
Abstract
Background and Purpose:
The complete removal of the stone is the ultimate goal in management, a result that might not be attained even after several sessions of percutaneus nephrolithotomy (PCNL) and/or extracorporeal shockwave lithotripsy (SWL) and/or retrograde intrarenal surgery (ureteroscopy). The objective of this study is to assess our technique of anatrophic nephrolithotomy, with decreased renal ischemia and reduced patient morbidity.
Patients and Methods:
From 2007 to 2010, we performed eight anatrophic laparoscopic nephrolithotomies in adult patients with staghorn renal calculus. The mean patient age was 49 years (range 35–62 y). The mean stone size was 53 mm (range 35–70 mm). All patients had complex renal calculi, with stones occupying more than 80% of the caliceal system. In all cases, a Double-J stent was placed before surgery. After clamping the hilum, the incision was made laterally and longitudinally through full thickness of cortex using a laparoscopic scalpel. A running cortical suture was performed with Hem-o-lok reinforcement. Renal function was assessed in three patients, using renography with technetium-99m-diethylenetriaminepentacetic acid (99mTc-DTPA), before and 3 months after the surgery.
Results:
Procedures for all patients were completed laparoscopically. The mean operative time was 142.5 minutes, and the mean warm ischemia time was 20.8 minutes. The estimated blood loss was 315 mL. The hospital stay average was 3.5 days. Only one patient had a complication—a vascular fistula with permanent postoperative hematuria. This patient subsequently underwent successful endovascular embolization. Residual stones were identified in 37% of cases (three patients) during follow-up imaging at 15 days. There were minimal changes on serum creatinine values.
Conclusions:
Laparoscopic surgery is feasible when anatrophic nephrolithotomy is indicated. This technique minimizes the barriers of an open flank incision, while achieving excellent stone-free rates. This minimally invasive technique should be considered for complex stones that would necessitate multiple renal access tracks and secondary procedures.
Introduction
The pioneers in the technique of open anatrophic nephrolitotomy were Boyce and Elkins, 2 who used anatomic and physiologic principles mixed with reconstructive techniques to performed this operation. With the development of laparoscopic and robot-assisted surgery in urology, there is the possibility to duplicate complex open surgical techniques, even complex procedures, such as extended pyelolithotomy and anatrophic nephrolithotomy. In fact, there have been a number of reports comparing laparoscopic nephrolithotomy with standard open techniques. 3,4
The goal of the laparoscopic approach is to ultimately improve the outcomes of open nephrolithotomy by eliminating the morbidity of the abdominal wall incision, reducing the warm ischemia time of renal injury, and improving stone-free rates.
The objective of this study is to assess our technique of anatrophic nephrolithotomy, with decreased renal ischemia and reduced patient morbidity.
Patients and Methods
From 2007 to 2010, we performed eight anatrophic laparoscopic nephrolithotomies in adult patients with staghorn renal calculi; all were performed by the same surgeon.
One patient had previous nephrolithotomy procedures in the same kidney, and two other patients had surgery several times on the contralateral kidney, for management of bilateral renal calculi.
The mean patient age was 49 years (range 35–62 y). The procedure was performed in four women and four men, and 66% were left kidney surgery. The average body mass index was 25.5 (range 22–31); the mean stone size was 53 mm (range 35–70 mm). All patients had complex renal calculi, with stones occupying more than 80% of the caliceal system (Table 1).
BMI=body mass index; SWL=shockwave lithotripsy; PCNL=percutaneous nephrolithotomy; UTI=urinary tract infection.
Before surgery, patients had a complete radiologic evaluation, including abdominal CT with three-dimensional reconstruction, assessing stone size (largest diameter), degree of caliceal extension, and hydronephrosis. All of the patients were admitted on the day of the surgery; they received adequate bowel preparation and intravenous (IV) antibiotics, a complete blood cell count, and urine analysis and culture during the same period. Renal function was assessed in three patients, using renography with technetium-99m-diethylenetriaminepentaacetic acid (99mTc-DTPA) before and 3 months after the procedure.
