
Abstract
Laparoscopic retroperitoneal lymph node dissection (RPLND) has been shown to be safe and effective in appropriately selected pediatric and adolescent patients with paratesticular rhabdomyosarcoma (RMS) and testicular germ-cell tumors (T-GCT). While the use of robot-assisted laparoscopy has expanded rapidly in many areas, there are very limited reports of its use with RPLND. We present two cases of adolescents who were treated using robot-assisted laparoscopic RPLND (R-RPLND)—one with paratesticular RMS (PT-RMS) and one with testicular GCT (T-GCT)—with good outcomes and low morbidity.
Introduction
Case Reports
Case 1
A 15-year-old male presented to the emergency department complaining of a right intrascrotal mass first noted 3 days before. Serum tumor markers were within normal limits, and ultrasonography noted a paratesticular mass. The patient underwent radical orchiectomy, and the pathology report demonstrated a 3.1-cm embryonal PT-RMS, negative margins, and no lymphovascular invasion (LVI). The postsurgical COG stage was stage I (T1aN0M0) and COG/IRS group Ia. Because of his age, he was offered RPLND and underwent a right ipsilateral, nerve-sparing R-RPLND.
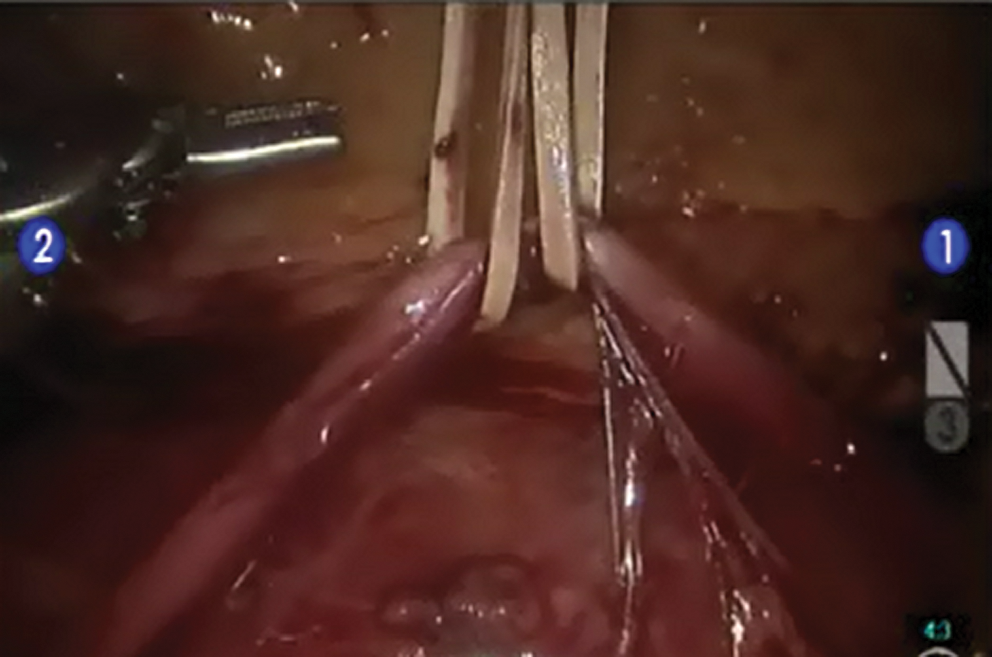
