
Abstract
Purpose:
To define in which patients who present with microscopic or macroscopic hematuria CT urography (CTU) is indicated as an imaging mode for the upper urinary tract (UUT).
Patients and Methods:
We conducted a prospective study on consecutive patients who attended a modern protocol-driven hematuria clinic from January 2006 to February 2010. Standard tests (history taking, physical examination, urinalysis via dipstick method, ultrasonography of kidneys and bladder performed by urologists, cystoscopy, and cytology) were directed to all patients, whereas the mode of additional UUT imaging (ultrasonography by a radiologist or four-phase CTU/magnetic resonance (MR) urography (MRU) when CTU was contraindicated) was selected according to a risk factor-based management algorithm. The added value of cross-sectional urography (CTU/MRU) supplementary to ultrasonography (by urologists) to detect renal masses, UUT tumors, and stones was assessed. Univariate and multivariate analysis on predictive factors for cross-sectional urography result were performed.
Results:
From the total of 841 patients, lesions that might account for hematuria could not be identified in 462 (54.9%), whereas in 250 (29.7%) and 124 (14.7%) patients, hematuria was from benign and malignant disease, respectively. Cross-sectional urography revealed relevant UUT lesions in 73 of 525 (13.9%) patients. Only result of ultrasonography (odds ratio [OR] 7.7, 95% confidence interval [CI] 4.0–14.9), P<0.001) and type of hematuria (OR 2.6, 95% CI 1.3–5.1, P=0.01) were significant predictors for cross-sectional urography result. In 44 of 456 (9.6%) patients with no abnormalities on ultrasonography, CTU/MRU revealed that these were false negatives, with most lesions missed being stones. In 253 of 309 (81.9%) patients with macroscopic hematuria, no lesions were detected in the UUT on CTU/MRU, in contrast to 199 of 216 patients (92.1%) with microscopic hematuria.
Conclusion:
For patients who present with microscopic hematuria, ultrasonography is sufficient to exclude significant UUT disease. For patients with macroscopic hematuria, the likelihood of finding UUT disease is higher, and a CTU as a first-line test seems justified.
Introduction
This study was conducted to define in which patients who present with microscopic or macroscopic hematuria CTU is indicated as an imaging mode for the UUT.
Patients and Methods
Study design
We conducted a prospective study on all consecutive patients who attended a protocol-driven hematuria clinic for the first time from January 2006 until Febriary 2010. Demographic variables, details of medical history, and type and results of examination, diagnosis, and therapy were recorded in an electronic database.
Hematuria clinic
Patients were referred by general practitioners, consultants from other departments in the hospital, or they learned about the clinic through the Internet and made an appointment on their own initiative.
The hematuria clinic was designed according to a specific testing algorithm. Each patient who attended the clinic underwent extensive history taking (including smoking habits, occupation, medication use, previous treatments), physical examination (including digital rectal examination [men] or vaginal examination [women]), urinalysis via dipstick method (Multistix® 8 SG analysed with Clinitek Status, Siemens Healthcare Diagnostics, Breda, the Netherlands), ultrasonography of the kidneys and bladder and flexible cystoscopy complemented with bladder washout cytology. Microscopic hematuria was defined as ≥17 erythrocytes/μL, which is comparative to >3 erythrocytes/field of view. 8 In general, dipstick hematuria had to be confirmed by microscopic urinalysis. If the urinary dipstick demonstrated an active urinary tract infection (UTI) defined as positive testing for nitrite and/or leucocytes, urine culture was performed and cystoscopy was postponed until UTI was treated adequately. Both the ultrasonography (Philips iU22, Bothell, WA) and cystoscopy (Olympus CYF-V2 flexible chip-on-the-tip cystoscope with Olympus Visera video system, Olympus Europa Holding GmbH, Hamburg, Germany) were performed by experienced residents of urology supervised by a staff member.
Additional four-phase CTU for upper tract imaging was performed in case of abnormal findings on cystoscopy or ultrasonography, or in patients with risk factors for significant disease as defined by the American Urological Association best practice policy. 2 The risk factors taken into account were: age 40 years or older, history of gross hematuria, irritative voiding symptoms, occupational exposure to chemicals or dyes, smoking history, or urologic history. In patients with renal insufficiency (roughly defined as creatinine level above 130 μmol/L) or allergy for iodine-containing contrast agents, a magnetic resonance (MR) urography (MRU) was performed instead. For all other cases, additional plain abdominal radiography of the kidneys, ureters, and bladder and ultrasonography (Philips iU22, Best, the Netherlands) by the department of radiology was requested. This algorithm is displayed in Figure 1.
