
Abstract
Background and Purpose:
Laparoscopic partial nephrectomy (LPN) paralleling open techniques, particularly closure of the collecting system, can be technically challenging for the novice laparoscopist. We describe operative results and complications of a single surgeon, retrospectively reviewed series using a simplified method of hand assistance and a fibrin glue patch for hemostasis without formal collecting system closure.
Patients and Methods:
We identified 104 consecutive patients between September 2003 and January 2009 who underwent hand-assisted laparoscopic partial nephrectomy (HALPN). Our technique involves routine hilar clamping after isolation of the tumor and mobilization of the kidney. After resection of the mass, a fibrin glue patch is placed within the surgical defect and secured with bolstering sutures. No attempt is made to suture the collecting system, nor are ureteral catheters placed when the collecting system is entered during resection of the tumor.
Results:
Mean tumor size was 2.8 cm (median 2.5 cm, range 0.7–7.0 cm). With hilar clamping, warm ischemia time averaged 24.5 minutes (range 11–39 min). Estimated blood loss averaged 220 mL (range 50–1500 mL), and five (4.8%) patients received transfusions either intraoperatively or postoperatively. Urine leak occurred in 1.9% (n=2) of patients overall and 4.3% (2/47) of patients with documented collecting system entry. Both urine leaks resolved with conservative management only.
Conclusions:
HALPN without formal collecting system closure is a safe and effective technique with similar urine leak and transfusion rates compared with other series. This technique may allow more urologists to perform minimally invasive partial nephrectomy or to do so with potentially shorter ischemia times.
Introduction
Compared with the open approach, LPN in most series is associated with longer ischemia times and higher complication rates. 1,3,4 Increased incidence of postoperative bleeding and urine leak from the renal remnant have been noted with LPN compared with open partial nephrectomy (OPN). 5 The increased rate of these complications may be attributable to the challenges of maintaining hemostasis and closure of the collecting system when entered during LPN. Efforts to mimic open techniques, such as formal vascular and collecting system closure, can be time consuming and difficult, particularly for surgeons with less laparoscopic experience. As a result, data suggest a trend toward increased use of laparoscopic radical nephrectomy at the expense of partial nephrectomy. 6,7
We examine our perioperative outcomes with a simplified technique for hand-assisted laparoscopic partial nephrectomy (HALPN) using an absorbable gelatin sponge (Gelfoam,™ Pharmacia and Upjohn Co, Kalamazoo, MI) soaked in fibrin glue (Tisseal,™ Baxter Inc., Deerfield, IL) and suture bolstering without formal collecting system closure in 104 consecutive patients.
Patients and Methods
After Institutional Review Board approval, retrospective review of two hospitals was performed to identify HALPNs performed by a single surgeon (SES) between the years 2003 to 2009. The time frame represents a consistent technique of a hand-assisted, transperitoneal approach to LPN with use of a hemostatic bolster, and no collecting system suturing. Nephrometry scores were determined in patients with available preoperative imaging. 8 Urine leak was defined as elevated fluid creatinine level of persistent drain output. 9 Because all patients had fluid from the drain sent for analysis postoperatively, a urine leak was diagnosed if a patient had persistent drain output with elevated fluid creatinine level at the time of discharge. Those patients who had either no significant output, fluid creatinine level similar to serum level, or both, had their drains removed before discharge.
The HALPN technique used has been described in detail elsewhere. 10 Briefly, after the patient is positioned in a modified flank position, intraperitoneal access is gained through a midline incision around the umbilicus. A hand port is inserted, and two additional 12-mm ports are placed in the midclavicular line and the anterior axillary line off the tip of the 12th rib. When deemed necessary for suction or retraction, an additional 5-mm port is placed below the costal margin in a triangular fashion with the 12-mm ports. The colon is mobilized, the renal hilum is exposed, and the Gerota fascia is opened transversely. The kidney is exposed completely while the perinephric fat overlying the lesion is left in situ.
