
Abstract
Background and Purpose:
Radiofrequency (RF) is an efficient, inexpensive, safe, and friendly option for the management of small renal tumors. The objective was to evaluate the ideal temperature for renal cell destruction in dogs by RF and to verify whether the injection of vasoactive drugs, such as prostaglandin E1 and adrenaline, can help to improve the results, compared with “dry” RF ablation.
Materials and Methods:
The study was divided into three phases: Initially, 16 dogs of comparable weight underwent RF ablation of the renal parenchyma at temperatures of 80°C, 90°C, and 100°C. After that, seven other dogs received adrenaline (vasoconstrictor) and seven received prostaglandin E1 (vasodilator). Finally, the results from 14 animals were compared with those of the 16 (dry RF) dogs at the optimum temperature found. After 14 days, the animals underwent nephrectomy to evaluate the size of the lesions (width and depth), histology examination, and were then sacrificed.
Results:
There were no clinical or surgical complications in any of the dogs, and none died before the 14th day after the procedure. The optimum temperature was found to be 90°C. Prostaglandin E1 resulted in significantly larger lesions (in depth and width) than adrenaline, with lower impedance. Prostaglandin did not increase the lesions compared with dry RF. All the kidneys presented total coagulation necrosis, with no viable cells in the histologic analysis of the treated tissue.
Conclusion:
In the ablation of renal cells by RF, prostaglandin produced larger lesions (in depth and width) than the same procedure using adrenaline, and its performance was similar to that of RF without injection of drugs.
Introduction
Research on ablation by RF began recently. 2 Nevertheless, the results are promising: The average success rate in the control of renal cancer with RF applied to small tumors with follow-up of more than 19 months is higher than 95%. 2,14
RF works by heating the tissue with an electrical current, promoting cell destruction. The temperature, however, cannot be too high because overly charred tissue creates a gas barrier that obstructs the passage of energy and limits the area of cell destruction, increasing tissue impedance and thereby reducing the efficiency of the RF. 15,16 The ideal temperature and treatment time for the effective destruction of cells, and its extent, are not yet standardized. 17
The “dry” RF ablation procedure involves inserting a needle into the lesions and activating the device. Because electrical conductivity increases in the presence of liquid, researchers worldwide started to introduce saline at the time of RF activation, creating a so-called wet ablation, with an increased area of cell destruction, initially in the liver 18 and then in the kidney, 4 inspiring the verification of the use of substances with different biologic properties. Hypertonic saline, acetic acid (50%), and ethanol have been tested with systemic injections with the aim of reducing tissue impedance at the ablation site. 4 There have been no studies with vasoactive drugs injected at the site of ablation.
Besides reducing impedance, 4 vasoconstrictor or vasodilator drugs could theoretically improve the outcome of RF ablation by enabling a concomitant increase in local temperature, contributing to cell death. Recently, after the publication of international studies in vitro, 19 an experimental study in dogs showed the optimum temperature for the ablation of lesions in the renal parenchyma. 3 The optimum temperature in vivo for the ablation of the renal parenchyma, however, taking into account the impedance of the organ, has not yet been demonstrated.
The hypotheses of this study were: (1) That there would be a difference between temperatures of 80°C and 90°C and 100°C in RF ablation with regard to the extent of injuries; therefore, the study could identify the optimum temperature for ablation of renal parenchyma in the animal; and (2) that the use of a potent vasoconstrictor (adrenaline) or a vasodilator (prostaglandin E1) could interfere significantly in the RF ablation procedure, resulting in a greater area of cell death compared with dry RF, contributing to an alternative for the management of tumors.
The aim of this controlled experimental study in dogs was to define the best conditions for application of RF ablation of renal cells with respect to temperature and the contribution of the use of vasodilator or vasoconstrictor substances, determined by the dimensions and characteristics of tissue injuries and the remaining viable cells in the necrotic tissue.
Material and Methods
Study design, animals, and ethics
This is a prospective experimental study, conducted at the Urological Clinic of Hospital das Clínicas of the University of São Paulo School of Medicine, using the university's vivarium, Medical Research Laboratory 55, and the Vicky Safra Centre for Surgery Teaching and Research (CEPEC), from January 2005 to December 2008. All the experimental procedures were approved by the university's Research Ethics Committee (CAPPesq), with the research protocol number 1078/04. The animals were treated in accordance with the guidelines of the Brazilian College on Animal Experimentation (COBEA), issued in June 1991. 20 The dogs were anesthetized before the surgical procedures and were sacrificed by injection of potassium chloride, also under anesthesia, according to the standards of the University Vivarium.
