
Abstract
Purpose:
The goal of this study is to evaluate the role of laparoscopic curricula and simulation technology in urology residency training from the perspectives of residents over a 2-year period.
Materials and Methods:
An anonymous survey was given to urology residents attending the American Urological Association Basic Sciences Course in 2008 and 2009. We evaluated laparoscopic simulator use within a curriculum and use of simulators outside of a curriculum. Face and content validity of simulators were analyzed on a 5-point Likert scale questionnaire. Responses were compared using the unpaired Student t test and chi-square with P<0.05 considered significant.
Results:
There were 114 surveys (81.4% response rate) and 76 surveys (43% response rate) evaluated from 2008 and 2009, respectively. Access to a surgical simulator increased from 74.6% to 78%. The percentage of programs with a laparoscopic curriculum expanded from 16.9% to 44%. In 2009, simulators were used more frequently by residents in programs with curricula compared with residents without curricula (P=0.03). In 2008, 48% of residents and in 2009 72% of residents reported using simulators as “never” or “once or twice a year.” Of residents, 93% stated that urology programs should use laparoscopic curricula and 82% think simulators should be involved in the curricula. One third of residents agreed that simulators are helpful for skill acquisition, and 80% described their current laparoscopic curriculum as inadequate.
Conclusions:
The number of urology programs that have invested in simulators continues to expand. Despite access to laparoscopic simulators, residents rarely use them. Residents in programs with laparoscopic curricula report using surgical simulators more often than residents without curricula. Laparoscopic curricula are important, and the incorporation of simulators enhances surgical education.
Introduction
Robotic and laparoscopic simulators are increasingly available to develop technical skills that decrease the learning curve for new procedures, improve operative efficiency, and decrease error rate. 3 –5 In addition, simulator acquired skills are transferable to the operating room. 6,7 Although the use of simulation technology is gaining a foothold in medicine, such technology is well established in other disciplines, such as the aerospace industry and training military personnel. In 2008, the Residency Review Committee in surgery decreed that the resources for all training programs within the United States “should include simulation and skills laboratories.” 8 The role of simulation in urology residency remains largely unknown and the perspectives of urology residents are unheard. The goal of this study is to evaluate the role of simulators in urology residency training from the perspectives of residents. In addition, we assessed the impact of laparoscopic curricula on simulator use by residents.
Materials and Methods
After Institutional Review Board approval, an anonymous survey of simulation education opportunities in urology residency training was developed (Appendix A and B). In June 2008 and 2009, the survey was distributed to urology residents attending the American Urological Association (AUA) Basic Sciences Conference held annually in Charlottesville, VA, at the University of Virginia. All respondents were queried concerning demographic data of their programs, including AUA section and program name. Each year, the participants of the AUA Basic Sciences course encompass a new group of junior residents transitioning into their first year of urology training. Therefore, we do not expect any duplicate responses between 2008 and 2009.
The first part of the survey consisted of questions about laparoscopic and robotic experience. All residents were questioned about the presence of a dedicated laparoscopic skills laboratory and perceived value of a laparoscopic curriculum. Those residents responding “yes” regarding a laparoscopic skills laboratory were specifically asked about types of trainers, incorporation of simulators into a laparoscopic curriculum, and use of trainers outside of a curriculum.
The second part of the survey included seven statements to which residents expressed their agreement on a 7-point Likert scale (1-strongly agree, 4-neutral, 7-strongly disagree) regarding the impact of surgical simulators on their urologic training. Responses were compared using the unpaired Student t test and chi-square test with P<0.05 considered significant. All statistical analyses were conducted using STATA 11.0 (StatCorp, College Station, TX).
Results
A total of 140 surveys were returned by residents in 2008 and 76 surveys in 2009 (Table 1). The overall response rates were 81% and 43% in 2008 and 2009, respectively. All sections of the AUA were represented in both years.
AUA=American Urological Association.
The majority of urology resident training programs have invested in surgical simulators. In 2008, 75% of residents reported they had access to surgical simulators (Table 1). In the span of 1 year, the percentage of residents who reported access to surgical simulators in their training programs was 78%, (P=0.81). Only 17% of residents reported that their residency training programs had incorporated a simulation-based laparoscopic curriculum. In 2009, 44% of residents reported simulation-based laparoscopic curricula in their residency training programs, which represents a significant increase (P=0.02).
Numerous different types of surgical simulators are used in urology programs in the United States (Fig. 1). In both years, the most popular surgical simulator used in urology residency programs was the laparoscopic box trainer (Lap Box), which was identified by 60% and 65% of residents in 2008 and 2009, respectively.