Before hilar clamping, 12.5 g of mannitol is administered, and hook electrocautery is used to make a circumferential capsulotomy around the mass. Hilar clamping using a vascular hand-held bulldog clamp is used routinely, with exceptions for solitary kidneys or particularly exophytic lesions. The resection is deepened using cold scissors, with hilar fat frequently visualized, while the more central portion is resected with scissors or ultrasonic shears for control of vessels when encountered (Fig. 1). The specimen is immediately brought out through the hand port and sent for frozen section analysis. The parenchymal edges of the resection defect are then cauterized using Argon beam coagulation, followed by placement of an absorbable gelatin sponge patch (Fig. 2). The patch is made by folding a 100 cm2 (8×12.5 cm) piece of Gelfoam™ and soaking it with 5 mL of the fibrinogen component of fibrin glue (Tisseel™). The thrombin (5 mL) component is then injected into the gelatin foam to activate the fibrinogen once the patch is in place. No attempt is made to close the collecting system, even when it has clearly been entered. Absorbable 2-0 polyglactin bolstering sutures are placed to compress the renal parenchymal edges around the patch and hold it in place (Fig. 3). We secure the suture with Lapra-Ty™ clips, avoiding intracorporeal knot tying (Lapra-Ty,® Ethicon Endosurgery, Inc, Piscataway, New Jersey). 11
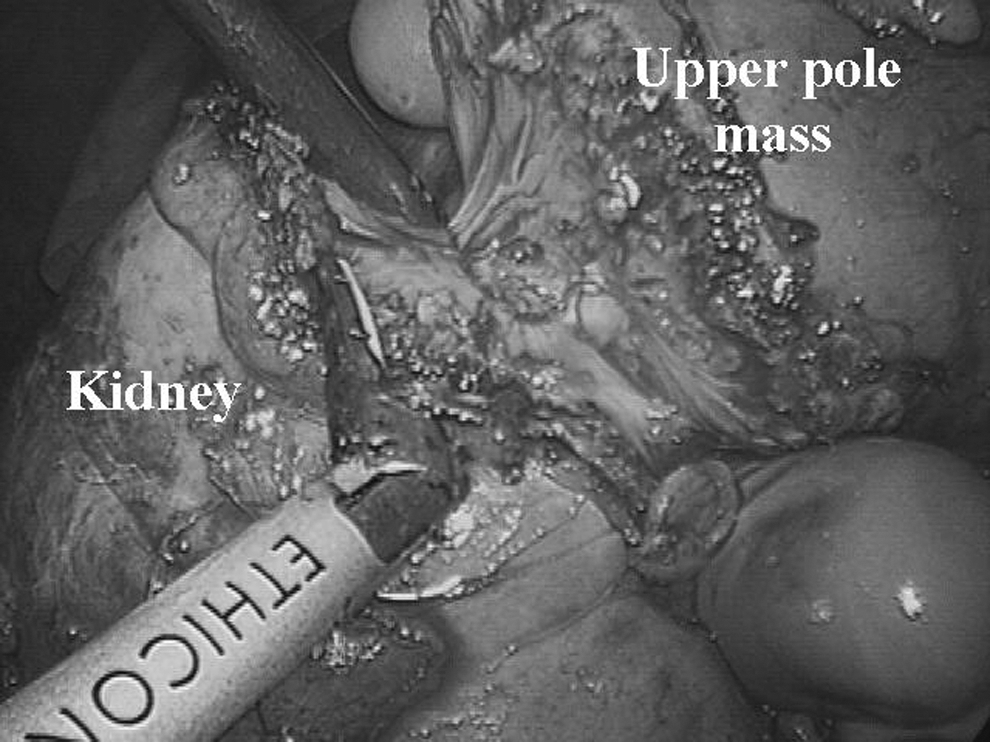
Deep resection of large endophytic right upper pole renal mass is performed using ultrasonic shears.

Fibrinogen-soaked gelatin sponge patch is placed in surgical defect and then activated with thrombin.

Bolster sutures are placed in a linear fashion across the surgical defect, incorporating the activated patch.
Once the bolstering is completed, the hilar clamp is released, the kidney palpated to assess for return of blood flow, the abdominal pressure decreased, and the resection defect observed to ensure adequate hemostasis. Perinepheric fat is then used to cover the resection site, and a Jackson-Pratt drain is placed adjacent to the renal remnant through the lateral trocar site. Ureteral stents are not placed before or during the procedure. Fluid creatinine level is obtained from the drain before its removal postoperatively. Standard outpatient follow-up consists of CT scan in all patients at 3 to 6 months postoperatively, with further imaging via ultrasonography or CT thereafter, depending on the clinical scenario.