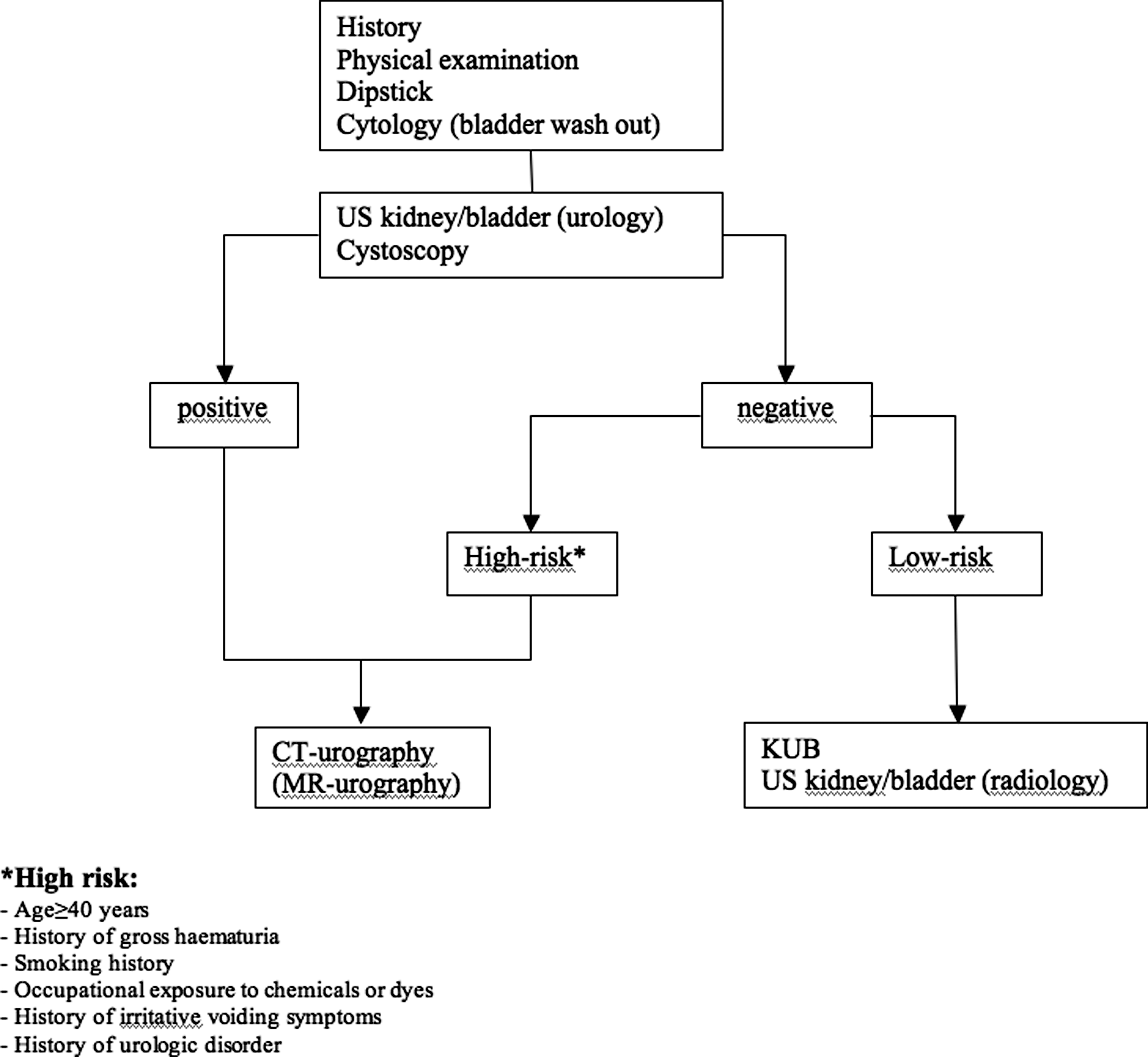
Flowchart for protocol for patients who present with hematuria. US=ultrasonography; CT=computed tomography; MR=magnetic resonance; KUB=X-ray of kidneys, ureters, and bladder.