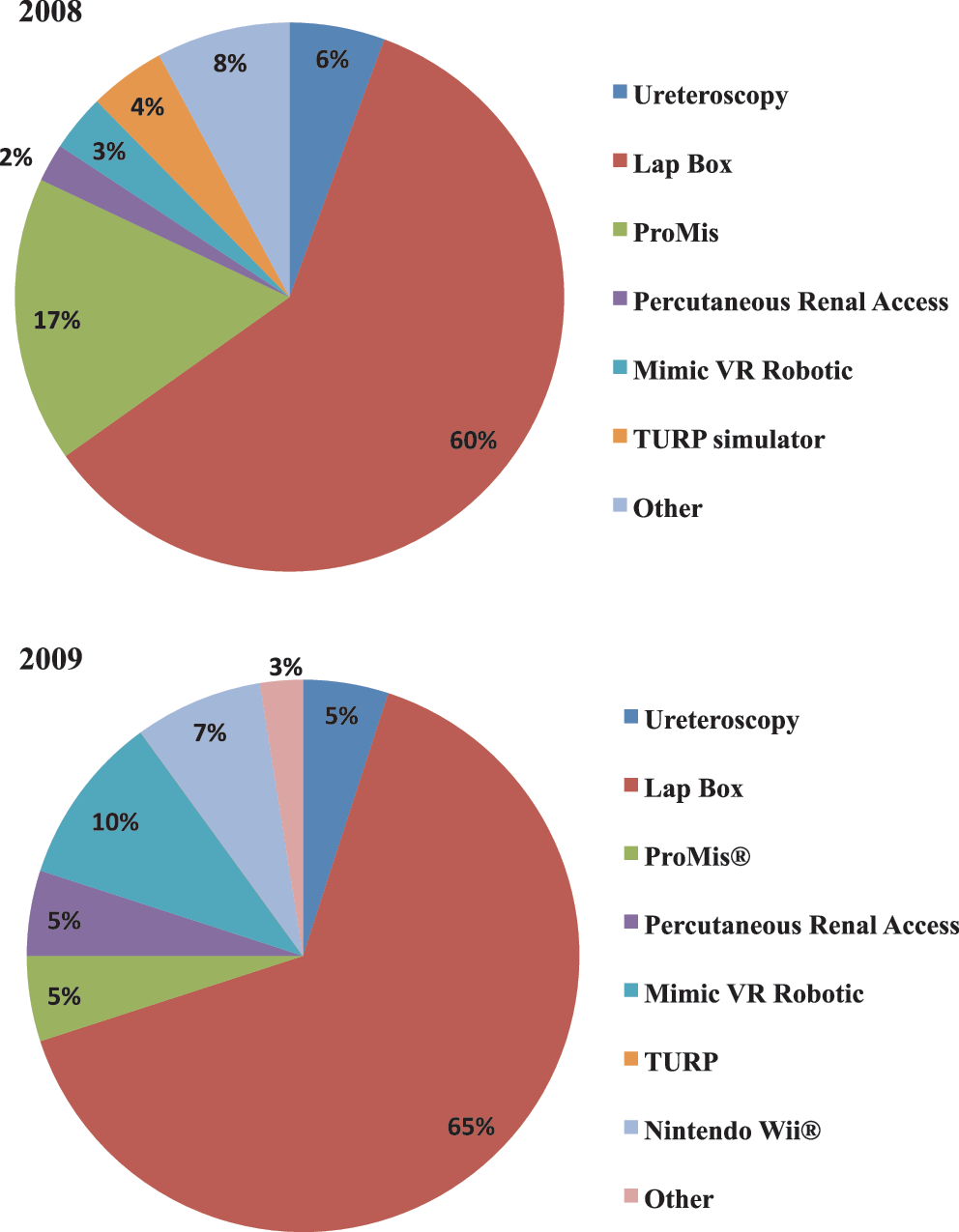
Types of surgical simulators used by residents in 2008 and 2009.
Participants were asked how often they use surgical simulators (Fig. 2). In 2009, the questionnaire was changed to distinguish simulator use outside of a curriculum. In 2008, approximately 30% of residents reported using surgical simulators “never.” Only 7% of residents reported using surgical simulators consistently “once a week.” In 2009, 24% of residents reported using surgical simulators “never” and 2% described using them “once a week.”