Preoperative preparation
Complete knowledge of the collecting system anatomy is essential, with either IV urography, retrograde pyelography, or CT imaging. Many patients who need these procedures have struvite calculi, so it is important to institute antibiotic coverage from preoperative evaluation; cultures taken from the stones (or the collecting system) are often discordant with the findings in voided urine cultures. The antibiotic should be broad spectrum and include management for urease-producing organisms. 5
Surgical technique
After general anesthesia, a Double-J stent is placed; in all cases, the patient must be repositioned to the side lying opposite the kidney to be treated.
In this laparoscopic technique, we use five trocars. The first trocar (10 mm) placed in the pararectal line, 3 cm above the umbilicus, is for the laparoscope. The other four trocars are placed under direct vision. One trocar (5 mm) is placed to the left side, 8 cm below the laparoscopic trocar. A second trocar (10 mm) is placed 8 cm to the right of the laparoscope. These three trocars form a triangle. An additional trocar of 10 mm is placed on the right side and used for renal retraction. In addition, the surgeon can use either of the right trocars to find the correct angle to incise the renal parenchima. The last 10-mm trocar is placed in the umbilicus for the Satinsky or bulldog clamp. If one is performing the procedure on the right kidney, an additional 5-mm trocar is placed in the epigastric area to retract the liver (Fig. 1).

Placement of ports.
After the incising on the white line of Toldt, superior retraction of the liver, and medial mobilization of the colon and duodenum (right), the renal pedicle is exposed and prepared for hilar clamping.