This study is divided into three parts: The first using a sample of 16 dogs to assess the most efficient temperature for ablation; the second, with 14 animals, using the parameters of temperature and time recorded in the first trial to assess whether the addition of two vasoactive substances influences the histopathologic results; and the third, in which the groups receiving vasoactive drugs were compared with a control group of animals that received no drug. In all the study groups, the RF was applied to the right kidney for technical ease.
The study to evaluate the most efficient temperature for cell destruction consisted of 16 healthy dogs of similar size. Temperatures of 80°C, 90°C, and 100°C were tested in different regions of the same kidney, with cycles of 10 minutes each. Impedance (Ω) was measured on the front panel of the RF device.
The second study, to evaluate the effect of the injection of vasoactive substances during RF consisted of 14 animals. Two subgroups of seven animals underwent RF ablation; one (G1) in which an injection of prostaglandin E1 was used, was compared with another subgroup (G2) in which dogs received an injection of adrenaline in a decimal solution, as described below.
In the third phase, the results of G1 and G2 were compared with the group of 16 dogs used for the study of temperature, considering the optimum temperature found.
The dogs used in this study (Canis lupus familiaris) were all from the same vivarium, all weighing between 14 kg and 16 kg, of undefined breed and of both sexes. For the study, they were housed in individual pens and were taken to the operating room of the laboratory in a fasting state.
RF procedures
The animals were weighed and sedated before the procedure. Under sedation, they were intubated for mechanical ventilation. Each dog was positioned in the left lateral decubitus position. An incision was made in the umbilicus region, followed by puncture with a Veress needle to establish pneumoperitoneum and an entry portal for the 10-mm optical video-laparoscopy. A laparoscopic optical probe was used to locate the kidney for the commencement of the RF procedure.
We used the model 1500 RF generator system of Rita Medical Systems (Atlanta, GA), and RF was applied with a nine-stem Starburst XL needle (same manufacturer) to perforate the renal capsule.
The procedure used in all the dogs was as follows: The needle was inserted through the skin into the most convex region of the kidney, under direct vision using video-laparoscopy. On the front panel, the researchers set the desired temperature and impedance monitoring during the RF procedure. In the first experiment, RF was applied at temperatures of 80°C, 90°C and 100°C, comparing different regions of the kidney, in cycles of 10 minutes.
In the second study, the aim of which was to evaluate the use of vasoactive medication, the drug was inserted through the needle immediately before applying the RF energy. Once the Starburst plunger was pushed in 2 cm, it opened at its distal end, allowing the passage of the substance. Then, at the moment of RF activation, the RF waves passed through the stems of the needle, also in a diameter of 2 cm. The drugs infused into the renal parenchyma were prostaglandin E1 (1 mL or 20 μg) in the seven dogs in G1, and 2 mL of 1:1000 of adrenaline (1 mL diluted in 9 m: of distilled water) in the seven dogs of G2. After the drug injection, 1 cycle of 10 minutes of RF was applied, at the optimum temperature, as in the first part of the experiment, with 100 watts of power. The impedance values were measured and recorded during the application of RF.
Evolution, sacrifice, and histologic analysis
The incision was sutured with mononylon 3-0; each dog was extubated after recovery from anesthesia, and soon afterward the dog was returned to the bay where it was kept under observation, received veterinary care, and was fed (with dog food and water ad libitum). There were no deaths among the animals during the postoperative observation period. The animals were clinically observed for 14 days postoperatively, for bowel habits, urine, and general condition.
Fourt een days after surgery, the dogs were anesthetized by the same methodology, and nephrectomy was performed by laparotomy. An inventory was made of the abdominal cavity (looking for bruises, urinoma, etc.) and the dogs were sacrificed while still under anesthesia.
Histopathologic analysis of the lesions was performed: Macroscopic analysis (Fig. 1), weight of the tissue block, and identification number of each tissue block. The kidney was sectioned at the level of the lesion produced by RF, and its size (width and depth) was measured as follows: • The width was considered the largest dimension of the kidney lesion in the craniocaudal direction. • The depth was considered the largest measurement in the anteroposterior direction. • Necrosis: Absence of viable cells under optical microscopy with hematoxylin and eosin (H&E) staining.

Dog kidney with a necrotic lesion resulting from radiofrequency application.
To identify the largest diameter of the tumor, at least three parallel cuts were made in the greater axis of the lesions.
The piece containing the injured tissue was cut with a microtome, and slides were prepared and stained with H&E. The material containing the lesion was placed in paraffin blocks, and the slides were numbered and examined under an optical microscope to check the area of coagulation necrosis. The pathologist who examined the samples was unaware of which technique was used in each case.