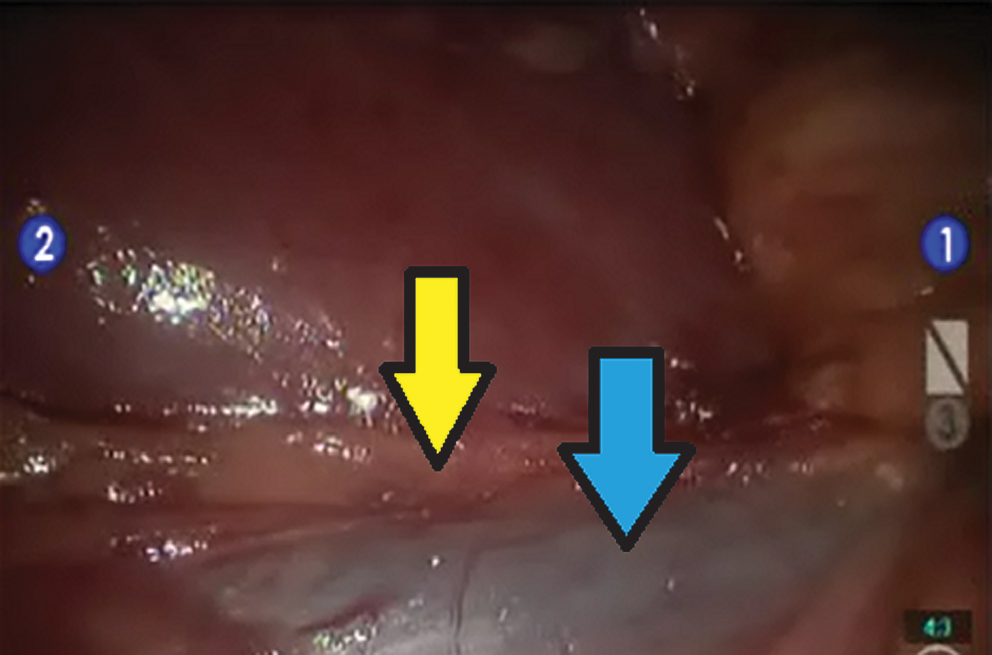
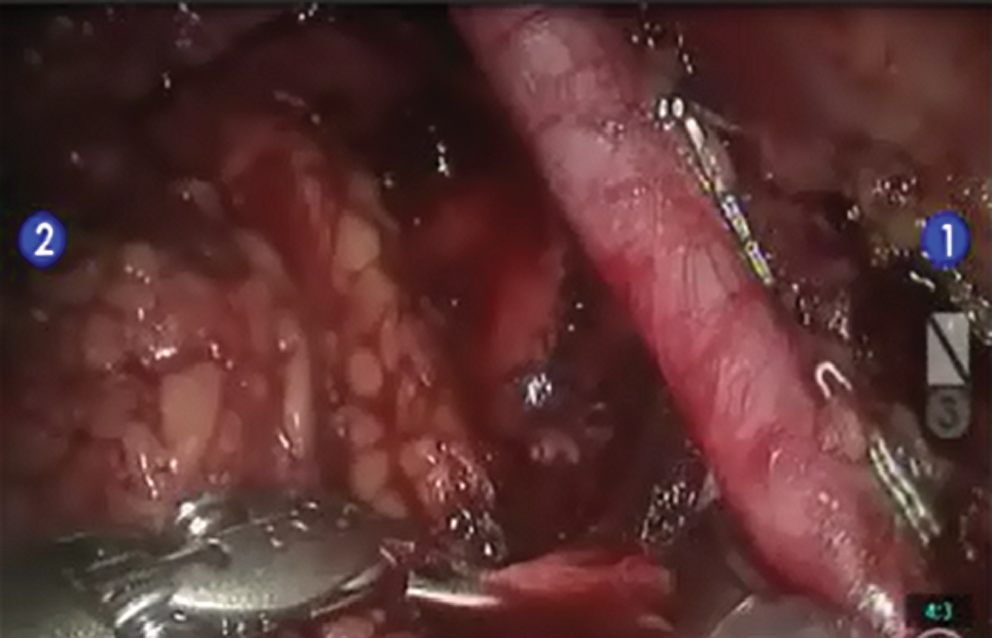
The patient had a favorable body habitus (height 162 cm, weight 62.5 kg, and body mass index [BMI] 24.7), which helped facilitate access and surgery. In a flank position, one 12-mm periumbilical camera port, two 8-mm robotic ports (1 midline below the xiphoid, 1 midline above the pubis), and two 5-mm assistant ports were placed (right upper and lower quadrants [RLQ]) (Fig. 1). First, the remnant right spermatic cord was dissected out and taken down to the point of the previous orchiectomy (Fig. 2). The colon was then mobilized medially, incising the white line of Toldt from the cecum inferiorly to the hepatic flexure superiorly (Fig. 3). Next, the duodenum was “kocherized” to reveal the renal vessels, the inferior vena cava (IVC), and ureter (Fig. 4). Dissecting out the ureter allowed for proper retraction to avoid ureteral injury (Fig. 5). The precaval tissue was then split to begin the dissection of the pericaval lymph nodes (LNs) (Fig. 6). This dissection then allowed for visualization of the common iliac artery and aorta (Figs. 7 and 8). Ultimately, the common iliac, pericaval, and interaortocaval LNs were taken.
