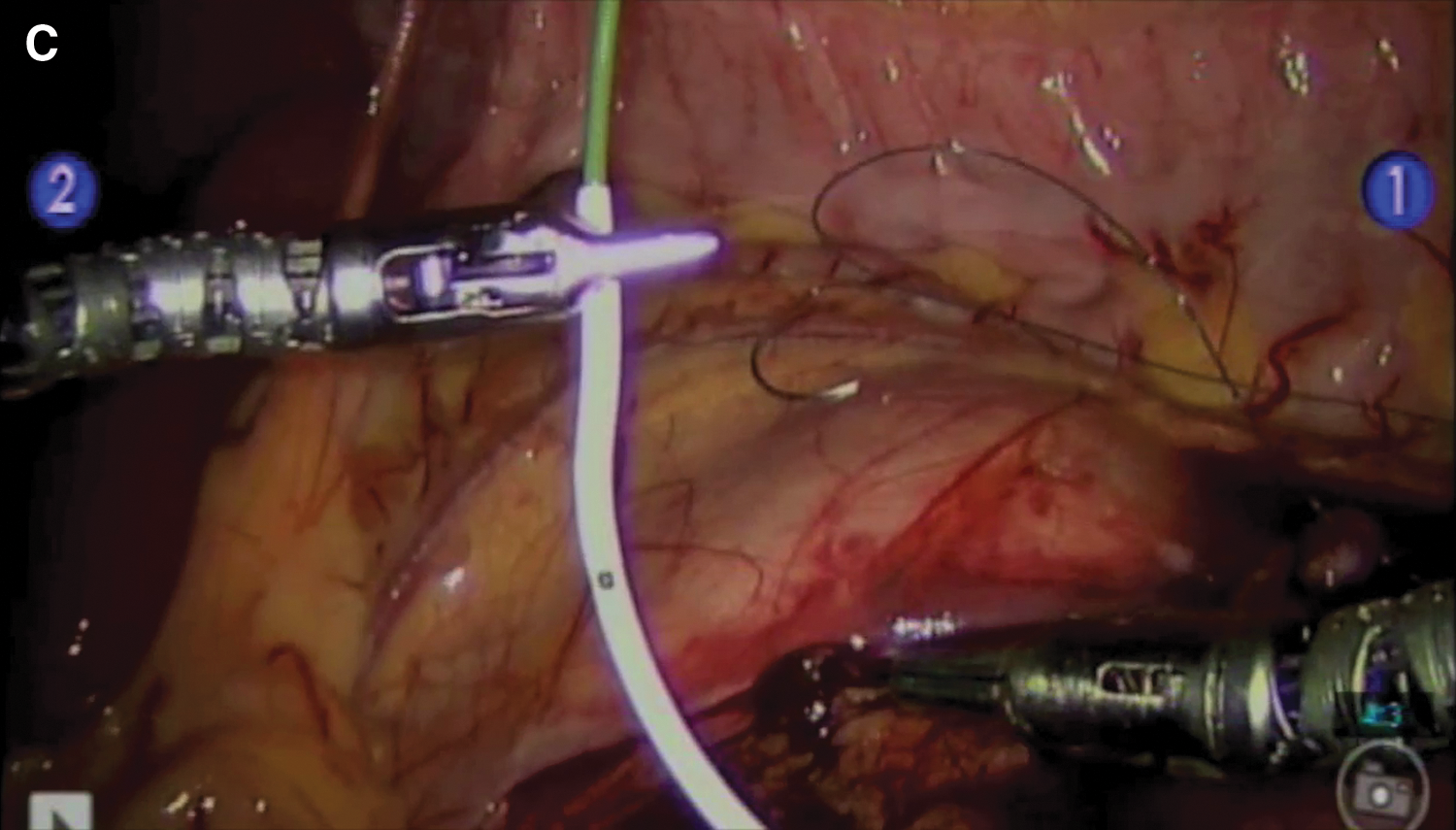
Removing guidewire while holding proximal end of ureteral stent in place.