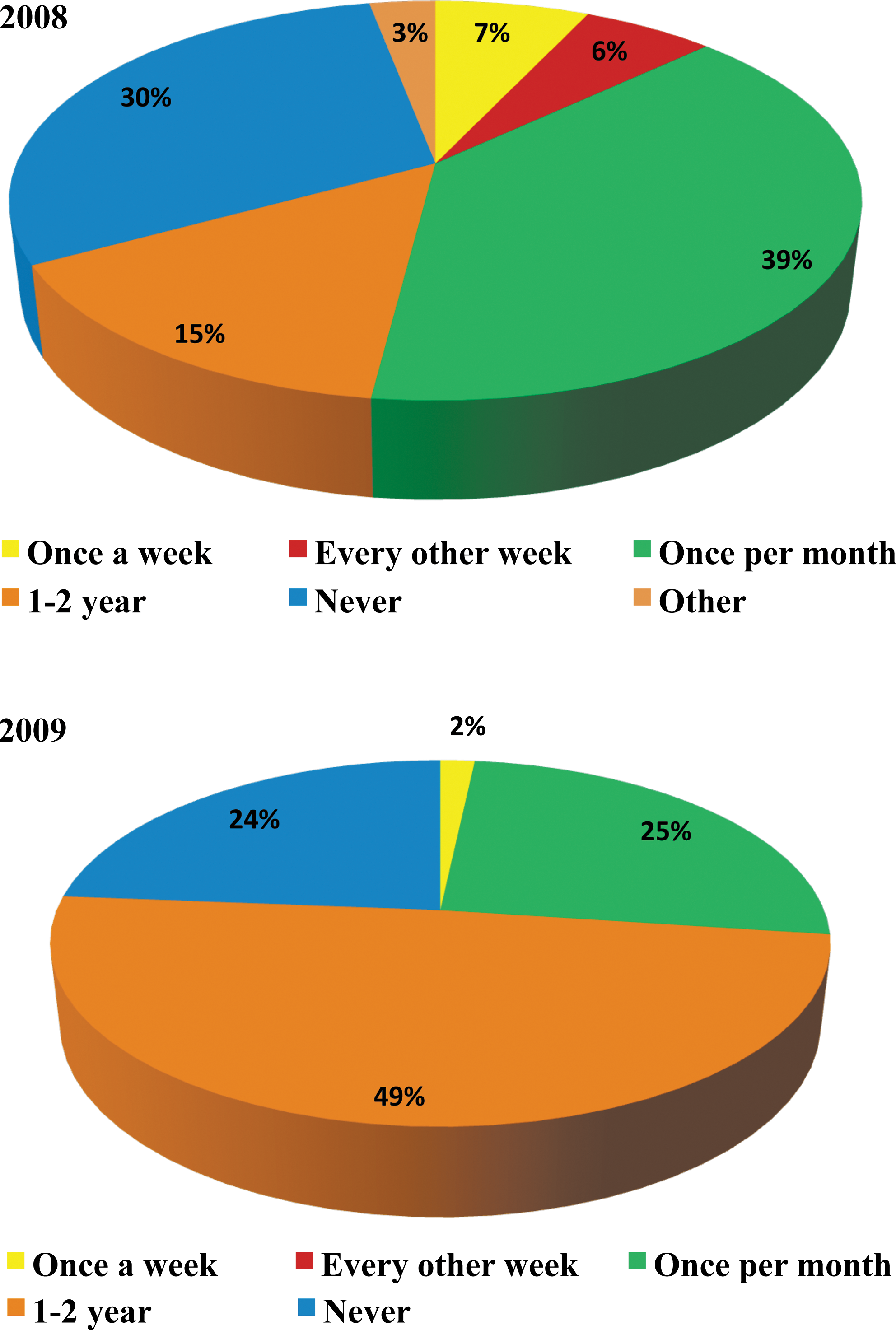
Reported use of surgical simulators by residents in 2008 and 2009.
We compared the use of surgical simulators by residents in programs stratified by the incorporation of a simulation-based laparoscopic curriculum (Fig. 3). In 2008, there was no statistical difference in the frequency of surgical simulators used by residents exposed to a laparoscopic curriculum. In 2009, the questionnaire was revised to separate the reported use of simulators outside of the requirements of laparoscopic curricula. Subsequently, residents in programs with incorporated simulator-based laparoscopic curricula used surgical simulators more often outside of the requirements of their curriculum than residents without a curriculum (P=0.03).