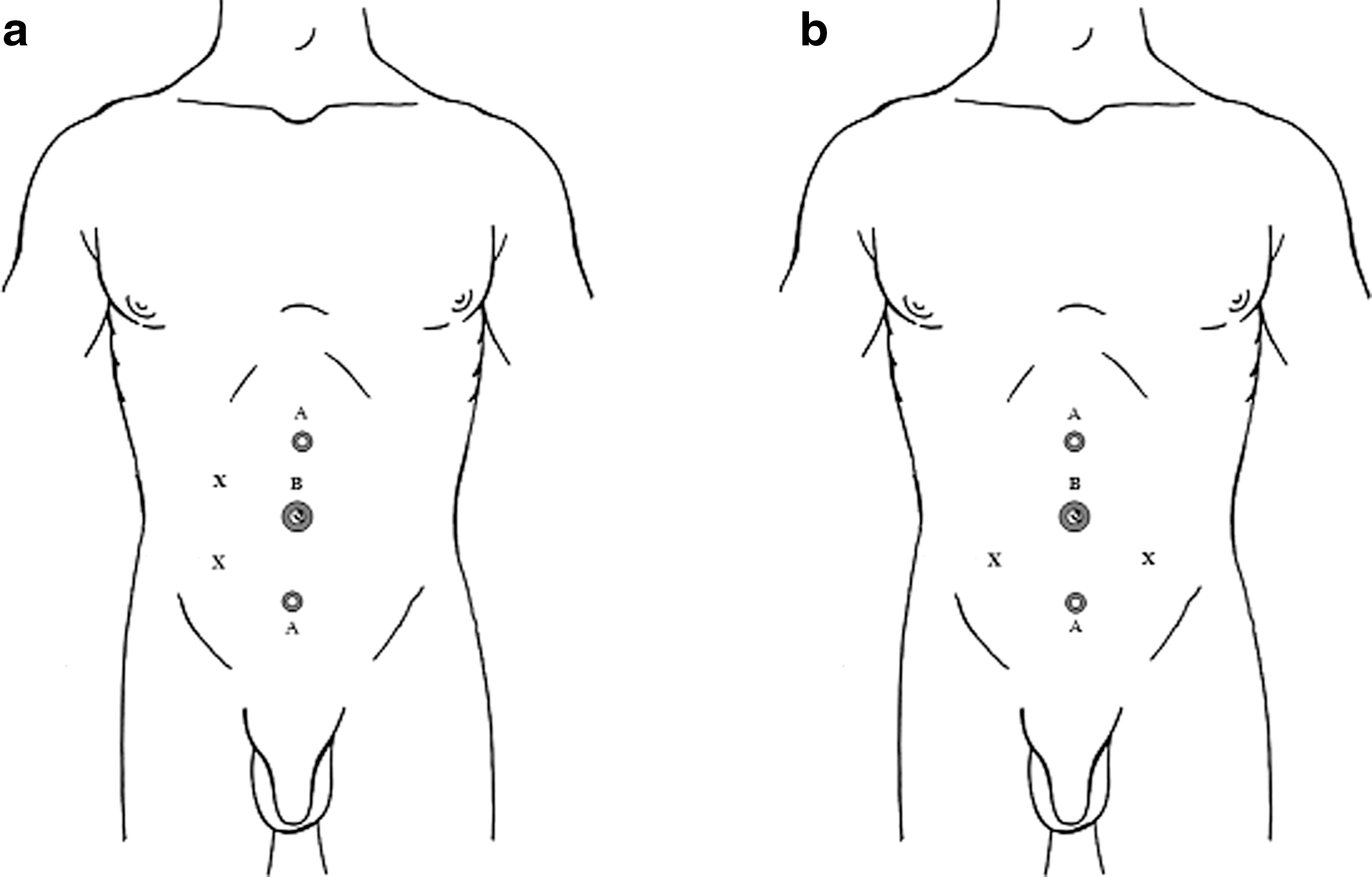
Placements of laparoscopic ports
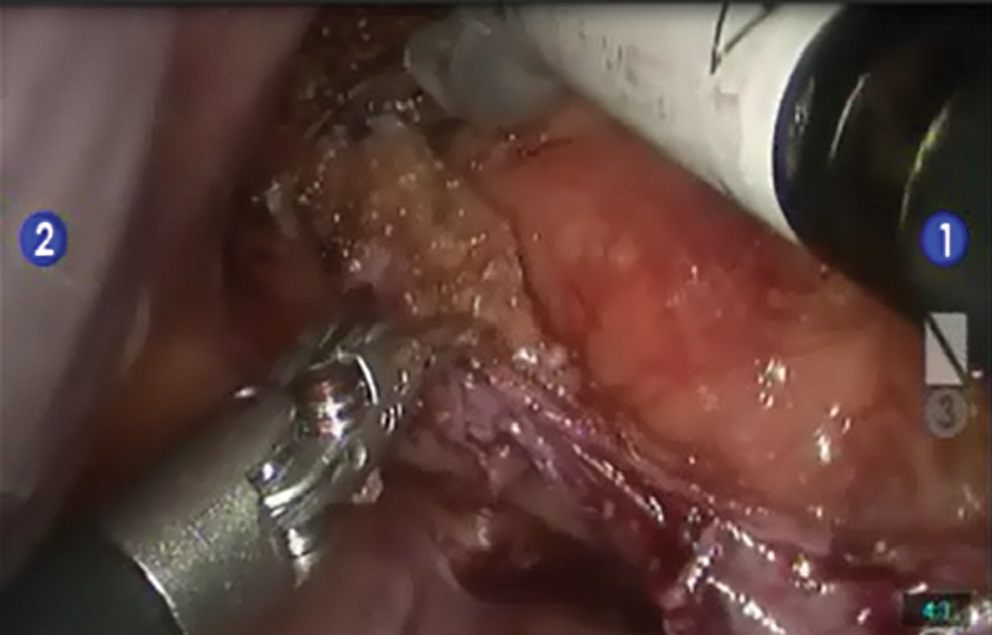
Dissected right spermatic cord, taken down to the level where it had been transected at the previous right radical inguinal orchiectomy.

Medial mobilization of the right colon by incising the white line of Toldt past the hepatic flexure to allow for maximal exposure.