Histologic data were recorded for the variables: Depth, width of the lesion, and the presence of viable (live) cells in an area subjected to ablation. The impedance measurement was recorded and correlated with the size of the lesions.
Statistical analysis
Initially, we examined the distributions of four variables: Depth, width, impedance, and necrosis. The width, depth, and impedance data were expressed as means, standard deviations, minimum and maximum values, for each temperature.
The variables width and depth and cell necrosis had normal distribution, as shown by the Shapiro-Wilk normality test (P=0.44 and P=0.99, respectively). The variable impedance was not normally distributed according to this test (P<0.001).
In the case-control group comparison, the width and depth variables were normally distributed (P corresponding to the kurtosis normality test of=0.86 and 0.14. respectively). The c (P=0.002).
To compare the distributions of variables width and depth according to the drugs used (adrenaline or prostaglandin E1), the Student t test was used for two independent samples, preceded by the test of equal variances. To compare the distributions of the variable impedance according to the same groups, the Mann-Whitney test was used.
These data were analyzed by constructing a model of analysis of variance (ANOVA), with repeated measurements and comparisons for the construction of contrasts. ANOVA was used for one factor, followed by multiple comparisons (Bonferroni method).
Significance was assumed to be P≤0.05. The statistical analysis was performed using the statistical program Stata (version 9.0).