CTU/MRU protocol
The scanning protocol for CTU was performed without oral contrast or bowel preparation using a 64 multidetector CT (Brilliance-64, Philips Medical Systems, Best, the Netherlands). The total amount of contrast used was 120 mL of 300 mg/mL iodine (Ultravist 300,® Bayer-Schering, Berlin, Germany) followed by a saline flush of 40 mL. The flow of infusion was 4 mL/sec. The whole imaging protocol consisted of acquiring 3 mm reconstructed axial images in four phases: A plain series of the total abdomen (from diaphragm to perineum) for the detection of urinary stones, a corticomedullary phase (after 45 seconds) of the upper abdomen (from diaphragm to iliac crest) for the evaluation of renal masses and lymph node or liver metastases, a nephrogenic phase (after 115 seconds) of the total abdomen for renal masses and lesions of the urinary tract, and finally, a delayed phase (after 10 minutes) of the total abdomen for the detection of filling defects of the urinary tract including the bladder.
The MRU protocol was also performed without oral contrast or bowel preparation using a 1.5 Tesla MRI (Avanto, Siemens Medical Systems, Erlangen, Germany). The contrast used was 0.2 mL/kg bodyweight, 0.5 mmol/mL gadolinium (Dotarem®, Guerbet, Gorinchem, the Netherlands). Imaging was performed from diaphragm to perineum and consisted of four plain series: coronal T2 (TRUE FISP) with fat saturation (fatsat), transverse T2 (HASTE) with and without fatsat, transverse three dimensional (3D) T1 (VIBE) with fatsat before contrast, followed by seven contrast series: Transverse 3D T1 (VIBE) with fatsat at contrast injection and after 30 and 60 seconds, coronal 3D T1 (VIBE) with fatsat at 5 and 10 minutes after contrast injection, and finally transverse and coronal 3D T1 (VIBE) with fatsat 15 minutes after contrast. All the transverse VIBE series, with exception of the last, were performed of the upper abdomen, including the kidneys.
Outcome measures and statistical analysis
Patient characteristics, presenting symptoms, an overview of diagnoses, and details of benign and malignant causes of hematuria in this population were summarized. Descriptive results are presented as mean±standard deviation for parametric variables and as median with interquartile range for nonparametric variables.
The results of cross-sectional urography (CTU or MRU) supplementary to initial ultrasonography (performed by a urologist) to detect renal masses, upper tract tumors, and stones in the ureter or kidney were assessed. For a representative assessment of the diagnostic value of CTU in clinical practice, the report of the prospective reading of the CTU scan constructed by a radiologist who was informed about clinical details by the referring urologist was used, instead of an independent retrospective evaluation of the scans by a radiologist blinded for clinical details. Baseline factors predicting relevant UUT disease on cross-sectional urography were assessed (CTU/MRU+ or -) with univariate and multivariate analysis. The following variables were tested: Sex, age (both mean and clustered in decades), type of hematuria, smoking history (in pack years), occupational risk exposure, symptoms, and use of anticoagulant therapy. To evaluate the value of ultrasonography performed by a urologist as a first-line test, the relation between the results of CTU/MRU and ultrasonography were explored. Independent t tests were used for parametric continuous variables and Mann-Whitney tests for nonparametric data. Pearson chi-square tests were used for categorical variables and logistic regression for multivariate analysis. In addition, incidental findings on cross-sectional urography and their clinical significance were described.
Statistical analysis was performed using the Statistical Package for Social Sciences, version 16.0 (SPSS, Chicago, IL), and P<0.05 was considered statistically significant.
Results
From January 2006 until February 2010, a total of 841 patients visited the hematuria clinic for the first time. Patient characteristics are presented in Table 1. Lesions that could account for the hematuria could not be identified in 462 (54.9%) patients, whereas in 250 (29.7%) and 124 (14.7%) patients, hematuria was from benign and malignant disease, respectively. An overview of causes for hematuria (benign, malignant, no urologic cause, or missing) in this population with stratification for sex, age, type of hematuria, and symptoms is shown in Table 2. Details of the benign and malignant diagnoses are presented in Tables 3 and 4, respectively.
SD=standard deviation; IQR=interquartile range.
LTFU=lost to follow-up.
INR=international normalized ratio.
No pathology: Transurethral resection performed in other hospital (two patients) or expectative management because of comorbidities (three patients).
