
Abstract
Laparoscopy has become an effective modality for the treatment of many pediatric urologic conditions that need both extirpative and reconstructive techniques. Laparoscopic procedures for urologic diseases in children, such as pyeloplasty, orchiopexy, nephrectomy, and bladder augmentation, have proven to be safe and effective with outcomes comparable to those of open techniques. Given the steep learning curve and technical difficulty of laparoscopic surgery, robot-assisted laparoscopic surgery (RAS) is increasingly being adopted in pediatric patients worldwide. Anything that can be performed laparoscopically in adults can be extended into pediatric practice with minor technical refinements. We review the role of laparoscopic and RAS in pediatric urology and provide technical considerations necessary to perform minimally invasive surgery successfully.
Introduction
The ability to treat children effectively in a minimally invasive fashion has been fueled by improvements in instrumentation, robotics, and the creativity of minimally invasive surgeons. Laparoscopic surgery has gained widespread acceptance given the reliability and durability of outcomes. The numerous benefits of laparoscopic surgery over the standard open approach include better cosmesis, increased magnification improving visualization, reduced postoperative pain, and shorter hospital stays. 2 Laparoscopic pyeloplasty, orchiopexy, nephrectomy, renal cyst decortication, pyelolithotomy, ureteral reimplantation, and bladder augmentation have all been performed safely and effectively with outcomes at least comparable to those of open techniques. 3 –6
The technical difficulty and steep learning curve of laparoscopic surgery has contributed to the growing popularity of robot-assisted surgery (RAS). The da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) provides the advantages of simplification and precision of exposure and suturing because of allowing movements of the robotic arm in real time with increased degree of freedom and magnified three-dimensional (3-D) view. 7 RAS has the potential to make laparoscopic surgery more accessible to pediatric urologists and simplify complex upper-tract and reconstructive procedures. 8 –10 RAS, initially used for pyeloplasty 11 and nephrectomy, 12 can be used to perform ureteral reimplantation 13 and more complex reconstructive surgeries including bladder augmentation 14 and antegrade continence enema. 15
One disadvantage of conventional pediatric laparoscopy and RAS is the need for multiple incisions that are significant in size with relation to patient size. 16,17 Single-incision laparoscopic surgery (SILS) may be advantageous in children, but experience with these novel techniques remains in its infancy. We review the current role of laparoscopic, RAS, and SILS in pediatric urology and provide a technical guide to minimally invasive pediatric urologic surgery using laparoscopic and single-port techniques, with and without robotic assistance, and a critical summary of the current literature, including surgical indications and outcome.
Technical Considerations in Pediatric Patients
Anesthesia
Laparoscopy has generally been well tolerated in children. Important anatomic and physiologic characteristics of children as opposed to adults include high chest wall compliance, diaphragmatic respiration, and rate dependent cardiac output because of reduced ventricular compliance. With creation of a pneumoperitoneum, decreased respiratory compliance and increased airway pressures create concern for oxygen desaturation. 18 To assess the impact of pneumoperitoneum on cardiopulmonary function, Halachmi and associates 19 retrospectively reviewed the impact of extraperitoneal vs intraperitoneal CO2 insufflation in 62 patients. They reported that despite physiologic changes in respiratory rate, peak airway pressures, and end tidal CO2, there were negligible changes in heart rate and oxygen saturation.
Size of the child
The smaller size of children presents a smaller working environment than found in adults after establishment of pneumoperitoneum. While an adult pneumoperitoneum will typically provide a 5 L to 6 L working space, a 1-year-old boy will present a 1 L intra-abdominal space. 20 Further, the limited “real estate” and small working distance on the abdominal wall in a child can significantly limit the mobility of the laparoscopic and robotic instruments, and the chance of port site conflicts or trocar head piece collisions is greater. A difference of a few millimeters can greatly affect the safety of the operation, making the location and placement of the robotic trocars critical in children and necessitating slight variations compared with placement in adults. The diminished thickness of the abdominal wall, especially in infants, makes maintenance of insufflation during instrument exchange challenging. Anchoring the trocar to the abdominal wall with a heavy suture will keep the abdominal wall in place if rapid desufflation should occur. 21
Pressure tolerance and abdominal wall compliance
Children are considered more sensitive to pressure in the peritoneal working space than adults with a greater chance of developing crepitance and dissection of insufflations gas. 22 The current norms used for working pressure in infants (0–2 y), children (2–10 y), and adolescents (>10 y) are 8 to 10 mm Hg, 10 to 12 mm Hg, and 15 mm Hg, respectively. The abdominal wall of children, however, has less resistance (or greater compliance), so there is little change in the working space afforded by increasing the pressure beyond these levels. The highly compliant pediatric abdomen also provides less resistance, making trocar placement more difficult and increasing the risk for injury to other intra-abdominal structures. An increase in pressure to 20 mm Hg will not increase the working space, but it does increase the resistance of the wall to deformation, easing safe trocar insertion. The more compliant abdomen of the infant, toddler, and preschool child may require more “curved” triangular configuration of ports to maximize exposure and ergonomics.