Results
There was homogeneity among the groups of dogs in relation to the animal's sex and weight. This was also reflected in the kidney weight, which did not show any significant change between the groups of dogs. During the 14-day observation period after each experiment, no clinical or surgical complications were seen among the operated dogs. None of them died before the end of the study period, and all the kidneys could be properly examined. There were no hematoma or urinoma collections in the abdominal cavity.
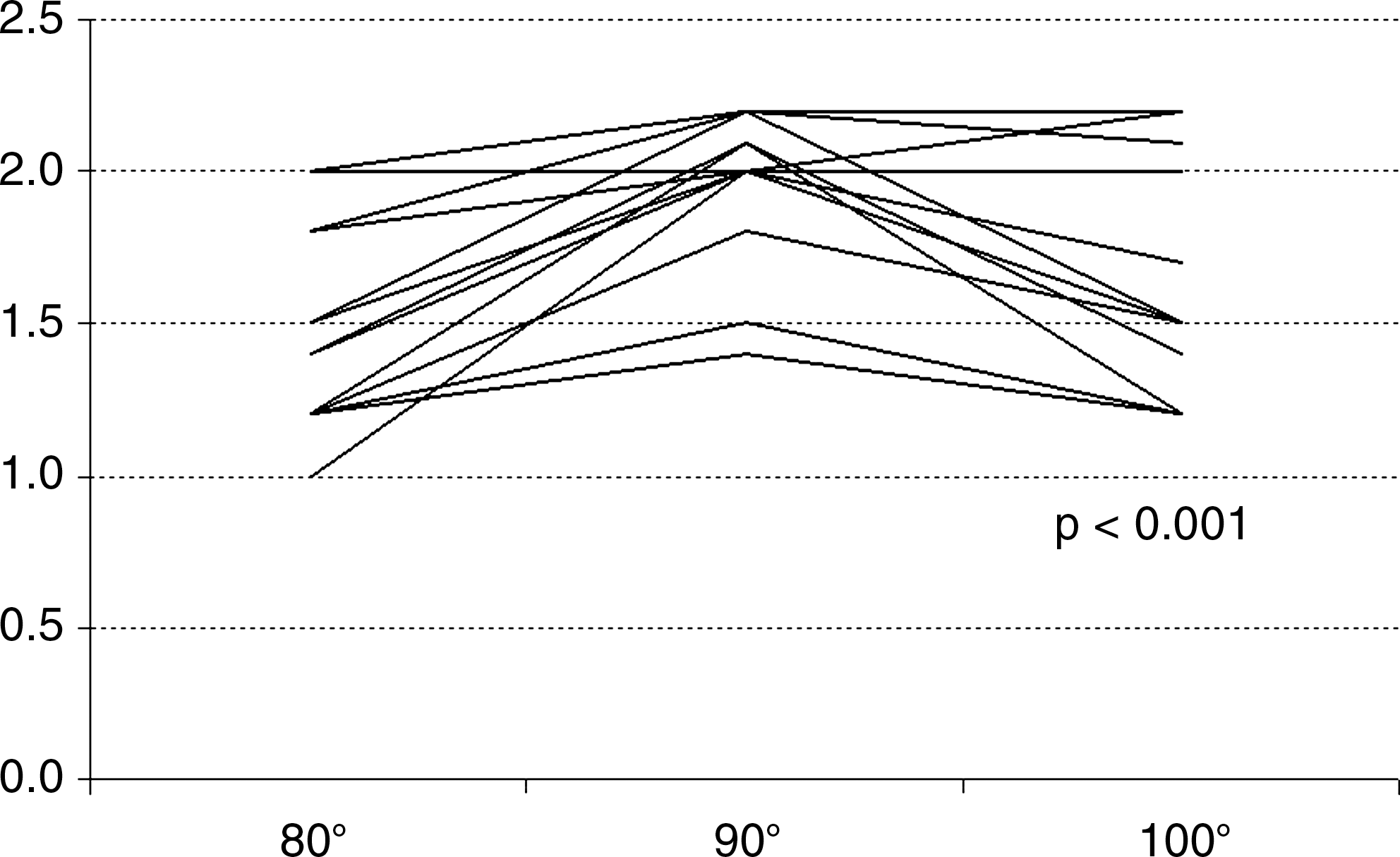
The first experiment was conducted to identify the best temperature for cell destruction. Figure 2 shows that there is a peak in the size of the renal lesions at the temperature of 90°C and a similar result for depth at temperatures of 80°C and 100°C. A statistically significant difference in lesion depth was found between the three temperatures (P<0.001). In Figure 3, we see that there is a peak in the size of the renal lesions at the temperature of 90°C, and a similar result was found for width at temperatures of 80°C and 100°C. A significant statistical difference was found in the width of the lesion at the three temperatures (P<0.001). According to Figure 4, there was a more favorable outcome at the temperature of 90°C (lower impedance) and similar outcomes for the temperatures of 80°C and 100°C.

Individual profile of lesion depth according to temperature.
Individual profile of lesion width according to temperature.
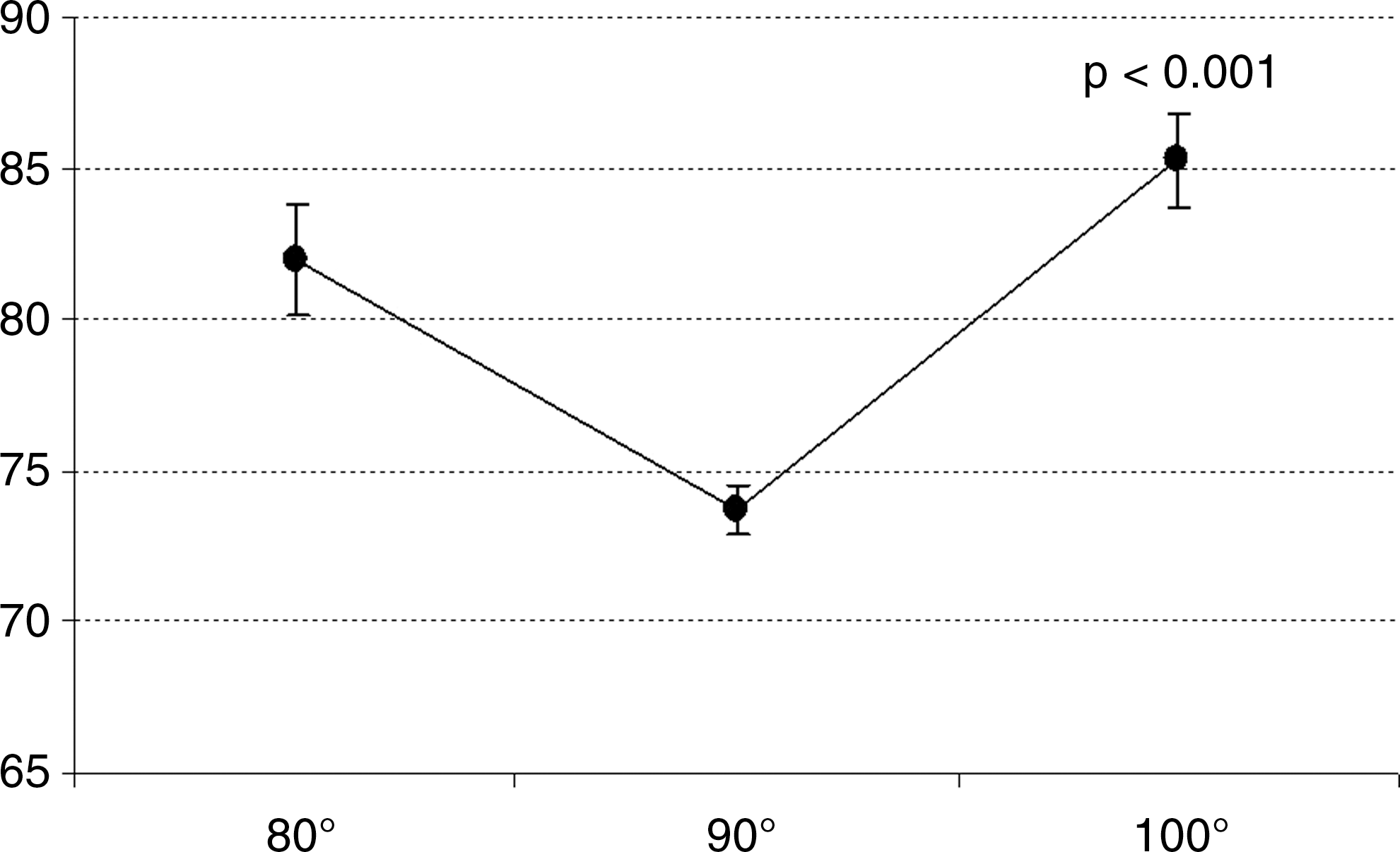
Average impedance profile according to temperature.