The perinephric fat is carefully removed from a segment of the anterior and posterior surface of the kidney to uncover the renal capsule, exposing clearly both faces of the kidney and the Brödel line. When clamping the hilum, we prefer to occlude only the artery (Fig. 2). Previous studies have demonstrated that selective arterial clamping is sufficient to minimize or avoid bleeding, because the vein is under control by CO2 insufflation compression.

Clamping the hilum; occlude only the artery.
A longitudinal nephrotomy is performed 1 or 2 cm behind the junction of the posterior and anterior kidney surfaces on the Brödel white line, lying in a specific area that is functionally an avascular plane. 6
In the first two patients, the incision was performed at the junction of the posterior and anterior kidney surface to seek complete and easier access to the collecting system. In the following six patients, the incision was performed along the Brödel line with good results, less bleeding, and achieving full exposure of the collecting system.
We have been using a homemade cold scalpel that is introduced under direct vision to protect the trocar by avoiding damage to the valve. The scalpel consists of a purpose-built detachable blade normally used in open surgery (number 11) assembled to a 5-mm large handle and 30-cm long handle (Fig. 3). The long, smooth incision makes the resection more expeditious while reducing the warm ischemia time. It has been reported that the severity of renal ischemic injury is directly proportional to the duration of ischemia time and that warm ischemia time should not exceed 30 minutes if the integrity of renal function is to be maintained. 4 –6
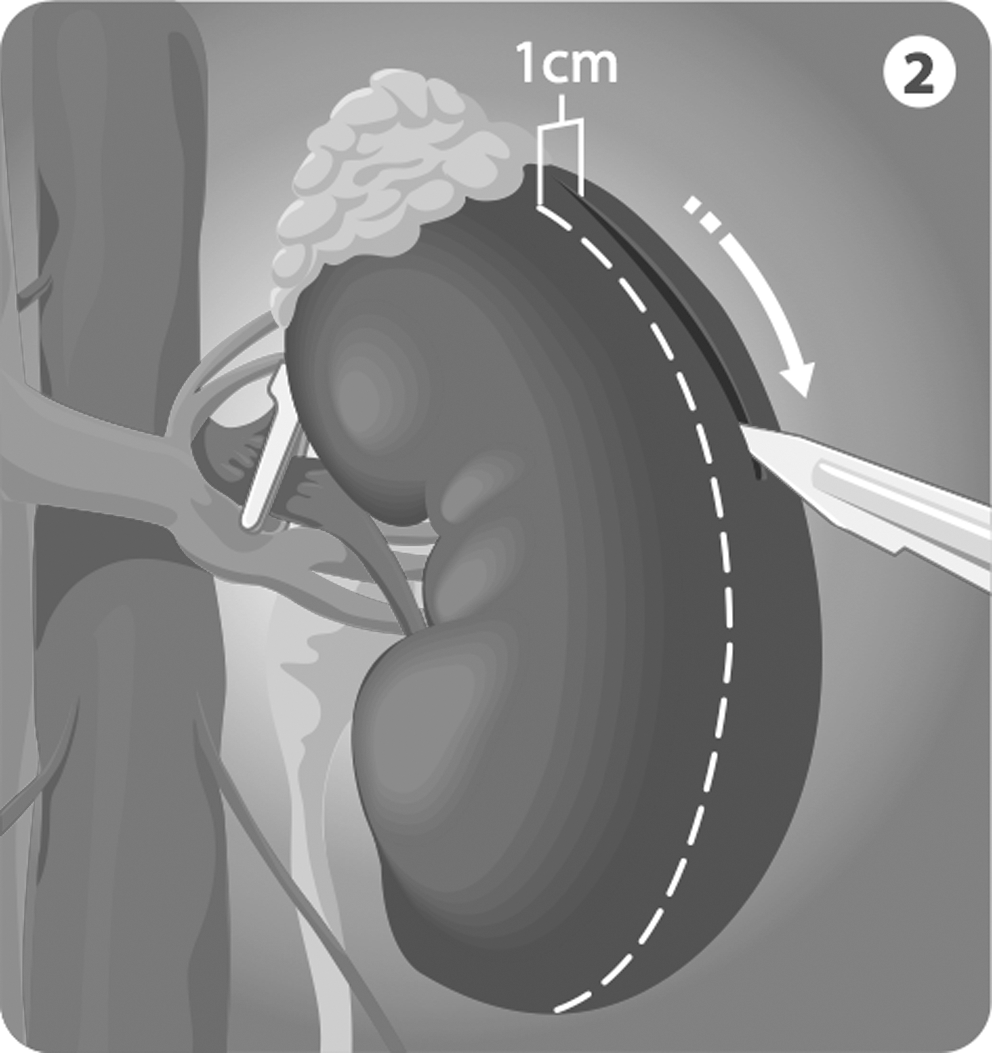
Long and smooth incision with cold scalpel along the Brodel's line.
IV mannitol (12.5 to 25 g) can be given to the patient before clamping the renal artery to reduce cellular edema and to attenuate reperfusion injury by serving as a free radical scavenger. 7