Foley/gastric decompression
Because of the more abdominal position of the bladder in infants, a Foley or straight catheter should be placed before access in all infants to reduce the possibility of inadvertent bladder injury. Placement during pelvic procedures, while not mandatory, is recommended to aid visualization of pelvic structures. Given the greater incidence of aerophagia and inflation of the stomach with air during induction of anesthesia in children, tube decompression of the stomach should be considered in all children.
General Techniques and Considerations: Peritoneal Access
Open access
Typically during RAS, an open access technique (Hasson) is used for the 12-mm camera port in which an incision is made in an open fashion and carried down to expose the peritoneum, which is then opened sharply under direct vision. The camera port is typically placed in the superior aspect of the umbilicus. Initial peritoneal access under direct vision is considered safer in children given their reduced anterior-posterior diameter and hence closer proximity to the great vessels.
Veress access
A needle with a spring-loaded “safety” insert is placed through the rectus fascia at the umbilicus. Two separate “pops” should be felt when traversing the rectus sheath and peritoneum. Aspiration with no withdrawal of blood or fecal matter and maintenance of a low pressure (<10 mm Hg) on insufflation of CO2 confirms needle placement in the peritoneum. Most significant complications that are associated with closed access techniques are related to placement of the trocar, not the Veress needle.
Direct access
This technique typically uses optical visualization or special bladeless trocars during initial trocar placement. The trocar is placed directly through the abdominal wall, absent underlying insufflation. With a 0-degree lens placed through the obturator of the trocar, the abdominal wall is observed directly as the port transits the wall. This approach is championed by several experienced gynecology groups that report no major vascular injuries with direct access and bowel injury rates that do not differ from other methods. They argue that the use of a single blind step is preferable to two blind steps in Veress access; however, their success may be related to the lower tone of the parous female abdominal wall that comprises the bulk of the patients addressed by these surgeons.
Off midline visual trocar access is a variant of direct access and has become popular in the hands of a number of general surgical and urologic laparoscopists. This method uses various optical trocars, such as a VisiPort (USSC, Norwalk, CT) or OptiView (Ethicon, Cincinnati, OH), which allow the tissue beneath the end of the trocar to be seen. An incision is made in the skin overlying the rectus muscle, and the trocar is inserted. The muscle is observed as the trocar advances, and the port is advanced to a position just beyond the rectus before insufflation. When initial access is placed lateral to the rectus muscle, the location of the port is followed through the orientation and layer number of the muscle fibers. At the lateral border of the rectus, all three muscle layers (external oblique, internal oblique, and transversus abdominis) may not be present. Familiarity with the ordination of the abdominal muscles and a thorough understanding of anatomic variations likely to be encountered is crucial during access. Briefly, the external oblique course from a superolateral to inferomedial position, internal oblique from inferolateral to medial, and transversus abdominis lateral to medial. Advocates for direct access purport that the advantages of both Veress and Hasson access are obtained in terms of time and safety.