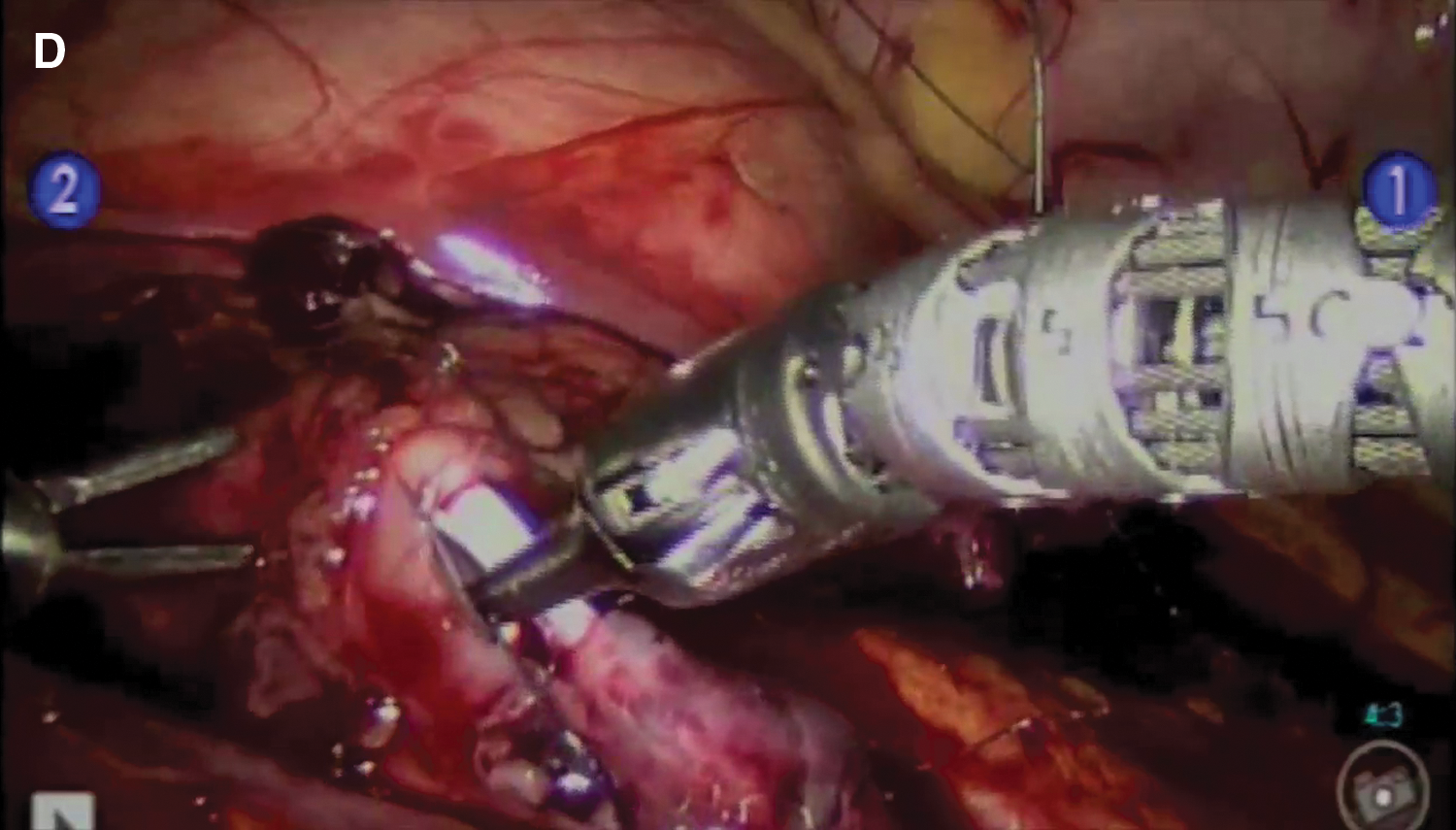
Proximal end of ureteral stent positioned into renal pelvis.