There was a statistically significant difference in impedance between the three temperatures studied (P<0.001). For both, width and depth, the highest mean occurred at 90°C, and for the impedance, the lowest mean also occurred at 90°C.
The second experiment was then initiated using a temperature of 90°C during all the RF procedures. There was no change in the number of male or female dogs treated with either drug (P>0.999), or in the animals' weights, as was expected (P=0.620). This homogeneity of body weight was again reflected in kidney weight, which did not change among groups of dogs receiving adrenaline or prostaglandin E1 (P=0.535).
The use of prostaglandin E1 resulted in significantly larger and deeper lesions than the use of adrenaline (P=0.05; P=0.02). Table 1 and Figure 5 show that impedance was lower with injection of prostaglandin E1, whereas there was minimal variation in average impedance with the use of adrenaline (Table 2).
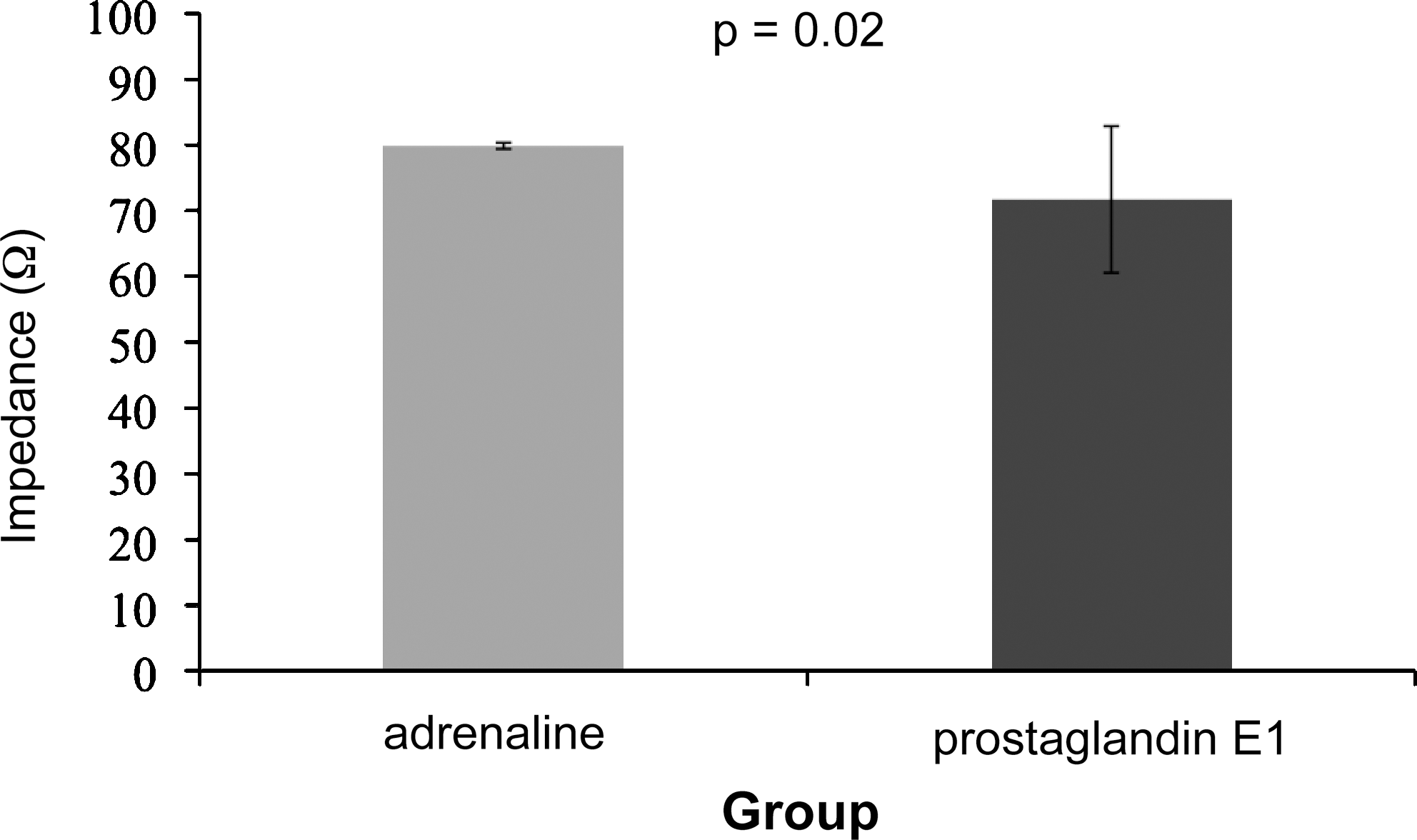
Comparison of impedance (Ω) of the lesion resulting from radiofrequency ablation with adrenaline injection vs prostaglandin E1.
P corresponding to the Student t test for two samples.
P corresponding to the Mann-Whitney test.
Table 3 and Figure 6 analyze G1 and G2 compared with a control group without drug injection (dry RF). There was a significant difference among the three groups, in terms of width of the lesions (ANOVA, P<0.001). The lesion of the