Although the overall risk of major vascular injury during access is low, large multicenter analyses of complications associated with laparoscopy revealed a substantial reduction in the incidence of major vascular injuries with open access. 23 The risk of bowel injury, however, was higher in patients undergoing open access. In a single institution analysis of more than 800 pediatric urologic laparoscopic procedures, there was no significant difference in access-related complications between open and Veress needle access (0.8% vs 2.3%, respectively). 24 Both open and minimally invasive peritoneal access techniques suffer from occasional inadvertent preperitoneal access, but the frequency of access-related injuries has decreased with both time and operator experience. Experience matters, because surgeons who perform more than 12 laparoscopic procedures annually had lower complication rates compared with surgeons who performed laparoscopy less frequently. 24
General Issues
Complications
Contemporary series of adult laparoscopic procedures report complication rates ranging from 12% to 16%. 25,26 but there are few such studies that examine laparoscopic complications in the pediatric population. In a review of 5400 laparoscopic cases performed by 153 pediatric urologists, Peters 27 reported an overall complication rate of 5.4%. When excluding misdirected insufflation, however, the incidence of complications decreased to 1.2%, of which 0.4% necessitated additional surgical intervention. Peters also concluded that the greatest predictor of complication rate was operator laparoscopic experience. This study affirms that laparoscopic procedures in children are safe with minimal mortality and a low rate of complications.
Port and instrument sizes
Particularly in both children and infants, it is preferable to limit the size of the trocar/sheath. At present, complete instrumentation (dissectors, scissors, grasping retractors, needle drivers, and bipolar instrumentation) are available in 2-, 3-, 5-, and 10-mm formats. Clip appliers need at least a 5-mm port, and stapling devices, automated suturing devices, and preloaded entrapment sacs need at least 10-mm access.
Need for specimen extraction may mandate an incision of a certain size, suggesting at least one port of similar size. For instance, while a nephrectomy can be accomplished using solely 3-mm instrumentation, even a diminutive multicystic dysplastic kidney cannot be removed through a 3-mm port site (incision will have to be enlarged before specimen removal). Optics vary, because 2-mm and some 3-mm telescopes use fused bundle fiberoptics that produce pixilated images with reduced resolution and that may be a distraction to the surgeon (50,000 pixel lenses are functional for most dissections, although may need an electronic filter and adaptation for the surgeon). Many 3-mm and current 5- and 10-mm optics use rod lens systems that provide excellent clarity and brightness. In almost all applications, there is no significant loss with the use of 5-mm rather than 10-mm optics. Some limitations of reduced format lenses, such as the ability to throw light over a more distant field, are simply not at issue when the working space is smaller.
Access methods are also impacted, because open access cannot practically be achieved through an incision less than 1 cm; at least a 5-mm port is usually placed at the access site. The use of optical trocars, particularly for retroperitoneal access, may need a 10-mm port. Instrument rigidity also directs port size. While 5- and 10-mm instruments are effectively rigid rods, 3-mm and 2-mm instruments flex to varying degrees based on manufacturer, length, and instrument type. The 2-mm instruments need acclimation to their flexibility while 3-mm instruments are sufficiently rigid to prove immediately functional to most surgeons. With experience, the flexibility of 2-mm instruments can provide a surrogate of tactile feedback in much the same way a fishing rod does.
Several instrument types work optimally in specific sizes. For example, 3-mm Babcock graspers do not consistently provide positive grip in handling bowel, while the 5-mm size is optimal for securely grasping and handling the ureter without crush damage. Right angle dissectors improve with increasing format size, providing greater jaw excursion and ability to envelop and pass behind structures. A size less than 5 mm is significantly compromised for dissection of all but the smallest of structures. The jaw design of 5-mm clip appliers uses expansion beyond the 5-mm shaft diameter, prohibiting insertion or removal of loaded clips.
Costs
While laparoscopic surgical procedures are often criticized for higher costs, attention to selection of reusable over disposable instruments can substantially reduce costs. 28 Time can be a significant factor in the cost of laparoscopy; procedures in evolution and inexperienced operators and support staff can considerably increase operative time. Teaching institutions often magnify these time differences as residents adapt to a new environment. Finally, it is often easy to stray from the task at hand and “take in the sights” at an additional cost in terms of time (checking abdominal contents is seldom part of an open orchiopexy). In evaluation of any report concerning a cost analysis where time represents a significant factor, some consideration should be given to the overall experience of the operators and support staff and their location on the learning curve. Finally, authors should differentiate between costs and charges and clearly state whether estimates are modeled.