Stent size was chosen by surgeon preference. In the prepubertal population, a general rule for estimating length of stent was using age plus 10, for length in centimeters. Variable length stents were also used for older patients.
A urethral catheter was left in place for 12 to 36 hours, and then the patient was discharged home from the hospital with oral prophylactic antimicrobial coverage. The ureteral stent was removed via cystoscopy 4 weeks postoperatively under a brief anesthetic. Follow-up renal ultrasonography was performed 1, 3, and 6 months after stent removal. Diuretic renography was not routinely performed postoperatively.
Results
A total of 29 patients (15 males and 14 females) were identified from 2009 to 2010. Average age was 10 years (range 19 mos–18 y), and average follow-up was 14 months. All patients had diuretic renography and sonographic confirmation of UPJ obstruction. No robotic cases were excluded. Fifteen left-sided and 14 right-sided procedures were performed. The etiology of obstruction was intrinsic in 38% and lower pole crossing vessels in 62%.
One patient had a complete ureteral duplication with a lower pole UPJ from a crossing vessel. Two patients had ureteral polyps at the UPJ that were excised at the time of repair. One patient had 10 small calculi in the lower pole of the kidney successfully extracted via basket by manipulating a flexible cystoscope through a trocar into the dismembered renal pelvis.
Laparoscopic access complications included one patient who had a small abdominal wall hematoma from port placement close to the inferior epigastric vessels. A morbidly obese patient (body mass index 35) had dislodgment of the umbilical port during robot docking and needed undocking to reinsert the trocar. There were no other intraoperative complications. Blood loss was minimal in all cases.
A total of 26 (90%) patients had successful antegrade stent placement at the time of pyeloplasty. Timing of stent placement was started with placing the angiocatheter. Mean time to correctly position the stent was less than 5 minutes. Average included all attempts of antegrade placement. Stent size was not changed based on the methylene blue dye. Methylene blue was used as an adjunct in this technique and was not the sole factor in assessing a successful placement. Two patients needed retrograde stent placement because of unsuccessful antegrade placement. Both cases of unsuccessful placement were complicated by congenital distal obstruction. One 19-month-old patient had a stentless procedure. Postoperatively, one patient had a urine leak managed by an indwelling urethral catheter and did not need percutaneous drainage. There were no cases of inadvertent passage of the stent down the urethra.
All patients had the stent successfully removed at the time of cystoscopy 4 to 6 weeks postoperatively. One patient had undiagnosed retrograde migration of the stent after hospital discharge that was managed by ureteroscopy at the time of stent retrieval. In this case, postoperative imaging at the end of the pyeloplasty documented good position. There were no cases of recurrent UPJ obstruction by follow-up ultrasonographic imaging and no symptomatic urinary tract infections. The patient with the multiple lower pole stones extracted at the time of pyeloplasty underwent extracorporeal shockwave lithotripsy 6 months postoperatively for a persistent 6-mm stone on follow-up plain abdominal radiography.
Discussion
The open Anderson-Hynes dismembered pyeloplasty has been the gold standard in the operative management of pediatric UPJ obstruction for many years. In the past few decades, less invasive laparoscopic and robot-assisted laparoscopic approaches have become more widely used. An indwelling ureteral stent placed at the time of repair has both its advocates and detractors, and outcomes have been reported in several observational studies. 1,2 Retrograde and antegrade ureteral stent placements have both been advocated, with the retrograde approach more widely used. 3 –7 As minimally invasive approaches for pyeloplasty have proliferated and become more commonly performed, surgeons have continued to modify techniques to use a ureteral stent. 8 –19 Factors taken into consideration include ease of stent placement, reliability of technique, and time needed for stent placement.