Value of CTU/MRU for detecting UUT disease
Based on the above mentioned criteria, in 617 patients, additional cross-sectional UUT imaging was indicated. This comprised CTU in 521 patients, MRU in 12 patients (because of renal insufficiency in 11 patients and iodine contrast allergy in 1 patient), and in 84 patients the protocol was breached and IVU was requested. Request of IVU occurred mainly just after the protocol was introduced, in the transition between former management that still used IVU. Because some patients did not show up for the requested examinations, even not when asked repeatedly, 515 (CTU) and 10 (MRU) cross-sectional studies eventually were available for analysis.
From all 525 cross-sectional imaging studies, 452 (86.1%) revealed no abnormal UUT findings while 73 (13.9%) studies did. Not all CTU/MRU findings were registered as the final diagnosis for the hematuria. In 5 of the 50 patients in whom stones in the ureter or renal pelvis were detected on CTU, these were subordinate to other causes (bladder tumor, UTI, radiation cystitis, and urethral meatal stenosis). In one of nine patients with an UUT tumor detected on CTU, this was not listed as cause for hematuria because of the presence of a much more prominent bladder tumor. In 14 patients, a renal mass was detected, and in 10 patients, the image was compatible with renal-cell carcinoma and in 4 with a small angiomyolipoma. At least for the two patients who presented with macroscopic hematuria, the angiomyolipomas were too small and too far from the collecting system to be a likely explanation for the hematuria.
The only statistically significant predictors for + and − cross-sectional urography cases were type of hematuria and initial ultrasonography results, on both univariate and multivariate analysis (Table 5). The CTU/MRU findings for these two variables are specified in Table 6.
Independent t test.
Chi-square test.
Mann-Whitney test.
CTU=computed tomography urography; MRU=magnetic resonance urogrphy; OR=odds ratio; CI=confidence interval; SD=standard deviation; IQR=interquartile range.
UUT=upper urinary tract.
CTU/MRU results in relation to results of ultrasonography (performed by urologist)
In 69 of the 525 patients who underwent cross-sectional imaging, initial ultrasonography was suspect for a renal or urothelial tumor or stones. In 40 (58%) of them, the initial ultrasonography was false-positive (for stones in 18 and tumor in 22 patients) because cross-sectional imaging could not confirm this. From the 22 suspected tumors on ultrasonography, 10 lesions were finally determined to be benign renal cysts.
In 456 patients, the ultrasonography results were negative (eg, no lesion or only dilation seen), and in 44 (9.6%), CTU/MRU revealed that these were false negatives, with the majority of lesions missed being stones (Table 6). In 10 of 32 (31.3%) patients with stones that were not detected on ultrasonography, active treatment was indicated; eg, ureteroscopy (URS) (5 patients), percutaneous nephrolithotomy (three patients), and shockwave lithotripsy (2 patients). From the seven UUT tumors detected only on cross-sectional imaging, four were managed with nephroureterectomy, one with URS and laser fulguration, and in two patients, an expectant management was chosen (because of patients' age/comorbidities and because of metastatic disease in the ureter from a primary cholangiocarcinoma, respectively). From the five renal masses detected only on cross-sectional imaging, all three renal-cell carcinomas were managed actively (two with radical nephrectomy and one with nephroureterectomy because of primary suspicion of urothelial carcinoma on CTU). The two patients with angiomyolipomas detected only with CTU are still in follow-up without a need for active treatment so far.
CTU/MRU results in relation to type of hematuria
In total, 309 patients who underwent cross-sectional imaging presented with macroscopic hematuria and in 253 (81.9%) of them, no lesions were detected in the UUT on CTU/MRU. From all gross hematuria patients, 209 were men (67.6%) and 100 (32.4%) were women. The type of macroscopic hematuria was unknown in 64 (20.7%) patients and defined as initial, total, or terminal in 34 (11%), 175 (56.6%), and 36 (11.7%) patients, respectively. No association was found between these two variables and CTU/MRU results (type of gross hematuria: χ2(3)=9.01, P=0.06; sex: χ2(1)=0.89, P=0.35).
In 199 of 216 (92.1%) patients with microscopic hematuria, no abnormalities were detected on UUT cross-sectional studies. From the 17 patients with microscopic hematuria who did have UUT disease on CTU/MRU, 12 had stones and 5 a renal mass (2 angiomyolipomas, 3 renal-cell carcinomas). One patient with a stone needed active treatment with URS, and 1 patient with renal-cell carcinoma underwent nephrectomy; the angiomyolipomas and other 2 renal masses were managed with active surveillance because of small size and comorbidities, respectively. From these 17 lesions, 9 were not yet detected on ultrasonographic examination (8 stones and 1 angiomyolipoma). None of the lesions missed with ultrasonography needed active treatment, however.