Working spaces
Two working environments are available: Laparoscopic, in which the working space is the peritoneal cavity, and retroperitoneoscopic. The laparoscopic or transperitoneal approach provides a larger working space, familiar anatomic landmarks, typically requires retraction of the intestines, and is a “tried and true” method to perform minimally invasive surgery. Limitations include the need to traverse the peritoneum, and a higher incidence of port-site–associated complications, such as enteric fistula and hernia. The retroperitoneoscopic approach allows a smaller working space, avoids intestinal retraction and violation of the peritoneal cavity, and lessens port-site complications. Many urologists, however, will find the anatomy and landmarks unfamiliar, resulting in a lower acceptance of this untraditional approach.
The admonition to avoid violation of the peritoneum is based on open surgical experience. While greater numbers of intraperitoneal adhesions are found in open transabdominal procedures, laparoscopic intra-abdominal procedures show minimal increased adhesion risk. 29 –32 The “elimination” of risk of injury to intra-abdominal structures is highly unfounded—the peritoneum does not defend against electrocautery. Partitioning an open urinary system from the peritoneum may afford some advantages; however, this has not been demonstrated in the modern surgical era.
Indications, Procedures, and Outcomes in Pediatric Urology
Orchiopexy
Indication
Laparoscopy remains the most accurate diagnostic tool for evaluation of a nonpalpable testis. Differential diagnosis includes undescended testis, testicular agenesis, vanishing testis, intra-abdominal testis (nubbin or normal), and intracanalicular testis (Fig. 1). Laparoscopy allows both diagnostic and therapeutic modalities, and laparoscopic orchiopexy has becomes the therapeutic procedure of choice in boys with undescended testes. 33,34 Overall outcomes are excellent, with reported success rates after laparoscopic orchiopexy ranging from 85% to 96%. 35
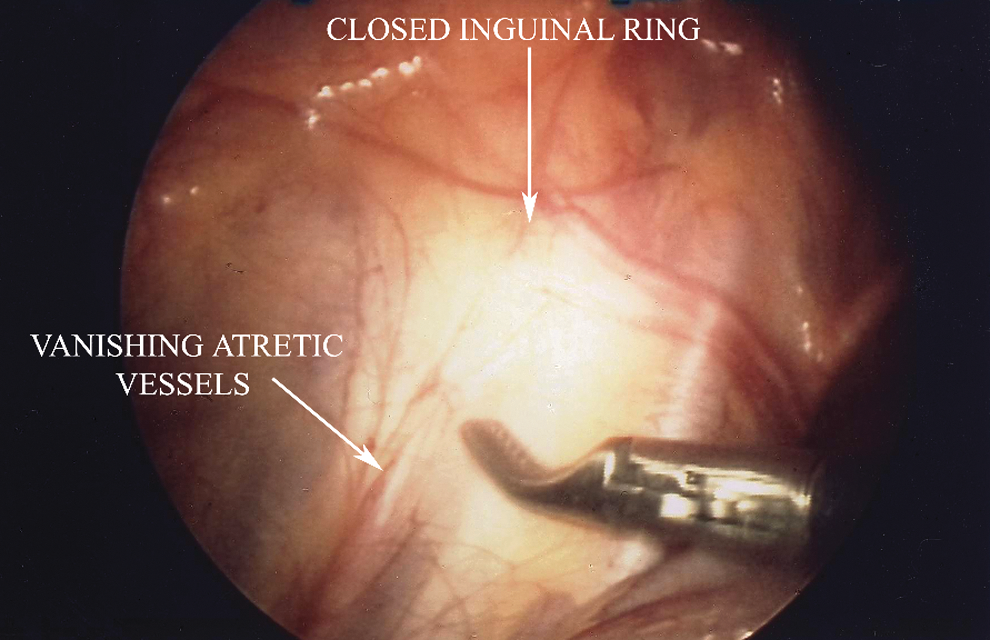
Diagnostic laparoscopy performed for a nonpalpable left testicle revealed a closed internal inguinal ring and vanishing atretic vessels. Testis can safely be deemed absent.
Surgical technique
Laparoscopic orchiopexy provides the advantage of being able to treat whatever pathology is encountered immediately after diagnosis. The patient is placed supine in the Trendelenburg position with elevation of the operative side. We routinely empty the bladder to prevent inadvertent injury and improve visualization. Port placement is similar for both conventional and robot-assisted laparoscopy, with a supraumbilical camera port and two working ports, one ipsilateral in the midupper abdominal quadrant lateral to the rectus and the other contralateral in the midlower abdominal quadrant lateral to the rectus; both ports are approximately in the midclavicular line.