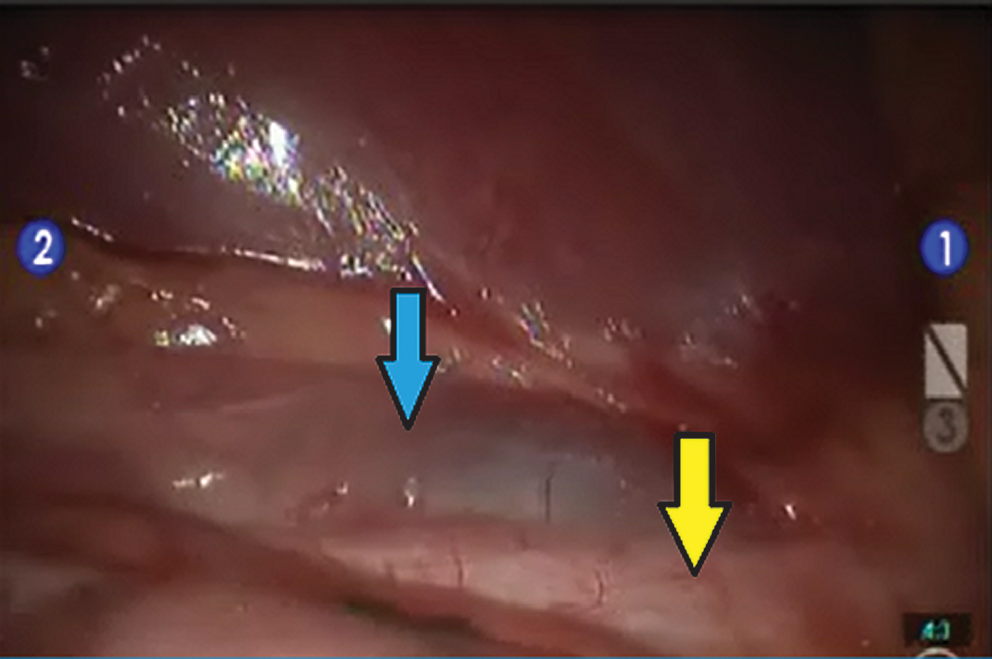
By completely mobilizing the right colon and “kocherizing” the duodenum, the inferior vena cava (blue arrow) and right ureter (yellow arrow) are visualized.
The right ureter is dissected out and retracted using a vessel loop secured to the abdominal wall with a silk suture.
The inferior vena cava (IVC) is exposed and the prbcaval tissue is split to reveal the IVC (blue arrow) and enable dissection of the pericaval lymph nodes (yellow arrow).
Dissection of the right iliac lymph nodes and visualization of the right common iliac artery.
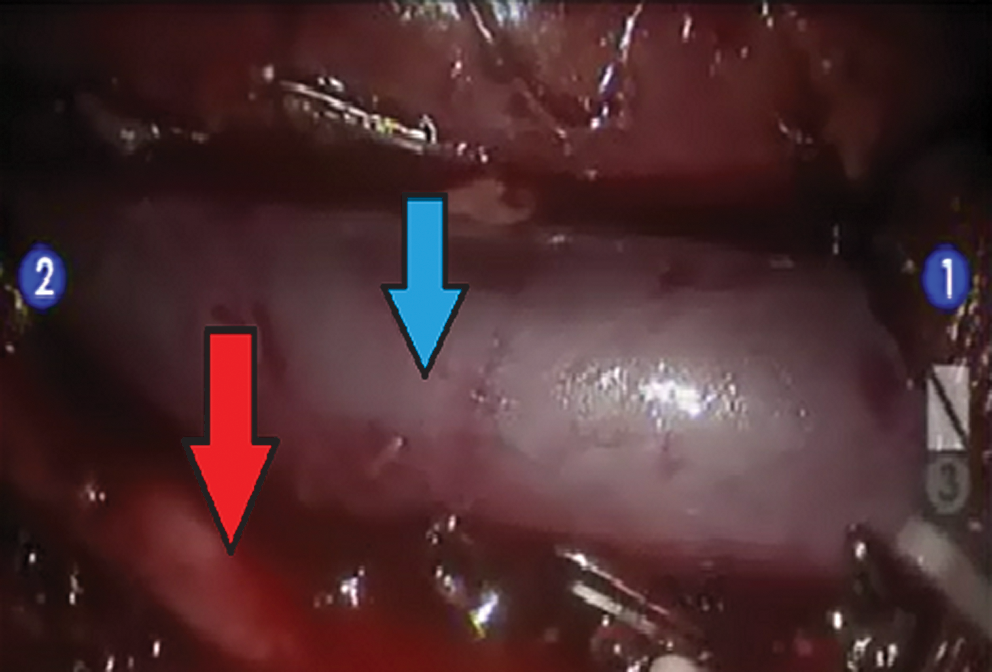
Dissection of the interaortocaval lymph nodes and visualization of the aorta (red arrow) and inferior vena cava (blue arrow).
