
Abstract
Background and Purpose:
Laparoendoscopic single-site (LESS) surgery offers potential improvements in cosmesis and recovery over standard laparoscopy (SL). We report the factors with which patients are most concerned in choosing surgery and how these affect preference for LESS. In addition, we rate the satisfaction of scars after laparoscopy.
Patients and Methods:
Patients followed after a laparoscopic procedure completed two surveys. First, patients rated, on a 5-point Likert scale, the importance of pain, recovery time, cost, treatment success, scars, and complications in choosing surgery. In addition, they were asked their preference for LESS. In the second survey, the impact of scars on body image and cosmesis was assessed.
Results:
Seventy-nine patients (median age 54.8 years, 65% male and 35% female) were treated for malignancy (53), donation (15), and benign indications (9). Treatment success (4.71±0.81) and complications (4.22±1.16) were most important, followed by pain (3.43±1.21) and convalescence (3.65±1.11), P<0.05. Cost was rated 2.68±1.38, and cosmesis was 2.22±1.13 (P<0.005). Cosmesis score increased in females (2.59±1.08 vs 2.02±1.12), patients <50 years (2.59±1.09 vs 2.02±1.12), and benign surgical indication (3.33±1.12 vs 2.07±1.06), P<0.05. LESS was preferred in 30.4%, SL in 39.2%. Concern for cosmesis was associated with LESS preference (48.5% vs 17.8%, P=0.004). Sex, age, and surgical indication also influenced this. On the body image scale, patients scored a mean 18.8±1.5 of 20. Patients rated scar appearance 8.31±1.80 of 10.
Conclusion:
Patients who were treated with laparoscopy were most concerned with success and complication. Preference for LESS was influenced by concerns for cosmesis, sex, age, and surgical indication.
Introduction
Despite the potential benefits, much is unknown about the factors that influence patients to choose LESS. Furthermore, little is known about the impact of laparoscopic scars on urology patients. In this study, we survey patients regarding the factors most important to them in choosing surgery, including their preference for LESS or SL, and through use of a validated questionnaire, assess the impact of laparoscopic scars on patient perceptions of cosmesis and body image.
Patients and Methods
Patients returning to clinic after transperitoneal laparoscopy by a single surgeon completed two surveys, after consenting to participate in this Institutional Review Board-approved study. Exclusion criteria were as follows: Patients undergoing large extirpative procedures, multiple previous open abdominal surgeries, or major complications. Demographic data and perioperative data, including surgical indication, number of trocars, hospital stay, and complications, were collected.
Patients received explanations for both LESS and SL, aided by a diagram. In the first survey, patients were asked to independently rate on a 5-point Likert scale (1: not important, 5: very important) the importance of the following factors in choosing surgery: (1) pain, (2) convalescence, (3) cost, (4) treatment success, (5) cosmesis, and (6) complications (Appendix 1). In addition, patients were asked whether they preferred LESS or SL, assuming equivalence and then assuming the surgeon had less experience for LESS. Finally, they were asked their preferences, if LESS were associated with increased complication or failure. In the second survey, a validated cosmesis and body image impact survey was administered (Appendix 2), consisting of a body image scale (questions 1–5) and the cosmesis scale (questions 6–8), with high reliability for both (Chronbach α: 0.81 and 0.74). 14 –17 Two additional questions addressed overall impact of surgery. 16,17
Statistical analyses were performed using PASW 18 (SPSS Inc, Chicago, IL). Mean responses were calculated, and comparisons for sex, age, and surgical indication were made using t tests, one-way analysis of variance, and chi-square.
Results
Seventy-nine patients completed surveys (median age=54.8 y, interquartile range [IQR]=25.3, Table 1). There were 20.5% aged 18 to 35 years, 16.7% 35 to 50 years, and 62.0% >50 years; 65% were men, and 35% were women. Surgical procedures included 27 robotic prostatectomies; 11 laparoscopic radical, 4 simple, and 15 donor nephrectomies; 4 pyeloplasties; 10 robotic partial nephrectomies; 5 adrenalectomies; 1 cyst decortication; 1 ablation; and 2 others. These were classified into 53 malignancies, 15 kidney donations, and 9 benign indications. Forty-six patients had no previous surgery, 10 had laparoscopy, and 20 had an open procedure. Minor complications occurred in three patients (1 ileus, 1 fever, and 1 mild cellulitis). Disease recurred in two patients, and there were no graft failures.
IQR=interquartile range; EBL=estimated blood loss.