Primary orchiopexy and mobilization of the testis into the scrotum can be performed for testes located within 2.5 cm of the internal inguinal ring, while Fowler-Stephens or staged orchiopexy, necessitating ligation of the spermatic vessels, can be used for more cephalad testes. The staged approach may be entertained in any abdominal testis worthy of salvage as long as there is union of the vas and testis and the vas is not short. We have not found the robot to be useful for orchiopexy, because reconstruction is not part of the procedure.
Outcome
A multi-institutional analysis of laparoscopic orchiopexy for the management of intra-abdominal testes revealed success rates higher than that historically ascribed to open orchiopexy. 3 Also, single-stage Fowler-Stephens laparoscopic orchiopexy resulted in a significantly higher atrophy rate than the two-stage repair. When considering both approaches, however, the laparoscopic approach gave greater success than previously reported for the same open approaches. 3 Others have demonstrated no significant difference between single and staged Fowler-Stephens orchiopexy with respect to intrascrotal testis viability at 6 month follow-up, 4 while others have shown that two-stage Fowler-Stephens is preferable. 36 Laparoscopic orchiopexy is the procedure of choice in the approach to the impalpable undescended testicle. 3,5
Nephrectomy
Indication
Indications for nephrectomy include a nonfunctioning or poorly functioning kidney secondary to ueteropelvic junction (UPJ) obstruction or recurrent urinary tract infection (UTI), vesicoureteral reflux nephropathy, calculi, malignancy, multicystic dysplastic kidney, and pediatric kidney recipients. 37 –39 The single-system ectopic ureter with incontinence in young females can be diagnosed and treated laparoscopically.
Surgical technique
Although the increased dexterity and 3-D visualization provided by the robot can be advantageous for beginners, 40 the technology is somewhat overkill for a simple nephrectomy. Laparoscopic renal surgery can be performed through a transperitoneal or retroperitoneal approach, but the transperitoneal approach is more readily accessible in infants, given the smaller abdominal surface area that may have the result of instrument clashing if the robot is used. In the transperitoneal approach, the patient is placed in a modified flank position with 30-degree to 60-degree elevation of the ipsilateral flank. An umbilical camera port is placed, and working ports are placed in the midline beneath the xiphoid process and lateral to the umbilicus (paramedian) at the anterior axillary line on the ipsilateral side of the pathologic site.
If the robot is being used, ports are placed in the umbilicus for the camera port, and the working ports are placed midline above the umbilicus and midclavicular line below the umbilicus. In infants, the lateral port should be placed as far lateral to the rectus muscle as possible. The robot is then docked over the ipsilateral shoulder. 21 The kidney is exposed by freeing medially at the lower pole to begin exposure of the hilum, and anterolateral traction on the ureter will provide better hilum exposure. After ligation of the hilar vessels, the ureter should be taken with electrocautery or an Endoloop device for nonrefluxing and refluxing units, respectively.
The retroperitoneal approach can be used dependent on surgeon preference and experience and may be influenced by the need for additional procedures such as nephroureterectomy and bladder access if reimplantation is needed. For the retroperitoneal approach, the patient is placed in full flank position, and ports are placed in the midaxillary line midway between the tip of the 12th rib and iliac crest (camera), and working ports just lateral to the psoas muscle below the 12th rib, and medial anteroinferior to the initial port. A balloon can be used for initial dissection of the retroperitoneal space. Similar to a transperitoneal approach, subsequent identification and upward traction on the ipsilateral ureter assists in identifying hilar structures. Lateral traction of the kidney puts the hilum on stretch for dissection and visualization, and the renal artery is evident more clearly given its posterior location. Anterior dissection of the kidney results in the kidney falling onto the hilum and should be avoided before transection of the vessels. The size of the robotic arms makes a posterior approach more difficult except in children older than 12 years.