The collecting system is opened to expose the stone. A right angle clamp and Allis clamp can be used to free up the stone, because our intent is to remove the staghorn calculi in one piece. Therefore, any stenotic infundibulae are opened before the stone is extracted to prevent fracture of the calculus. Shredding of the renal parenchyma is limited by using a gentle, deliberate, intrarenal exploratory technique. The surgeon must be familiar with the calculus configuration during the stone removal to assess where additional stone fragments may be located and removed before closing the parenchyma (Fig. 4).
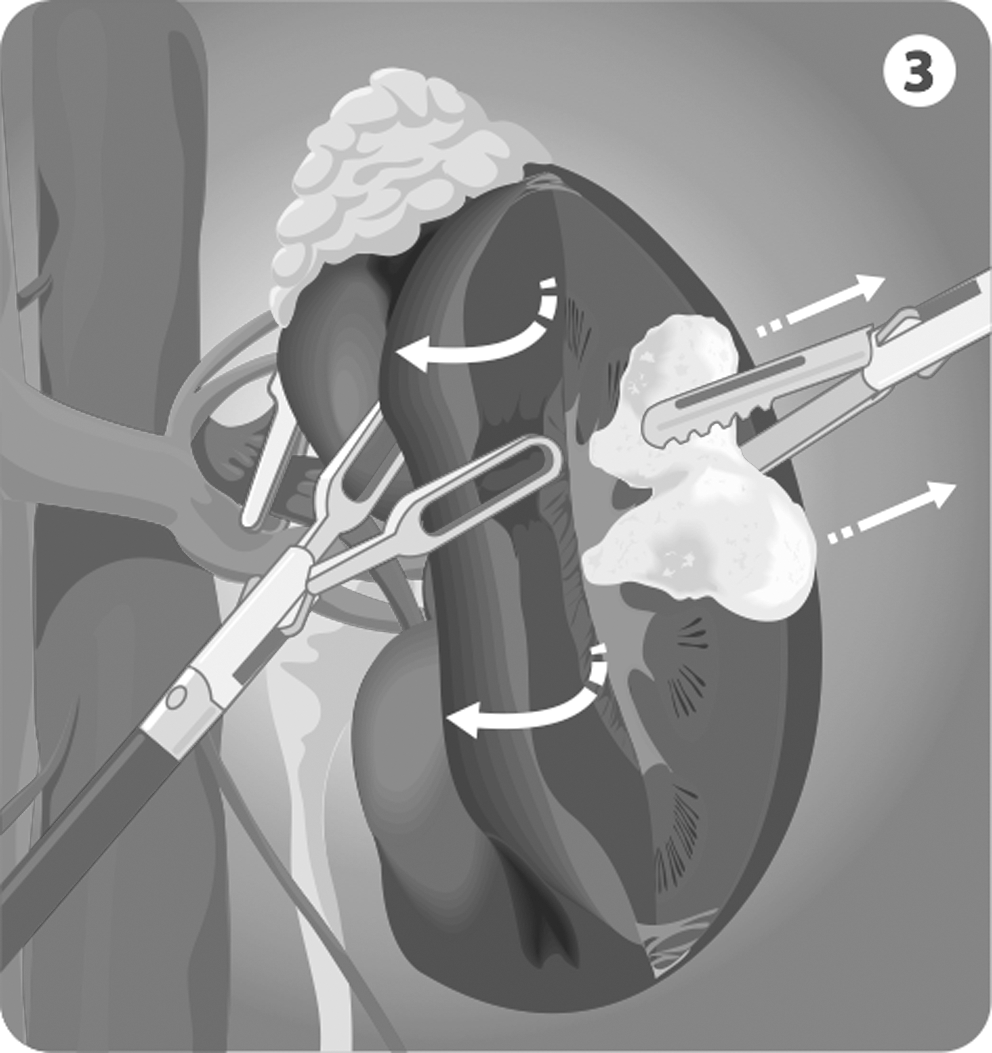
Stone removal; assess if additional stone fragments may be located and removed before closing the parenchyma with 30 degree lens.
After stone removal, the collecting system is inspected with a 30 degree lens. Once stone clearance has been confirmed endoscopically, arterial bleeders, and visibly transected vessels in the opened parenchyma are oversewn with polyglactin 2-0. A running cortical suture is also performed with Hem-o-lok reinforcement (Fig. 5). After parenchymal closure, the vascular clamp is opened to assess for any residual bleeding (Fig. 6). If bleeding persists, reinforcing absorbable sutures can be placed at the site of hemorrhage and bolstered with Surgicel or Gelfoam. A Jackson-Pratt drain is then placed and brought out through.
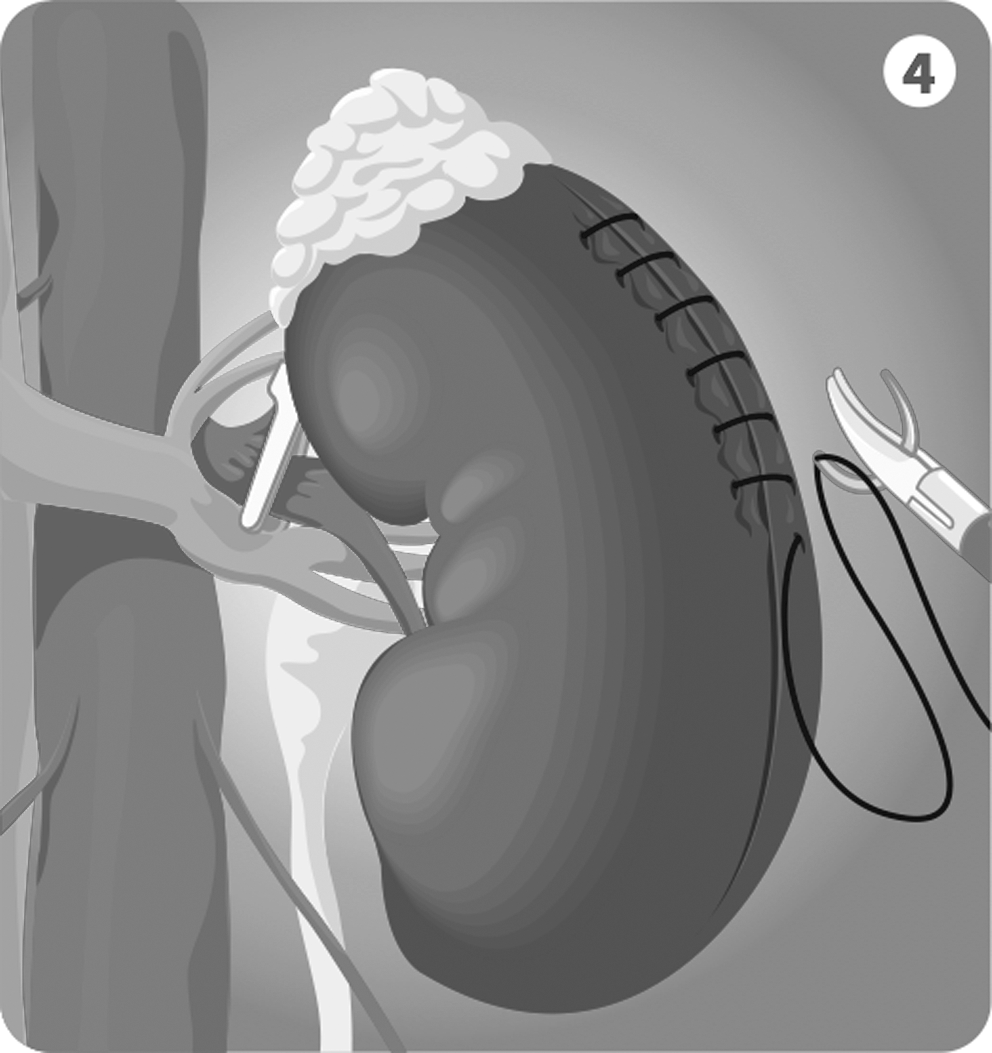
Closing the parenchyma; visibly transected vessels in the opened parenchyma are oversewn with polyglactin 2–0. A running cortical suture is also performed with Hem-o-lok reinforcement.

After parenchymal closure, the vascular clamp is opened.
It is important to compare the extracted lithiasic piece with the previous CT scan image to see if is complete.
Results