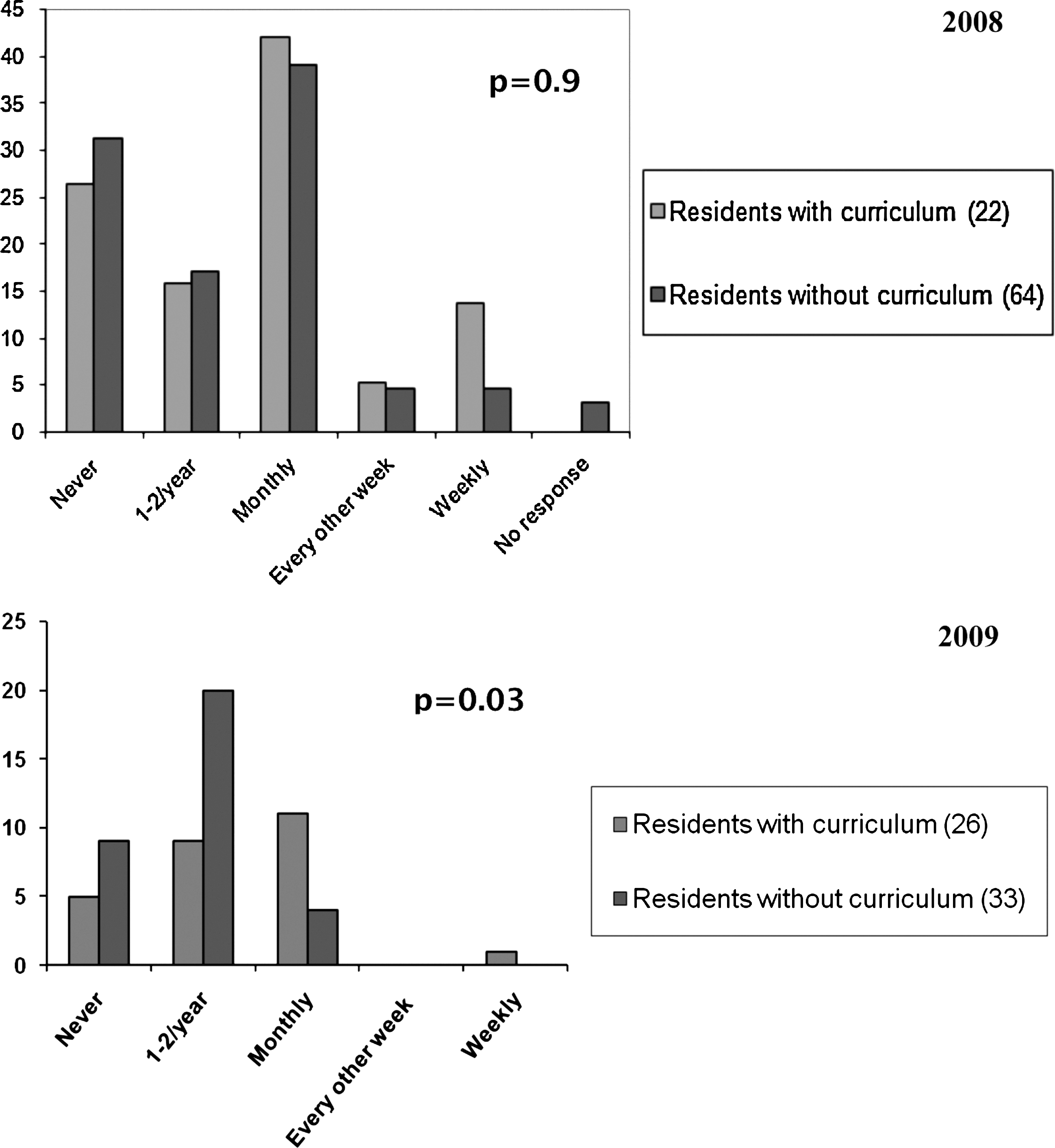
Impact of simulation-based laparoscopic curricula on reported use of surgical simulation by residents in 2008 and 2009.
We qualitatively assessed the current role of surgical simulators in urology residency training programs and structure of laparoscopic curricula from the perspective of residents. Ninety-three percent of residents reported that urology programs should incorporate laparoscopic curricula, and 82% stated that surgical simulators should be involved in curricula (Table 2). Fifty-three percent of residents agreed that the current curriculum at their institution for laparoscopic skills training is not adequate (Fig. 4). In addition, 48% and 49% of residents reported that working with surgical simulators improves intraoperative skills and is useful for learning basic tasks, respectively.

Qualitative assessment of simulation-based laparoscopic curricula in 2009.