control group was, on average, 0.65 cm wider than that of the adrenaline group (P<0.001), and that of the prostaglandin E1 group was, on average, 0.71 cm wider than that of the adrenaline group (P<0.001). There was no significant difference between the groups prostaglandin E1 and control (P>0.99).

Width of the lesions in the three groups (n=30).
p corresponding to the Analysis of Variance (ANOVA).
Figure 7 shows a significant difference among the three groups in terms of lesion depth (ANOVA, P=0.02); the lesion depth in the control group was, on average, 0.51 cm greater than that of the adrenaline group (P=0.02). The depth of the prostaglandin E1 group was, on average, 0.54 cm greater than that of the adrenaline group (P=0.04). There was no significant difference between the prostaglandin and control groups (p>0.99).
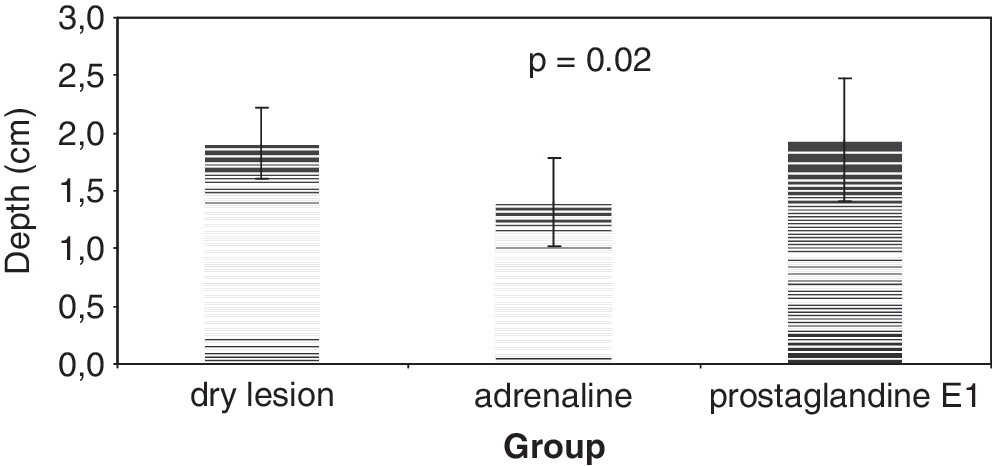
Depth of the lesions in the three groups (n=30).
In all the experiments, all the treated kidneys had complete coagulation necrosis in the areas subjected to RF ablation, with no islands of viable cells.
Discussion
RF ablation in renal masses is already widespread in the therapeutic armamentarium2; it is effective in causing destruction of tumor cells and is considered a minimally invasive procedure with low morbidity. It is a technique, however, that is still being developed and lacks clearly defined parameters to improve the quality of the procedure and long-term treatment.