Factors important in choosing surgery
Mean importance of pain (3.43±1.21), convalescence (3.65±1.11), cost (2.68±1.38), success (4.71±0.81), cosmesis (2.22±1.13), and risk (4.22±1.16) differed (Fig. 1). Cosmesis was lower than all other factors, except cost (P<0.005). Success and risk were rated highest (P<0.001). Pain was higher than cost and scars (P<0.005), but similar to convalescence. Cosmesis was more important in women than men, 2.59±1.08 vs 2.02±1.12, P=0.033, at least moderately important in 52% women and 37% men, P=0.212 (Table 2). Pain was higher for women than men (3.96±1.06 vs 3.16±1.21, P=0.005), moderately important in 93% women and 67% men (P=0.011). Risk was rated higher in women than men (4.63±0.63 vs 3.98±1.32, P=0.018). There were no significant differences for treatment success (P=0.224), convalescence (P=0.884) or cost (P=0.140).
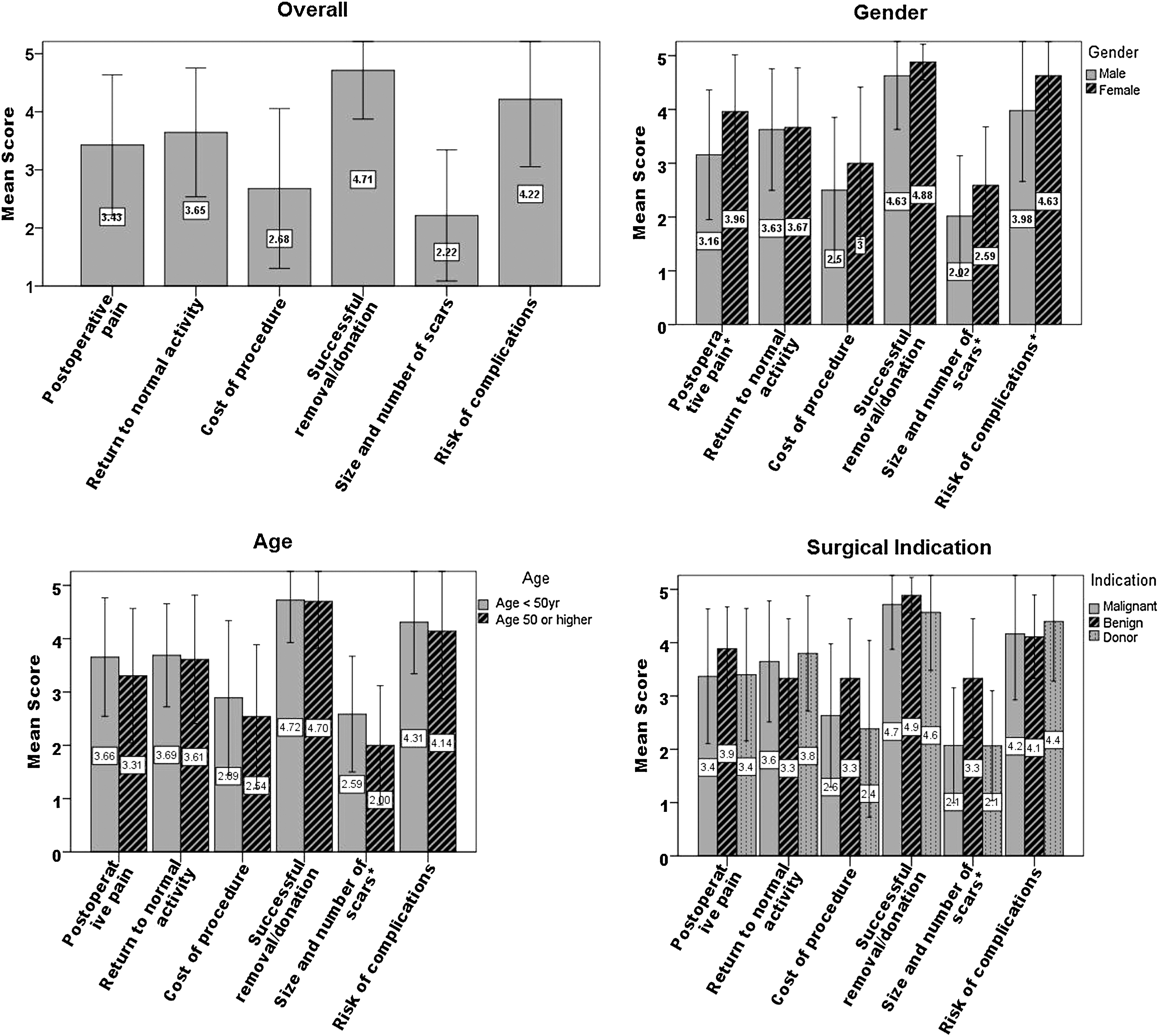
Mean scores for six factors rated by importance in making surgical choice overall, and stratified by sex, age, and surgical indication. *Denotes significant difference between stratified groups for that factor.