Results
One hundred and four patients who met the inclusion criteria were identified. Patient demographics and tumor features are detailed in Table 1. Mean lesion size was 2.8 cm (median 2.5 cm, range 0.7–7.0 cm) on final pathology examination, and the majority (78%) of tumors were malignant. Mean warm ischemia time for kidneys that were clamped was 24.6 minutes (range 11–39 min). Thirteen (12.5%) of the 104 cases were performed without hilar clamping. Mean operative time from skin incision to closure was 188.8 minutes (median 187 min, range 99–323 min). Median length of stay was 3 days (range 1–8 d). Mean creatinine level increased from 1.0 mg/dL (median 1.0 mg/dL, range 0.5–3.0 mg/dL) preoperatively to 1.1 mg/dL (median 1.1 mg/dL, range 0.5–2.9 mg/dL) at discharge.
Perioperative complications, including urine leak, are demonstrated in Table 2. Within the entire series, postoperative urine leak developed in two patients (1.9%); both leaks resolved with continued drainage. Each drain was removed within 2 weeks of discharge without event. No secondary procedure, including ureteral stent or urethral catheter placement, was necessary for either patient. Fifty-one percent (53/104) of patients were documented in the operative report to have tumor resection down to the perihilar fat (6/53) or collecting system entry (47/53). Both patients in whom postoperative urine leak developed were noted to have collecting system entry at the time of surgery. Thus, a postoperative urine leak developed in 4.3% (2/47) of patients with documented collecting system entry at the time of HALPN.
MI=myocardial infarction.
Estimated blood loss averaged 220 mL (median 150 mL, range 50–1500 mL). Mean hemoglobin level decreased from 14.3 g/dL (median 14.4 g/dL, range 9.7–17.5 g/dL) preoperatively to 12.1 g/dL (median 12.3 g/dL, range 7.2–16.0 g/dL) at discharge. Only 4.8% (5/104) patients needed blood transfusion during or after surgery. Two patients presented in a delayed fashion with hematuria. One presented 3 months after surgery with significant hematuria and was found to have a pseudoaneurysm, which was managed with selective embolization. The second patient had gross hematuria presumed to be from the renal remnant that resolved without any intervention. No renal units were lost perioperatively because of surgical complications, nor were any found to be nonfunctioning at follow-up based on clinical data and imaging.
Discussion
As emphasized in the recent American Urological Association guideline for the mnagement of small renal masses, nephron-sparing approaches should be used whenever feasible in the management of the clinical T1 renal mass to preserve renal parenchyma and avoid chronic kidney disease. Concerns about the increased warm ischemia times and higher complication rates reported in the literature led the panel to maintain that OPN remains the standard of care, while potential advantages of minimally invasive surgery must be carefully weighed against the greater risk of complications and longer ischemia times. Furthermore, the panel acknowledged that there will likely be an increasing application of these approaches as minimally invasive instrumentation improves and expertise becomes more disseminated. 1
Nevertheless, there is concern that the application of minimally invasive surgery in the form of laparoscopic nephrectomy is sometimes replacing the option of OPN for certain patients. 6,7 As the clinical scenario of an incidentally found clinical T1 renal mass becomes ever more common for today's urologist, we propose a technique that allows more broad application of minimally invasive nephron-sparing surgery for these patients while maintaining a low complication rate and limiting ischemia time. In many areas where it is available, the robot-assisted approach is also gaining acceptance as a means to provide a minimally invasive approach to nephron sparing. 12,13
Traditionally, during OPN the collecting system is formally closed with sutures. Maintaining this technique laparoscopically results in leak rates from 1% to 50%, depending on the series, tumor location, and size of the tumor resected. 14 –16 Laparoscopic or robotic closure of the collecting system and vascular structures typically involves one deep row of sutures placed in the resection bed followed by a second more superficial layer, while individual vessels or areas of entry into the collecting system may not be specifically sutured. 17 The collecting system was not formally closed in any of the 104 patients in our series. Urine leaks developed in two (1.9%) patients, neither of whom needed a ureteral stent. This is comparable to other large series (LPN 3%, OPN 1%, robot-assisted LPN 1.6%) 3,12,18 in which collecting systems were formally closed, as well as to those seen in a comparison of fibrin glue alone (9%) vs fibrin glue with suture bolster and suturing of the collecting system (2%). 19
Tissue sealants are gaining in popularity in many areas of surgery, including urology. They have been used to close collecting system defects and improve hemostasis, demonstrating favorable results in porcine models and humans. Pruthi and colleagues 20 discussed their experience in 15 patients using Tisseal fibrin sealant placed directly on the PN defect without any formal collecting system closure. No leaks were noted postoperatively, and there were no immediate or delayed complications with a follow-up of 12 to 60 weeks. Patel and coworkers 21 evaluated the ability of an absorbable gelatin sponge patch soaked in fibrin glue to seal collecting system injuries up to 1 cm in a porcine model. No leaks were noted at supraphysiologic pressures of 50 cm H2O. Kouba and colleagues 22 evaluated the vascular and pelvicaliceal burst pressures in a porcine model after PN, using application of Tisseal with hardening for 10 and 60 minutes. Burst pressures on average were 378 and 166 mm Hg for the renal vascular and pelvicaliceal systems, respectively, and were not affected by hardening times.