Incidentalomas
Incidental findings were discovered in 139 (26.5%) of 525 cross-sectional imaging studies. The majority were benign liver lesions (33.8%), followed by cholelithiasis (12.9%), adrenal lesions (11.5%), diverticulosis (10.1%), anomalies to the female reproductive tract (9.4%), aortic aneurysms (diameter ranging from 28–65 mm) (6.5%), hepatic steatosis (4.3%), pulmonary nodules (4.3%), metastases of nonurologic primary tumor (2.2%), benign spleen lesions (2.2%), malignant liver lesion (0.7%), liver cirrhosis (0.7%), retroperitoneal fibrosis (0.7%), and ureteropelvic junction stenosis (0.7%). Of these, 14.4% were potentially life threatening (aortic aneurysm, malignant lesions, liver cirrhosis), whereas 40.2% may need further evaluation.
Discussion
This article represents the largest published prospective series of CTU as a diagnostic modality of UUT imaging for both macroscopic and microscopic hematuria patients. Although it has been proven that CTU outperforms IVU in terms of diagnostic accuracy, the modality in itself has some obvious disadvantages. The major drawback is the increased radiation hazard. Each CTU delivers about 25 to 35 mSv to the patient, depending on the number of image acquisitions. 9 Knowing that the radiation dose of a typical adult abdominal CT, which is in the range of ±10 mSv, already can increase the risk for development of cancer, 10 the hazard of CTU should not be underestimated. An additional disadvantage of CTU is the need to use iodine-containing contrast agents, which may pose danger to the patients' renal function or even be accompanied by serious side effects (eg, anaphylactic shock). 7 Furthermore, CTU is relatively expensive.
Nevertheless, some clear advantages are the fact that CTU is fast and nowadays widely available. It enables imaging of filling defects as well as parenchymal lesions in one examination. In case of malignancy, it also allows for clinical staging and, specifically in bladder tumors, for exclusion of upper tract involvement. The anatomic information provided by CTU may aid in decision making for a surgical approach. Furthermore, incidentalomas may be discovered in a timely fashion, which theoretically may result in better patient outcomes. On the other hand, it may also lead to unnecessary additional examinations or patient anxiety. Incidentalomas were discovered in 26.5% of scans of this study, and 14.4% of these were potentially life threatening.
The goal of investigations in patients with hematuria is twofold: To rule out malignant disease and to detect the source of the bleeding. Because of the trade-off between improved diagnostic accuracy and increased risk for adverse events, it is unclear for which patients CTU should be reserved. Because of the prospective nature of this research, the fact that CTU was part of a management algorithm and prospective readings were used for CTU results, this study provides valuable real-life data that may answer this question.
The diagnoses for the patients who presented with both microscopic and macroscopic hematuria in the current series are consistent with previous publications: In 8% to 17% of patients, malignancies are detected, in 8% to 30% benign causes, and in 52% to 82%, no abnormalities are found. 11 –16 The higher prevalence of malignant disease in patients who presented with gross hematuria, men, and patients above the age of 40 was also noted by other authors. 11,12,14,15 In the majority of patients, cross-sectional urography revealed no significant lesions. On analysis, only type of hematuria and results of ultrasonography (as performed by a urologist) were predictive factors for final CTU/MRU results. Although age is a commonly used factor in diagnostic decision making, the current study could not provide evidence for that. Because we looked for evidence of UUT disease overall, not only including malignancies but also stones (which can occur on any age), this may prohibit age from being a statistically significant predictor for finding UUT disease on CTU.
The ultrasonographic examination performed by our urologists had a relatively good capability of excluding UUT disease. Nevertheless, in 9.6% of patients with negative ultrasonographic examination, additional CTU revealed UUT disease. Table 6, however, shows that most lesions missed were stones and that although the majority of UUT tumors were not directly visualized, hydronephrosis was apparent, which would normally prompt further investigations. In addition, all patients with UUT tumors presented with macroscopic hematuria (in two with red efflux from the ipsilateral orifice at cystoscopy), which already induces a higher index of suspicion and a more extensive search for a diagnosis. The false-positive rate, however, was relatively high. It may be speculated that the diagnostic accuracy of an ultrasonographic examination would improve if performed by radiologists.