The operative time was 357 minutes, with 5 mL estimated blood loss (EBL). The patient tolerated surgery well, and recovery was uncomplicated after being discharged home on postoperative day 2. Pathology results revealed 14 negative LNs and per COG/IRS recommendations, the patient received vincristine, dactinomycin, and cyclophosphamide. He is now 16.2 months after RPLND, 3 months off chemotherapy, and remains disease-free with no complications. He reports normal antegrade ejaculatory function.
Case 2
A 15-year-old male presented to the emergency room with a left testicular mass noted that morning. Tumor markers were elevated: Alpha-fetoprotein - 29.9 ng/mL (normal: 0–15 ng/mL) and β-human chorionic gonadotropin - 10.0 IU/L (normal: 0–0.8 IU/L). Ultrasonography revealed an intratesticular mass, and cross-sectional imaging revealed a 1.7-cm para-aortic LN. He underwent left radical orchiectomy, and pathology results demonstrated a 1.2-cm mixed germ-cell malignancy with elements of embryonal carcinoma, yolk sac tumor, seminoma, teratoma, and evidence of LVI. The surgical margins were negative. Postoperatively, tumor markers normalized, and therefore he was stage IIa (T2N1M0S0), and a “good risk” according to the International Germ Cell Cancer Collaborative Group Classification. 9
Accordingly, he underwent three cycles of bleomycin, etoposide, and cisplatin. During chemotherapy, his tumor markers remained normal, but postchemotherapy imaging revealed an increase in the para-aortic mass to 2.1 cm. Therefore, the patient and family were counseled toward a bilateral RPLND with metastasectomy. They were offered both open and R-RPLND, understanding that open RPLND was standard of care and R-RPLND in this setting was considered experimental. They elected for R-RPLND.
Because of the patient's thin body habitus (height 170 cm, weight 57.9 kg, and BMI 20.1) and favorable anatomy, we were able to complete the full bilateral dissection with the patient in the modified left flank position. In the modified flank position, one 12-mm periumbilical camera port, two 8-mm robotic ports (1 midline below the xiphoid, 1 midline above the pubis), and two 5-mm assistant ports were placed (left lower quadrant and RLQ), Figure 1. The left colon was mobilized medially, well past the splenic flexure, which allowed for visualization of the pre- and para-aortic LNs. During this portion of the dissection, it was seen that the inferior mesenteric artery (IMA) was encased with what we were concerned was tumor and pathologically was revealed to be fibrosis and necrosis from treated germ-cell elements. To facilitate a thorough resection, the IMA was dissected and taken, which then allowed the intestines to fall to the point that it allowed full visualization of the aorta, IVC, and bilateral renal vessels. The remnant left spermatic cord and vessels were taken, along with the para-aortic/left renal hilar mass and the bilateral common iliac, para-aortic, preaortic, interaortocaval, precaval, and paracaval LNs.
Because the surgery was bilateral, the difficulty induced by preoperative chemotherapy of the germ-cell elements in the retroperitoneum and the location of the residual masses in the left renal hilum, the resection was tedious and resulted in an operative time of 527 minutes with 100 mL EBL. The patient tolerated surgery well, and recovery was uncomplicated after being discharged home on postoperative day 2. Pathology results revealed treated germ-cell elements and mature teratoma in the residual para-aortic mass in addition to 10 negative LNs, with areas of necrosis and treated germ-cell elements. He is now 12.5 months post-RPLND, disease-free with normal markers, normal imaging, and no complications. He reports antegrade ejaculatory function.