Procedures for all patients were completed laparoscopically; no procedure required conversion to an open technique. The mean operative time was 142.5 minutes (range 120–180 min), and the mean warm ischemia time was 20.8 minutes (range 13-30 min).
The estimated blood loss was 315 mL (range 100–600 mL), and three (37%) patients received transfusions. The hospital stay average was 3.5 days (range 3–5 d).
Only one patient had a complication—a vascular fistula with permanent postoperative hematuria. This patient subsequently underwent successful endovascular embolization. Residual stones were identified in 37% of cases (three patients) during follow-up imaging at 15 days. These residual calculi were not up to 1 cm in diameter (Table 2). There were minimal changes in serum creatinine values.
EBL=estimated blood loss.
Renal function was assessed in three patients before and 3 months after surgery, using renography with 99mTc-DTPA. Renal function decreased by a factor of 4%, 12%, and 4% on the operated kidney (Table 3).
GFR=glomerular filtration rate.
Discussion
Despite further developments in percutaneous renal surgery, the anatrophic nephrolitotomy has clear indications. The AUA Nephrolithiasis Guidelines Panel stated in their 2004 guideline for staghorn calculi that anatrophic nephrolithotomy should be considered when complete stone removal could not be completed in a reasonable number of minimally invasive procedures or if the kidney had unusually complex anatomy. 8 For example, studies have suggested that with complex renal calculi, where the total stone area exceeds 2.500 mm3, the stone-free rate with PCNL is only 50%. 7 –9 Stone size and collecting system anatomy have less impact on the outcomes during anatrophic nephrolithotomy. 10
Contraindications to laparoscopic anatrophic nephrolithotomy are patients with coagulopathy or active urinary tract infection. One should also assess the patient's renal function, because kidneys with <10% function should probably be removed.