In a large proportion of patients who presented with macroscopic hematuria, no abnormalities were identified on CTU/MRU (81.9%), but this was even more prominent for microscopic hematuria (92.1%). Although 9 of 17 UUT lesions in patients with microscopic hematuria were missed with the first-line ultrasonography, none of them were malignant or needed active treatment. Thus, ultrasonography seems a reliable diagnostic tool for patients who present with microscopic hematuria.
The results of this study can also be evaluated in an exploratory way. If all patients who present with microscopic hematuria and a negative ultrasonographic examination (performed by a urologist) as a first-line test would not have had an additional CTU, no significant lesions would have been missed (8 stones and 1 small angiomylipoma). Then, for 196 of 525 patients, the risks associated with CTU and healthcare costs would have been avoided. Therefore, based on the data of the current study, we would propose the following management algorithm for UUT imaging for patients who present with hematuria: For macroscopic hematuria, a CTU should be performed (or MRU in selected cases with renal insufficiency or iodine contrast allergy), based on the higher likelihood of detecting significant disease. For patients with microscopic hematuria, ultrasonography should be performed as initial assessment. If results of this ultrasonography are positive, findings need to be confirmed with CTU. If results are negative, the patient can be followed and in case of persistent microscopic hematuria (eg, after 6 months as defined by the American Urological Association guidelines 2 ) in combination with risk factors for significant disease, cross-sectional UUT imaging has to be reconsidered. The Dutch Association of Urology has recently adopted an update of their hematuria guideline that underlines the above proposed diagnostic management algorithm. 8 Whether a CTU should consist of four phases as in the current study protocol or fewer phases (using a split-bolus or triple-bolus technique that decreases radiation exposure) 9,17,18 is yet unknown. Because of the low prevalence of renal and UUT tumors in the current series, an analysis on the diagnostic value of each individual phase of the four-phase CTUs performed in this study will be inconclusive and was therefore not performed. Future protocols might include risk-tailored cross-sectional investigations as proposed by the European Society of Urogenital Radiology. This group stated that for high-risk cases, the increased radiation risk seems balanced against the need for detection or exclusion of significant disease. For low-risk cases, the group proposed to use CTU as a problem-solving approach, with risk-tailored protocols (either one- or two-phase scans). 9
This study has several possible limitations that need to be addressed. First, the accuracy of ultrasonography is highly investigator dependent. Although radiologists are specialized in ultrasonographic imaging, this diagnostic tool is also frequently used by urologists. The reason we chose to have the initial ultrasonography performed by a urologist instead of a radiologist is mainly because of logistics. Second, although we did advise the general practitioner to repeat urinalysis after 3 months in the case of negative examinations, we did not collect data on follow-up. Hence, there is a possibility of yet unidentified false-negative results. Nevertheless, recent studies have shown that the likelihood of detecting significant disease after negative initial evaluation is rather low in patients with microscopic hematuria (risk <1%). 19,20 For macroscopic hematuria, this likelihood is slightly higher (up to 5%). 19 It must be noted, however, that in the referred study, initial evaluation consisted of IVU, which is known to have a lower diagnostic accuracy than CTU, as used in the current protocol.
Third, the number of patients in the current population with microscopic hematuria from nephrologic disease is unknown. Although we did perform microscopic urinalysis if indicated, results of this examination were not recorded in the database because this was beyond the scope of our study. We do want to stress that it is of utmost importance to look for signs of nephrologic causes of hematuria. This includes microscopic urinalysis that allows detection of proteinuria, casts, or dysmorphic erythrocytes. Also, blood pressure and kidney function should be estimated with creatinine serum analysis or preferably glomerular filtration rate.
Fourth, in the analysis of possible predictive factors for findings on CTU/MRU, we did not include cytology results, although this does seem to make sense. 21 We decided to do so, because in the current hematuria clinic protocol, we solely used bladder washout specimens for cytology, which do not provide information on the UUT.
Conclusion
In most patients (86.1%), cross-sectional urography revealed no significant UUT lesions. Only type of hematuria and results of ultrasonography were predictive factors for final CTU/MRU results. For patients who present with microscopic hematuria, ultrasonography is sufficient to exclude significant UUT disease. For patients who present with macroscopic hematuria, the likelihood of finding significant UUT disease is higher, and a CTU as a first-line test seems justified.
Footnotes
Disclosure Statement
No competing financial interests exist.