Discussion
The need for RPLND in a pediatric population is uncommon; however, the appropriate use enhances the potential for cure. There is much debate surrounding RPLND for PT-RMS, but given that 30% to 40% of patients with negative LNs on imaging harbor micrometastases, some adjuvant therapy is necessary. Unfortunately, chemotherapy alone does not manage this occult micrometastatic disease, and previous studies demonstrate that adolescents (>10 y) are understaged and undertreated by omitting RPLND. 1,10,11 Thus, the current recommendation is that all patients >10 years with PT-RMS undergo ipsilateral RPLND regardless of CT findings. 1,11
For T-GCT, there is less debate about the role of RPLND, and it is recommended for postchemotherapy residual masses with negative tumor markers and should be offered as an option to patients with low-stage disease but adverse pathologic features. 6 There are differences between the RPLNDs offered in these settings, with an ipsilateral RPLND used for clinically localized disease and a bilateral RPLND used in a postchemotherapy setting. It has been demonstrated that L-RPLND is feasible in both settings; however, there is ongoing debate about its oncologic efficacy compared with open RPLND. 6,8
Recently, L-RPLND was reported as safe with good intermediate-term oncologic outcomes in a pediatric population with PT-RMS. 7 In addition, multiple series on L-RPLND for T-GCT include adolescent patients and demonstrate equivalent intermediate-term oncologic outcomes with lower morbidity than open RPLND. 5,8 The benefits of L-RPLND over open RPLND include decreased complications, improved visualization, cosmesis, decreased hospital stay by approximately 7 days, and a reduced convalescence that translates to higher postoperative quality of life. 5,7,12
In addition to the size and location of the mass, the complication rate of RPLND is also driven by the chemotherapy effect on germ-cell elements in the retroperitoneum. Thus, prechemotherapy RPLNDs are associated with decreased complication rates when compared with postchemotherapy resections. Accordingly, the intra- and postoperative complications of open RPLND are reported as 5% to 12% and 24% to 32%, respectively. Blood loss is the most common intraoperative complication, while chylous ascites, ileus, and small bowel obstruction are the most common postoperative complications. Damage to the retroperitoneal sympathetic nerves resulting in retrograde ejaculation is seen in up to 30%. 13 While the R-RPLND experience is limited, thus precluding comparison, a meta-analysis of L-RPLND demonstrates a decrease in bowel complications and retrograde ejaculation but a higher rate of chylous ascites and vascular injury compared with open RPLND. 14
Whether it be open, laparoscopic, or robot-assisted RPLND, this is a technically complex procedure with potential for complications from extended operative times. Adding laparoscopy or robot-assisted laparoscopy and associated learning curves can extend these times, as demonstrated in a publication of L-RPLND in three adolescents reporting an average time of 382 minutes (245–656), similar to our report, 357 and 527 minutes. While extended, these are at least in the range of reported times for open RPLND with a median of 305 minutes (150–1020) in a recent series. 13
In the robot-assisted laparoscopic prostatectomy experience, a learning-curve for proficiency has been proposed at up to 200 cases. 15 Unfortunately, for RPLND, this volume is not practical, and we recommend using a proctor to facilitate proficiency. The extended operative times for these cases is a matter of concern, and we believe this is directly related to the surgeon's and surgical team's experience with this unique procedure. For this reason, we recommend using an experienced robotic surgery team and a proctor who can advise on issues of port placement, robot docking, and the use of specialized instruments, such as the fanned bowel retractor, the clip applicator, and the LigaSure™ (Covidien, Mansfield, MA). Extensive robotic and laparoscopic surgical experience is certainly helpful, but there are specific technical challenges to R-RPLND; if they can be addressed, it will make for a more efficient procedure. Despite this, one advantage of a robotic system is that operative times can be reduced and safety increased through proctoring and robotic training modules. 16
Naturally, new technology must demonstrate both feasibility and potential additional benefits. Based on the robot-assisted laparoscopic prostatectomy experience, robot assistance enables physicians to more easily and safely incorporate advanced laparoscopic skills into clinical practice. 17 Thus, robot assistance could allow for wider dissemination of minimally invasive RPLND. 18 Also, robot assistance allows for enhanced three-dimensional visualization and more precise surgical instrumentation. This would hopefully enable the surgeon to achieve a complete resection and potentially better nerve sparing.