Discussion
Modern surgical education requires the development of supplemental approaches to teach surgical skills outside of the operating room. A survey of 162 general surgery program directors found that 88% of responders considered skill laboratories effective in improving operative room performance, and only 55% of those surveyed provided this resource to their residents. 9 Similarly, a questionnaire of urology program directors reported a 68% prevalence of simulation education centers. The overall response rate, however, was low at 35%. 10 This study is the first to examine the perspectives of urology residents on surgical simulators and laparoscopic curricula in urology training programs.
The majority of urology programs have invested in surgical simulators. In some cases, these surgical simulators are very expensive. Approximately 20% of the surgical simulators represent high-fidelity platforms that involve advanced computer hardware and software. Despite access to surgical simulators, the majority of residents do not use them. The reasons are numerous and may include: Decreased time, work-hour restrictions, lack of motivation or incentive, and lack of evidence supporting the use of simulators and technical improvement in the operating room. These data may confirm the suspicions of urology program directors who observe residents in their programs, but the magnitude of this paradox is alarming. The results are more provocative given that all of the residents surveyed at the AUA Basic Sciences course are at the beginning of their training and represent a population that presumably should have the most time and motivation to use surgical simulators. The issue becomes more complex when we consider that the majority of program directors and residents believe surgical simulators are important to urology education.
We examined the underlying cause for these paradoxic results by asking residents to assess the structure of laparoscopic curricula in their institutions. In our experience, a laparoscopic curriculum that incorporates surgical simulators was a critical initial step to establish an effective program to teach surgical skills. Surgical simulators are tools of little educational value without the foundation of a curriculum that provides real-life context to motivate and teach residents surgical skills. The data suggest that surgical simulators are used more consistently by residents in programs that have incorporated simulators within laparoscopic curricula. These results highlight the importance of guidance and mentorship in surgical education. Specifically, a surgical curriculum may enable residents dedicated time away from clinical duties to focus on improving surgical skills. Moreover, competitive contests in surgical tasks between residents will provide incentive to actively participate in a curriculum. Finally, surgical educators can observe residents and provide constructive feedback outside of the stressful and time-sensitive environment of the operating room.
Several limitations of our analysis should be noted. Self-reported questionnaire data may introduce misclassification because of recall bias or selection bias. It may be presumed that residents interested in surgical simulator education or access to simulators would preferentially respond to survey questions regarding surgical education. Residents in programs without simulators, however, may also be interested in answering surgical education survey questions to improve the curriculum at their institution, which may explain the variability in our results.
A strength of this study is the large population surveyed. All of the participants were urology residents and represented all sections of the AUA. The residents were early in their training and therefore represent an ideal target to focus educational resources. In addition, this represents a homogeneous group because the majority of residents do not have any experience with laparoscopic urologic procedures.
From the perspective of residents, surgical simulators and laparoscopic curricula are important and enhance surgical education. Multiple studies have validated individual surgical simulators, but the next frontier in surgical education is to validate curricula that incorporate various surgical simulators. Academic leaders in urologic education have initiated the process of creating a core curriculum and laparoscopic handbook. 11 Further advancement may require a partnership between urology and other surgical specialties to enable an appropriate allocation of resources to create and validate laparoscopic curricula that can be shared by urology, gynecology, and general surgery services. Importantly, we envision that a laparoscopic curriculum should be a part of a broader surgical skills curriculum that encompasses open and endourologic education. Despite the emergence of high-fidelity surgical trainers for laparoscopy, the development of advanced surgical trainers for open surgery remains essential, because the obstacles to teaching laparoscopy in the operating room face open surgical education, as well.
We sought to describe the role of laparoscopic curricula and simulation training in urology training from the perspective of residents by using survey data. In the future we intend to administer the survey every 5 years and accumulate longitudinal data to evaluate the impact of surgical simulators on resident education.
Conclusions
In the era of a rapidly changing health care environment and surgical technologic innovation, the evolution of surgical education requires the development of a robust surgical skills curriculum incorporating surgical simulators. The majority of urology residency programs have invested in surgical simulators. Concurrently, more residency programs have adopted laparoscopic curricula. Despite access to surgical simulators, however, residents in programs without an incorporated laparoscopic curriculum do not use them. From the perspective of residents, the incorporation of surgical simulators in laparoscopic curricula is important and enhances surgical education.
Footnotes
Acknowledgment
Funding: University of Virginia Young Scientist Award given to Dr. Ehdaie.
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
Appendix A
Appendix B
Part II