Mean scores for cosmesis for patients<50 years and patients ≥50 years were 2.59±1.09 and 2.02±1.12, P=0.027. Pain (P=0.221), convalescence (P=0.913), treatment success (P=0.913), complications (P=0.543), and cost (P=0.296) did not differ with age. Mean scores for cosmesis were 2.07±1.08 for cancers, 2.07±1.03 for donations, and 3.33±1.12 for benign cases (P<0.05, benign vs cancers or donations). Pain (P=0.496), convalescence (P=0.615), treatment success (P=0.682), complications (P=0.770), and cost (P=0.770) were not associated with surgical indication.
Preference for LESS
Thirty-one (39.2%) preferred SL, 23 (29.1%) had no preference, and 24 (30.4%) preferred LESS (1 did not answer). If the surgeon were credentialed but less experienced in LESS, 39 (49.3%) preferred SL, 20 (25.3%) had no preference, and 19 (24.1%) preferred LESS, (P<0.001). Of women, 38.5% (10/26) preferred LESS while 27.5% (14/51) men preferred LESS, P=0.324. Among patients <50 years, 35.7% (10/28) preferred LESS, while 28.6% (14/49) ≥50 years preferred LESS, P=0.515 (Table 3). Preference for LESS was observed in 29.6% (16/54) of cancers, 21.4% (3/14) of donors, and 55.6% (5/9) of benign cases (0.205). Among patients rating scars at least moderately important, 48.5% (16/33) preferred LESS, while 17.8% (8/45) of those who did not, P=0.004 (Table 3). When postoperative pain was at least moderately important, 33.9% (20/59) preferred LESS, while 21.1% (4/19) preferred LESS if it were unimportant (P>0.1). Of patients who rated convalescence time as moderately important (4/13) and unimportant (20/65), 30.8% each preferred LESS.
When asked whether one would accept an increase in complications to undergo LESS, 50.0% would accept no increase, 25.3% tolerated an increase from 1% to 2%, 11.4% an increase from 1% to 5%, 11.4% an increase from 1% to 10%, and 1.3% from 1% to 20%. Similarly, when asked whether one would prefer LESS even if it meant an increased risk in recurrence of treatment failure, 65.4% would accept no increase, 16.7% would accept an increase from 5% to 7%, 13.9% an increase from 5% to 10%, 2.5% from 5% to 15%, and 1.3% from 5% to 20%. Median risk for complications or failure acceptable was none for those not preferring LESS and an increase from 1% to 2% complications and 5% to 7% recurrence in those preferring LESS, P<0.005.
Scar satisfaction
Patients reported high body image scores (mean body image score: 18.8±1.5, of 20). Mean scores for the individual body image questions ranged from 3.41±0.96 (body satisfaction) to 3.95±−0.23 (difficult to look at oneself ), with only body satisfaction significantly lower than the rest (Fig. 2). A large negative impact on body satisfaction (score ≤2), P=0.087 was reported by 18.4% males and 4.0% females. Similarly, 18.8% patients older than 50 years vs 3.8% <50 years reported a large negative impact on body satisfaction, P=0.073. Finally, 19.6% malignant cases and no donor or benign case reported a significant negative impact on body satisfaction, P=0.033.

Mean scores reported for impact of surgical scarring on perceived body image.
No patient reported their body damaged or less attractive by a large amount (≤2), and scores were similar across sex, age, and surgical indication (P>0.05). Men (14.3%) and women (16.0%) felt a little less attractive (score=3, P=0.845). No significant difference in mean scores for decline in femininity/masculinity or difficulty in looking at oneself were observed for sex, age, or surgical indication (P>0.5). Mean cosmesis scale was 19.86±3.56 of 24 (scar rating: 8.31±1.80 of 10). Cosmesis scores for women and men were 20.9±3.2 and 19.4±3.7, <50 years and ≥50 years were 20.2±3.4 and 19.7±3.7, and for malignancy, donation, and benign conditions were 19.7±3.7, 20.5±3.2, and 20.3±3.5, P>0.4. Confidence before and after surgery was 8.53±2.00 and 8.67±1.88, P=0.199. Eight patients had declined confidence: 8/49 men and 0/25 women (P=0.045), 3/26 aged <50 years and 5/48 aged ≥50 years (P=0.882), and 7/51 malignancies and 1/14 donors (P=0.420).
Discussion
In our survey of 79 patients, the factors most important in choosing a surgical modality were success and complications (4.7 and 4.2). Pain and convalescence had moderate importance (3.4 and 3.7), while scars had less importance (2.2), which was more important in women, younger patients, and benign cases. Preference for LESS increased in those rating scars as important (49% vs 18%). Women (39% vs 28%), younger patients (36% vs 29%), and patients treated for benign conditions (56% vs 30% cancer, 21% donors) tended to prefer LESS more often.