Research in RF ablation started with the liver and then extended to the kidneys and lungs. Early studies involving the kidney, with at least 1 year of follow-up, were published since 2004 10,14,21,22 and demonstrated a success rate of more than 94% for the control of kidney cancer for tumors smaller than 4 cm. 2 These studies used different temperatures for ablation, mostly based on the temperature of 105°C, a parameter used in the liver. 17
The ablation equipment consists of an RF generator, with an electrode that is inserted into the target tissue, generating a high-frequency alternating current that passes through the tissue. The ionic turmoil caused by the current heats the tissue to temperatures sufficient for cell death (coagulation necrosis). Cell homeostasis is maintained at temperatures of up to 40°C. When the temperature rises to 42°C to 45°C, the cell becomes more susceptible to injury by other agents, such as chemotherapy and radiation. 23 Increasing the temperature to 46°C for 60 minutes leads to irreversible cell damage. 24 By increasing it to 50°C to 52°C, the time needed to induce cytotoxicity is reduced to 4 to 6 minutes. 25 Between 60°C and 100°C, an almost instantaneous protein coagulation occurs, which frequently progresses to coagulation necrosis. 26 Temperatures higher than 105°C lead to tissue boiling, vaporization, and charring. This carbonization causes the formation of gas at the periphery of the lesion, restricting the transmission of energy. Thus, the optimum temperature was reported in the literature as between 50°C and 100°C. 25
In 2007, Walsh and associates 19 succeeded in establishing an ideal temperature for the death of renal tumors at three different exposure times, but in an experimental in vitro study with cell cultures. The temperature ranged from 55°C to 65°C. In the organ tissues, however, the heat is distributed heterogeneously. In general, the temperature is greater near the needle and it is lower farther away, because there is no full conductivity of heat to the periphery. 25
In our study, we found the optimum temperature for renal RF ablation to be 90°C, this being the temperature that allowed the lowest impedance, improving heat distribution in the tissue and promoting greater tissue injury. 3 The temperature of 90°C was, therefore, used as a standard, which was compared with animals that also received injections of adrenaline and prostaglandin E1.
Another method, concurrent with RF, is to promote cell death by freezing, which causes the formation of crystals and results in dehydration of the cell. In this case, therefore, it is lower temperatures, rather than higher, that produce the desired clinical outcome. 27 A recent meta-analysis comparing cryoablation with RF in the management of renal tumors included 47 studies, representing 1375 lesions. The study concluded that local cancer control and the re-treatment rate were better with cryotherapy. Of the studies included in the review, however, 65% of procedures were performed by laparoscopy and 92% of RF procedures were performed percutaneously. 28 It is worth noting that the laparoscopic approach allows better positioning of the probes, while with the percutaneous approach, no imaging examination provides a satisfactory image that can serve as a guide. In this study, the renal puncture was performed with laparoscopic guidance, as described.
The lesion produced by cryotherapy (ice ball) is easily visualized by ultrasonography, 29,30 but the same test is not able to provide a clear picture of the damage caused by RF. 29,30 Being a dynamic examination, performed in real time, ultrasonography can still be widely used in RF ablation. 4 A possible bias in the evaluation of cryotherapy is the difficulty of locating the renal lesion produced by percutaneous treatment, which was evident in another meta-analysis in which it was shown that the effectiveness of percutaneous renal tumor ablation is 87%, significantly lower than among patients who underwent an open or laparoscopic approach (94%) using only RF. 31
Cryotherapy treatment is effective but costly. In most cases, it necessitates laparoscopy equipment, which involves higher investments than percutaneous equipment. 28 Laparoscopic partial nephrectomy, which also competes with RF, has a significantly higher cost than RF. 32,33 Also, it normally needs the use of a laparoscope. The cryotherapy device is larger, heavier, and more expensive than RF. Precisely because of its economic feasibility and practicality, the destruction (“burning”) of renal tumor tissue by RF is a theme in which research is advancing quickly. Having established the optimal temperature for RF ablation, 3 the investigations should now be focused on improving the technique, through increased and better control of the lesion area and improved histologic outcome.
The literature indicates a limit of 3.7 cm as the maximum size of tumors that would be candidates for RF ablation: For larger tumors managed by RF, the risk that the treatment will not be complete—ie, remaining tumor cells at the periphery of the tumor—is significantly higher. 34 Since this limit was established, techniques for improvement of RF have been studied.