Postoperative complications include acute tubular necrosis, especially in those patients with renal insufficiency or solitary kidneys and postoperative renal bleeding; the medical literature reports a 6% transfusion rate in those patients undergoing anatrophic nephrolithotomy. 7 The risk of acute tubular necrosis can be minimized with the use of IV dopamine in high-risk patients after the kidney has been reperfused. Renal function usually returns to baseline, and standard medical management is often sufficient without dialysis. 7
It has been reported that the severity of renal ischemic injury is directly proportional to the duration of ischemia time, and that warm ischemia time should not exeed 30 minutes if the integrity of renal function is to be maintained. 4 –6
In the present study, we assessed the feasibility of laparoscopic anatrophic nephrolitotomy for the management of complex renal calculi. We did not use a cooling system, and the mean warm ischemia time was 20 minutes, which is considered within the acceptable range. 11,12
Stubbs and Resnick 13 reported that serum creatinine levels did not significantly increase in patients with a solitary kidney who were undergoing anatrophic nephrolithotomy. Thomas and colleagues 14 found a decrease of renal plasma flow in kidney surgery, as determined by scintillation techniques.
Morey and coworkers 15 reported an average decrease of 4% in postoperative renal function, measured by nuclear renography, after open nephrolitholtomy. They determined, however, that 20% of the patients had a 20% improvement in renal function in the treated kidney over time. Stage and Lewis 16 reported both a decrease and increase in postoperative renal function, measured with iodine 131-hippuran and DTPA scintigraphy. 16 These studies suggest that renal function can decrease after anatrophic nephrolithotomy, but these changes are not clinically significant. The postoperative functional improvement may be important in some cases, however, especially in those kidneys that are severely infected or obstructed.
Early experience in an animal model suggested that laparoscopic anatrophic nephrolithotomy was a feasible technique. Synthetic calculi were place din 10 animals, the renal artery was controlled, in situ ice slush cooling was initiated, and after a parenchymal incision was made to remove the stones, the collecting system was repaired. 4 Simforoosh and colleagues 17 published the first human experience in 2007, reporting on five patients. In this series, only the renal artery was clamped, with the warm ischemia time ranging between 29 and 35 minutes. Laparoscopic scissors were used to open the kidney, and residual stones were found in two patients.
One of the concerns raised by the 2004 AUA Guidelines to limit the use of open nephrolithotomy is that patients are subjected to long incisions that may promote hernias or eventration through the abdominal muscles. The benefits of laparoscopic procedures, in a similar approach, have been demonstrated after laparoscopic nephrectomy when this procedure was compared with open nephrectomy. 18
The development of laparoscopic anatrophic nephrolithotomy follows the evolution of robotic pyeloplasty, which now achieves similar success rates as those of open pyeloplasty without the morbidity of the open approach. Now, anatrophic nephrolithotomy can successfully remove stones in a fashion similar to that of open nephrolithotomy, but with a minimally invasive approach, with reduced incisional pain and avoiding the possibility of complications, such as incisional hernias (Table 4).
Our intention was to duplicate the results of open anatrophic nephrolithotomy with regard to stone-free rates and renal injury. Yet our stone-free results did not approach the outcomes of open surgery, probably because of the use of imaging with small radiographic films used to identify residual stones during open anatropic nephrolithotomy. 19,20 Therefore, we are currently exploring alternative imaging technologies, such as intraoperative ultrasonography and/or ways to increase our exploration time of the collecting system, such as controlled hypotension or hypothermia. 11,12
Yet the stone-free rate of our laparoscopic anatrophic nephrolithotomy appears better than PCNL for the management of large volume stones (>2.500 mm3), (37% vs 50%). 21 Moreover, patients undergoing complex PCNL have demonstrated an 8% decrease in renal function (glomerular filtration rate [GFR]). In the current study, the patients who were treated with laparoscopic anatrophic nephrolithotomy demonstrated a 6.6% decrease in GFR (range 4–12) (Table 3). 22
Conclusions
Anatrophic nephrolithotomy historically has produced high stone-free rates for the removal of complex renal calculi. The primary drawback of this approach was the morbidity of the flank incision. Laparoscopic techniques minimize the barriers of an open flank incision, while achieving excellent stone-free rates. This minimally invasive technique should be considered for complex stones that would necessitate multiple renal access tracks and secondary procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.