Several reports suggest LESS is comparable to SL in terms of safety and efficacy. In 100 LESS cases, conversion to SL occurred in three cases and open conversion in four cases. 8 Intraoperative complications occurred in five (one bowel injury) while postoperative complications occurred in nine patients (one death, 1/17 grafts lost). In a randomized study of patients undergoing simple nephrectomy by LESS (14) or SL (13), median operative times were similar (117.5 min vs 114 min). 10 Blood loss was similar for LESS, 50.7 mL, and SL, 47.2 mL. In a multi-institutional review of 125 cases, LESS surgery was comparable to SL for extirpative procedures in complications (7.8%), but demonstrated a high rate of complications for reconstructive procedures (27.1%). 9
Despite this success, LESS is more difficult to perform. Comparing simulator performance of tasks on SL and LESS platforms by inexperienced, SL-experienced, and LESS-experienced surgeons, performance decreased in all groups on the LESS platform. 13 In the future, difficult procedures may be alleviated by the development of a robotic platform. 18 In our study, patients were most concerned with treatment success and complication. Thus, further investigations of safety and long-term follow-up of treatment success are needed for LESS.
Patients concerned with pain tend to prefer LESS, a preference supported by studies of pain and convalescence after LESS. In a comparison of LESS and SL nephrectomy, pain scores were significantly lower for LESS than SL, differing by 0.5 to 1 of 10 points. 10 Analgesic use and time to convalescence decreased for LESS (10.7 d vs 13.5 d, P=0.001). In donors, LESS decreased time to analgesic discontinuation (6d vs 20 d), return to work (18 d vs 46 d), and 100% recovery (29 d vs 83 d). 7 Median incision length was 4.1 cm for LESS (SL not reported), which may bias the results. In contrast, comparison of LESS and SL pyeloplasty showed no difference in hospital stay (77 h vs 74 h) or use of analgesics (34 vs 38 morphine equivalents). 11
In our series, patients concerned with scars more often preferred LESS. Canes and colleagues 7 matched 18 LESS with 17 SL, demonstrating that mean scar rating scores were significantly higher for LESS (9.7 vs 7.7, P=0.003). 7
While we report a slight preference for SL (39%) over LESS (30%), others report preference for LESS. In a study of 736 participants regarding preference for LESS, SL, or natural orifice translumenal endoscopic surgery (NOTES), LESS was preferred with a rank of 1.78/4 vs 1.98/4 for SL. 19 There were no sex differences. 19 In our series, women tended to prefer LESS, although this was not statistically significant. In addition, women were more concerned with cosmesis. In their survey, as in ours, age decreased preference for LESS with 57.6% of those <20 years preferring LESS vs 31.6% >60 years. 19 Median age in their study was <30 years, which increased preference for LESS. Similarly, 100 females in a surgery clinic preferred NOTES cholecystectomy (68%) to SL. 20 The choice was influenced by cosmesis (61%), hernia (90%), and pain (93%). 20 Cosmesis most strongly predicted preference for LESS in our series. Before surgery, patients may overemphasize pain from SL as a reason to choose LESS.
Finally, among 192 presurgical patients, 56% preferred NOTES cholecystectomy. 21 In deciding surgery, 98.4% were concerned with complications, 88.9% with pain, and 49.5% with cosmesis. They perceived more complications with open surgery and SL than NOTES. 21 Thus, before surgery, patients may have unrealistic expectations of new techniques.
Interestingly, we found that donors had a low concern for scars similar to malignancies, despite being younger. Furthermore, donors had the lowest preference for LESS. While ways to improve interest in donation should be encouraged, safety and successful transplantation should be maintained, because patients who present for donation are most concerned with these.
This study has limitations that we discuss below. First, we used postoperative patients, which may bias preferences toward SL. Preoperative patients, however, also have biases from inexperience. A second limitation is that median age (50 y) for our series is higher than others, underestimating preference for LESS. Thus, subgroup analysis by age was performed. Third, the number of patients was relatively low, particularly for benign cases and donors. Further study is needed to better define their preferences. Finally, the body image and cosmesis questionnaire did not differentiate treatment groups, which was muted by a floor effect (responses clustered at the top). The body image and cosmesis scales in other series distinguished differences in open and SL splenectomy and colectomy, 16,17 but not appendectomy or donor nephrectomy. 14,15
Conclusion
Patients who were treated with laparoscopy for urologic conditions were predominantly concerned with complications, success, recovery, and pain, and were less concerned with cosmesis. Female patients, younger patients, and patients who were treated for benign conditions had an increased concern for cosmesis and could be ideal patients for LESS. Overall, patients were very satisfied with their postoperative scars after traditional minimally invasive surgery with multiple ports.
Footnotes
Disclosure Statement
No competing financial interests exist.