One of the keys to improvement of this technique may be the evaluation of impedance; ie, tissue resistance to transfer of the current. In this regard, there is evidence that it is possible to improve the resistance (by decreasing the impedance), changing the temperature by cooling the tissue immediately adjacent to the probe 35 and improving the electrical conductivity by injecting saline into the liver tissue at the time of activation of the RF needle. 18,36 –38 This ensures a more uniform temperature throughout the lesion and not just around the needle. This principle of liquid acting on the homogenization temperature was further investigated in the kidney. 39 Different liquid solutions have also recently been successfully tested in porcine kidney tissue. 4
The research area of wet RF was promising during the planning of this work. Based on the premise that the presence of blood flow interferes with electrical and thermal conduction in the renal lesion, we decided to investigate whether the histologic effects of RF ablation would be modified not only by saline, but also by drugs that interfere with the circulatory mechanics, and therefore the presence of liquid “blood” in the injury to be produced. Thus, we planned to compare a vasoconstrictor and a vasodilator drug in the procedure of renal ablation by RF in dogs. We also compared the efficacy of this procedure with the dry lesion at a temperature of 90°C.
Adrenaline is a substance capable of causing vasoconstriction. It is used in conjunction with local anesthetics to decrease systemic absorption of these drugs. Its vasoconstriction action would, hypothetically, have a beneficial effect on RF ablation by reducing the caliber of the renal vessels, allowing better distribution of the electric current around the tumor and throughout the parenchyma. 40,41 In the first phase of the study with dogs of similar sizes, 3 we found that even without the injection of substances, RF ablation is capable of producing coagulation necrosis in the renal parenchyma. In the second phase of the study, we tested the use of adrenaline in RF ablation for the first time and also produced adequate coagulation necrosis in the renal tissue of dogs, with no islands of viable cells in the middle of the lesion produced by heat. In the third stage, however, we found that the lesion caused by RF with adrenaline was smaller than the lesion in the dry RF group and smaller than in the group receiving prostaglandin. This finding rules out the hypothesis that adrenaline can be used to help increase kidney damage in healthy tissue of dogs.
The use of prostaglandin E1, on the other hand, has shown promising, innovative, and impressive results in this line of research. The width (P=0.002) and depth (P=0.05) of renal lesions in this study were significantly higher in the dogs that received prostaglandin E1. In 2007, Friesenecker and colleagues 42 published a study that provides a physiological explanation for this finding.
The authors 42 injected intravenous prostaglandin E1 (2.5 μg/kg/min) in hamsters and measured oxygen availability in the circulation and tissue of the vessels before and after the injection. Besides the expected vasodilation, there was also up to 50% of tissue availability of oxygen after the drug use. 42 The oxygen, which increased in the tissue because of the injection of prostaglandin E1, would also increase thermal diffusion in the parenchyma region subjected to RF, through the phenomenon of combustion, enhancing the effect and amplifying the RF lesion. In the third phase of our study, prostaglandin showed a better performance than adrenaline. No statistically significant difference was achieved, however, between the group that received prostaglandin and the dogs submitted to dry RF. This phenomenon may perhaps be explained by the small sample.
In this experiment, the RF was applied in the healthy kidney cells, which could be a criticism, because the objective of developing the technique is to treat tumors. Tumor cells, however, are more sensitive to RF than healthy cells. 43
The application of RF is not without risks. Its potential complications include: Urinary leakage, bleeding, hematuria, stenosis of urethral segments and ureteropelvic junctions, hematomas, renal infarction, and abdominal wall tumor implantation. 43 In this study, none of these complications were observed in the animals.
For the histologic analysis, the renal cells subjected to the action of RF can be stained with H&E or nicotinamide adenine dinucleotide (NADH). In the case of evaluation immediately after the application of RF, NADH is suitable for analysis of cell destruction. For later analysis, however, the use of H&E is considered more appropriate. 44 Moreover, some authors highlight the possibility of incomplete destruction of the tumor cells and the remaining of viable cells in the areas subjected to RF by insufficient heat. 44 For a safer analysis, we waited 14 days after RF application before assessing cell vitality and also the extension of the lesion with H&E. 43
Conclusion
The optimum temperature for inducing cell destruction by RF was 90°C, because this temperature produced more extensive lesions in terms of width and depth, compared with temperatures of 80°C and 100°C. The impedance was also lower at 90°C. There were no viable cells in the microscopic analysis within the limits reached by RF.
Prostaglandin E1 used in the RF ablation procedure was capable of causing significantly higher renal damage in terms of width and depth than the same procedure using adrenaline. The tissue impedance was significantly lower in the group in which prostaglandin E1 was used. The procedure of RF with injection of prostaglandin was not more effective than the dry RF procedure. RF ablation with the addition of both adrenaline and prostaglandin E1 caused complete tissue destruction; ie, no live cells remained in the treated kidney tissue.
Footnotes
Disclosure Statement
No competing financial interests exist.