The visualization of the great vessels and sympathetic nerves was enhanced with our choice of trocar placement, Figure 1, and we did not suffer any intra- or extracorporeal instrument clashing. We prefer the camera port in a periumbilical location accompanied by the robotic ports in a linear orientation, which when the patient is in a flank position, enables the surgeon to be in good “triangulation” with the great vessels where the resection is taking place. This is a well-known and comfortable position for most laparoscopic and robotic surgeons and allows for easy robot docking and minimal instrument clashing.
For unilateral RPLND, we recommend lateralizing the assistant ports to enable assistance when focusing on the side of interest. For bilateral RPLND, however, we found adjusting the assistant ports helpful in bowel retraction to enhance visualization of both sides of the retroperitoneum. In each instance, by keeping these assistant ports in a lateral position, it provides more room for the assistant to help by increasing the distance between the assistant and the docked robot. In addition, we prefer to use the assistant ports over an additional robotic arm/port in this case to allow for the assistant to use a fanned bowel retractor, a clip applicator, or a 5-mm LigaSure. We prefer the fanned bowel retractor during the dissection because it provides good exposure and can be adjusted to be “low-profile” in a variety of positions. Of note, a 10-mm endocatch bag was used to extract the separate specimens during the course of surgery.
In these two cases, we were blessed by favorable anatomy and the patients' body habitus, which facilitated easier dissection. In general, however, we prefer to secure the patients to the table in a flank position. In the case of a unilateral template RPLND, we recommend that side of interest be performed in an ipsilateral flank position. In the case of a bilateral dissection, we recommend starting with a flank position of the side with the residual mass. Most cases will necessitate undocking the robot, adjusting and rotating the table, and potentially even patient reposition to allow for mobilization of the contralateral colon and exposure of the other great vessel. Fortunately, in our case, after being forced to resect the IMA, we were able to complete the resection all from the left side.
In both cases, we could completely dissect the great vessels and resect the nodal basins to perform a technically sound RPLND. Our LN counts of 11 and 14 are comparable to similar reports, such as Tomaszewski and associates, 7 who reported retrieving 10 LNs in a unilateral L-RPLND for an adolescent. 7 While these yields are lower than published adult series reporting yields of approximately 25 nodes in an open bilateral RPLND, 13,19 there are possible explanations. Case #1 was unilateral, which clearly removes fewer nodes, and Case #2 was postchemotherapy, which is known to reduce LN counts in other malignancies. 20
In terms of cost, while robotic instruments cost approximately $1000 more per case than traditional laparoscopic instruments, 21 the reduced convalescence and hospital stay easily recover this cost difference in centers where only open RPLND is offered and L-RPLND is not currently used. We are hopeful that the advantages of R-RPLND will allow more patients to undergo minimally invasive RPLND with reduced morbidity. We present our cases to demonstrate that the benefits of L-RPLND can also be achieved in appropriately selected children and adolescents with R-RPLND.`
Conclusion
While uncommon, some pediatric and adolescent patients with PT-RMS and T-GCT need RPLND. As technology evolves, we must use these advances to provide therapy that minimizes morbidity while maximizing cure. For this reason, we present our series of R-RPLND in an adolescent population demonstrating its feasibility and efficacy.
Footnotes
Disclosure Statement
No competing financial interests exist.