Prone retroperitoneoscopic nephrectomy
The patient is positioned prone and secured, with support at iliac crests and axillae, being sure not to limit forward fall of the abdomen. VisiPort access is obtained at the costovertebral angle inferior to the 12th rib and lateral to the sacrospinalis muscle. Once retroperitoneal fat is seen, the scope should be oriented toward the psoas muscle (this is “up”), pointing to the pelvis. Balloon dilation of the retroperitoneum can be used for initial dissection if desired (5 minutes for minor vessel tamponade). After increasing pressure to 15 mm Hg, 2- to 5-mm working ports are placed 1- to 2-cm above the iliac crest lateral to the sacrospinalis and another port 1- to 2-cm above the iliac crest at the posterior axillary line.
Care should be taken to avoid transgression of the peritoneum, which has been actively reflected as far anteriorly as possible. Dissection should begin anterior to the lower port, freeing the lower pole of the kidney, then moving superiorly to free the kidney posteriorly. The ureter is located by dissecting medially from the lower pole, and then followed superiorly to the renal hilum. After ligation of the renal vessels, the ureter is dissected distally as is appropriate, and ligated.
Outcome
While robot-assisted nephrectomy is possible in children, it is cost-prohibitive, and there is little information available in the literature regarding its use. 41 The safety and efficacy of laparoscopic nephrectomy for benign disease in children, however, has been firmly established. 42 –45 The need to convert to open renal surgery is very low in published series (Table 1). In experienced hands, a transperitoneal or retroperitoneal approach has comparable operative times. The benefits of laparoscopy may be less apparent in infants given their rapid convalescence after any surgical approach. Comparative studies of open vs laparoscopic nephrectomy typically demonstrate increased operative times and shorter hospital stay with laparoscopy (Table 1).
OR=operative; LOS=length of stay; RP=retroperitoneal; RN=radical nephrectomy; TP:=transperitoneal; RNU=radical nephroureterectomy; ARF=acute renal failure.
Partial nephrectomy (heminephroureterectomy)
Indication
Partial nephrectomy can be used in the management of renal duplication anomalies, such as a nonfunctioning upper (or lower) pole segment with ureterocele or ectopic ureter, cystic malformation of the upper pole kidney, and a nonfunctioning refluxing lower pole kidney. 46 Surgical management consists of identification of the upper and lower pole vessels and ureter. Children with a duplication anomaly will have a clear vascular and anatomic plane between the upper and lower pole kidney. Once the structures are sorted to upper or lower pole, division of the vessels to the dysfunctional segment, and division of the renal cortex along the line of demarcation identified after ligation of the associated vessels is performed.
Surgical technique
The procedure follows the same approach as a nephrectomy with regard to port placement and initial exposure of the ureters and hilum. The identification of upper and lower pole renal segments and their vascular supply is critical. A harmonic scalpel is an excellent device to divide the parenchyma while avoiding hemorrhage. Robotic assistance can also be used via a transperitoneal or retroperitoneal approach. The procedure is performed as described for the laparoscopic approach with similar port placement. We prefer the transperitoneal approach because of the size of the robotic arms and ports. Also, the transperitoneal approach allows easy access to the bladder if needed. Prior to patient positioning, we place an open-ended ureteral catheter in the unaffected moiety. This allows injection of methylene blue after transection of the affected moiety to assess for leakage. Typically, a bladder catheter is left in place overnight, and the patient is discharged to home on postoperative day 1.
Outcome
Lee and colleagues 46 successfully completed robot-assisted heminephroureterectomy in nine children with a mean operative time of 275 minutes and an estimated blood loss of 49 mL. They reported only one complication—an asymptomatic urinoma—and all children had a normal remaining renal moiety. The retroperitoneal robot-assisted approach has also been reported in 14 children with a median operative time of 176 min; 2 children needed conversion to an open operation. 47
Pyeloplasty
Indication
The natural history and the need for surgical repair of a hydronephrotic system with apparent elevated resistance at the UPJ are in evolution. The ultimate fate of patients with UPJ obstruction and the means to separate those in need of repair from those destined to avoid ill effects are currently under study. The most clearly accepted current criteria for intervention is loss of function of more than one third from the affected kidney (asymmetric renal function with less than 35% to 40% of function in the affected side given a normal contralateral kidney). 48 Increasing hydronephrosis, massive hydronephrosis, symptomatic obstruction, pyelonephritis, poor parental acceptance, and contralateral renal disease are also relative indications.