Our series of patients with the current technique also further confirms that a fibrin glue patch maintains good hemostasis with low delayed bleed rates (1.9%) that are comparable to series in which more complicated closure is performed. 14 We routinely ensure good hemostasis before closing by lowering intra-abdominal pressure and confirming that the kidney is once again firm with the return of blood flow. One of the patients with a delayed bleed was found to have a pseudoaneurysm, which necessitated angiographic embolization 3 months after the procedure. Singh and Gill 23 proposed two theories on the formation of pseudoaneurysms: End-on or partial transaction of an artery was thought to represent the most likely cause; less likely, they concluded, was the possibility that inaccurate placement and replacement of needles during suturing of the collecting system may have contributed to formation. The lack of suturing the collecting system and passing needles through the central portions of the kidney with our technique may contribute to the low rate of pseudoaneurysm observed in the current series.
Warm ischemia time is believed to be an important determinant of injury to the renal remnant. For LPN or robot-assisted LPN, reconstruction of the renal remnant after excision of the mass is typically the most time-consuming portion of the case. As a result, there have been many techniques described to try to expedite this process. Nguyen and Gill 24 notably describe a technique of early unclamping after a layer of deep suture closure is placed that allows for a decrease in clamp time to only 14 minutes. This, of course, requires expertise that is not widely had to complete the resection of the mass followed by intracorporeal laparoscopic suturing. The “sliding-clip renorrhaphy” technique has now been widely adopted as another means to shorten warm ischemia time related to renal reconstruction in the setting of robot-assisted LPN. 12,25
Warm ischemia time in our series averaged 24.6 minutes, which compares favorably with other recent published series of “pure” or robot-assisted LPN. 12,18 It does not, however, represent a significant improvement over most of them. This we attribute to the fact that this technique allows the procedure to be performed by residents and fellows, whose experience likely is more consistent with a typical urologist than that of a high-volume laparoscopist at a tertiary referral center. Therefore, we believe our data suggest that our technique will allow urologists who would otherwise offer a patient OPN the capability to perform minimally invasive nephron-sparing surgery while still maintaining acceptable ischemia times. For those already using a minimally invasive approach, with or without robot assistance, our findings suggest a potential tool to decrease the clamp time for such cases.
This study is limited by its retrospective nature and the inaccuracies that are inherent in retrospective data recovery. Furthermore, spanning more than 5 years, this series encompasses the learning curve of one surgeon at two institutions. Nonetheless, the series shows this technique to have similar rates of complications when compared with more technically challenging techniques.
Another limitation is the lack of data to specifically address distance from the collecting system. Because of our comfort with this technique, we are willing and able to approach larger and more central lesions without excessive concern. As such, this series has a fairly representative distribution of tumors, in terms of size and location, with more aggressive resections common later in the series. We did attempt to mitigate this by also showing a low leak rate in patients in whom the collecting system was described to have been clearly entered during the operation based on operative reports.
Some will certainly think that placement of a hand port is unnecessary for a PN. While this may be true, the hand port simplifies the technique for the novice laparoscopist and may add a degree of comfort that can be invaluable, especially if one were to encounter hemorrhagic complications intraoperatively. 6 The hand port also allows simple and expeditious removal of the specimen for frozen section analysis before beginning closure of the defect. Those urologists for whom a pure laparoscopic or robot-assisted approach is preferred may certainly apply the same closure technique by inserting the bolster through a 12-mm port and completing the renorrhaphy as described. This approach is gaining popularity in our institution.
Conclusions
LPN can be a difficult procedure for the novice laparoscopist. Our technique of HALPN with use of a fibrin-soaked absorbable gelatin foam patch with bolstering sutures eliminates suturing of the collecting system, which is arguably the most intimidating and difficult portion of the procedure. This technique may allow more urologic surgeons to offer their patients minimally invasive nephron-sparing surgery safely with complication rates and operative outcomes consistent with open and other laparoscopic series. For those already using a minimally invasive approach, we provide a potential technique to decrease warm ischemia time while not sacrificing patient safety or perioperative outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.