At our institution, a transperitoneal approach is selected during robot-assisted laparoscopic pyeloplasty because of the working space advantage over a retroperitoneal approach. This is especially pertinent in the pediatric population. As other investigators have reported, 3,7,11 we also prefer an initially unstented upper urinary tract to facilitate dissection by avoiding a decompressed renal pelvis. An alternative to prestent placement includes leaving a guidewire or leaving a ureteral catheter below the UPJ. 18,19 Performing these maneuvers would necessitate cystoscopy at the beginning of the procedure.
Antegrade stent placement has been shown to take a shorter time than retrograde stent placement. 6 Our experience has also been that performing cystoscopy with retrograde ureteropyelography, with or without ureteral stent placement, adds a significant time under anesthesia for the patient. This has been because of the time it takes to move equipment around in the operating room, including the C-arm fluoroscopy machine, and reposition the patient for the pyeloplasty. We prefer antegrade ureteral stent placement because of the ease of technique, high success rate, and limited time needed to successfully place the stent.
During open pyeloplasty with antegrade ureteral stent placement, our group has used methylene blue in a distended bladder to facilitate confirmation that the distal end of the ureteral stent is in the bladder. The dye is seen refluxing out of the anastomosis once the stent has passed the ureterovesical junction into the bladder. Because of this positive experience with open pyeloplasty, the modification was incorporated into our approach for stent placement during laparoscopic pyeloplasty.
Confirmation by using dye may obviate additional equipment, such as an intraoperative ultrasonography, which has been reported to help confirm appropriate stent positioning in the bladder. 20 It can also avoid the need for fluoroscopy, 19 which would be impractical for robotic procedures while the robot is still docked to the trocars. Additional time would be needed to undock and redock the robot for fluoroscopy, or to wait until the end of the procedure when options to manipulate the ureteral stent are limited or lost.
This technique for percutaneous antegrade ureteral stent placement, using an angiocatheter with methylene blue bladder distention, is simple, reproducible, and reliable. Dismembering and starting the anastomosis is facilitated by not having to work around an indwelling ureteral stent. The stent can then be placed near the completion of the repair when only the anterior wall of the anastomosis is yet to be performed. Manipulating and passing the stent antegrade are greatly facilitated by robotic assistance.
As more effort is made to continue to decrease the morbidity of surgical procedures, an angiocatheter is an excellent way to minimize trocar use and improve cosmesis by reducing visible scarring. In addition to introducing ureteral stents and guidewires, we have used it as a vent to release smoke from electrocautery, as has also been demonstrated by Hotaling and associates. 21 It is also likely to reduce postoperative pain by avoiding an extra trocar, and the puncture site is virtually unnoticeable. We have found that using dye is a helpful adjunct in successful placement.
A disadvantage of this technique is that it has not been successful in every case. This is inherent in the pediatric population, especially infants and toddlers, when small size or concomitant pathology can preclude any ureteral stent placement. In these infrequent circumstances, a retrograde approach, nephrostomy tube placement, or stentless approach can be used. A retrograde stent placement across a new anastomosis is a potential disadvantage, with the inherent concerns regarding disruption of the anastomosis. As with ureteral stents left indwelling without dangling strings for removal, a disadvantage is the second anesthetic to remove the foreign body.
Limitations of this study include the inherent nature of retrospective chart reviews, including lack of a control group, randomization, and blinding. In addition, the small number of patients in this pilot study allows for little statistical analysis or analysis of confounding factors. Further study with larger numbers of patients and longer follow-up are necessary to completely evaluate the safety and efficacy of this procedure.
Conclusion
In our experience, antegrade ureteral stent placement through a percutaneous angiocatheter during robot-assisted laparoscopic pyeloplasty is a rapid and effective method for bridging the repair. Intraoperative confirmation of stent position can be obtained, using methylene blue bladder distention, without repositioning the patient or undocking the surgical robot. Further study is necessary to confirm these preliminary findings.
Footnotes
Disclosure Statement
No competing financial interests exist.