Surgical technique
Laparoscopic pyeloplasty is typically approached in a transperitoneal fashion to afford a larger working environment for intracorporeal suturing. A stent is typically placed, and this can be performed cystoscopically at the start of the procedure or after the UPJ is opened. This procedure at present is ideally suited for children >20 kg because of working space limitations. The patient is positioned either supine with a 30-degree wedge or in full flank position. Ports are placed at the umbilicus, subcostally in the midclavicular line, and near the midaxillary line lateral to the rectus at the level of the anterior superior iliac spine. In many children, access to the renal pelvis can be obtained through a mesenteric window; this obviates the need to reflect the colon.
The dissection begins at the lower pole to expose the hilum and identify the ureter and any crossing lower pole vessel. Two additional 5-mm working ports can be placed in the anterior to midaxillary line for additional retraction as needed. A hitch stitch is placed in the renal pelvis to lift and secure the pelvis toward the midpoint of the lower two ports. The renal pelvis is then opened superior to the UPJ, and the incision extended to the most dependent position, followed by spatulation of the ureter. A single suture is placed in the crotch of the ureter spatulation to the dependent portion of the pelvis and tied. The back wall is sutured with a running stitch, and tied at the superior apex. We typically use 6-0 monofilament absorbable suture. The UPJ area is excised removing the “handle,” and the anterior wall is then closed in a running fashion. A drain may be place if desired, although we infrequently use drains.
Robotic modifications
A trans- or retroperitoneal approach can be used. The patient is placed in the same position and robotic docking is performed in the same fashion as for nephrectomy. The UPJ is exposed transmesenterically on the left or by colonic mobilization on the right. The surgical procedure is performed in the same way as described for the conventional laparoscopic approach. We use a hitch stitch if a pyelolithotomy is necessary. The ureter is typically spatulated laterally, and the anastomosis is performed using a running suture (Fig. 2). A double pigtail stent is placed after closure of the posterior wall. A guidewire is placed antegrade via an 18-gauge angiocatheter through the anterior abdominal wall, and the stent is placed over the guidewire. Filling the bladder with saline or methylene blue will allow visualization of urine efflux once the stent reaches the bladder. A urethral catheter is left in place overnight, and the Double-J ureteral stent is removed in 2 to 4 weeks.

Intraoperative view of posterior anastomotic suture placement during stentless transmesenteric robot-assisted laparoscopic pyeloplasty.
Outcome
When comparing the gold standard open approach with the laparoscopic approach, the mean operative time is shorter in the open group, but children undergoing laparoscopic surgery use fewer analgesics and leave the hospital faster. 49 The success rate of laparoscopic pyeloplasty is approaching that of conventional open pyeloplasty. 50 –56 The major disadvantage of the laparoscopic approach is the high proficiency needed for intracorporeal suturing, leading to increased surgical times. Robot-assisted laparoscopic pyeloplasty (RALP) facilitates intracorporeal suturing and decreases the learning curve for minimally invasive surgery. 57
Success rates with robotic assistance are approximately 95%, 58 –63 approaching success rates of the open approach. Two reports compared an age-matched cohort undergoing open pyeloplasty with RALP, and all robotic procedures were successful as determined by pain scales and radiologic data. 61,62 A retrospective case-control study of 66 patients undergoing either open or RALP showed similar success rates. 61 Finally, while smaller working spaces may limit robotic performance in laparoscopy, 64 RALP can also be safely performed in infants 3 to 8 months old (Table 2). 65
OR=operative; LOS=length of stay; TP=transperitoneal; RP=retroperitoneal; NR=not reported; ACE=antegrade continence enema.
Ureteral reimplantation
Indication
The management of vesicoureteral reflux (VUR) has changed greatly over the last 25 years, and current strategy attempts to curtail upper tract infection through the use of suppressive antibiotics while awaiting spontaneous resolution of VUR. Surgical correction is considered appropriate for persistent or recurrent pyelonephritis despite prophylactic antibiotics, failure of spontaneous VUR resolution, worsening reflux, or parental selection of surgical management. The goals of surgical management are prevention of pyelonephritis, renal scarring, and functional loss. The goal of surgery directed at the prevention of VUR is to enhance compression and luminal occlusion of the ureter against the muscular backing of the detrusor during voiding.
Surgical technique, extravesical approach
The procedure is identical to an extravesical detrusorrhaphy (Lich-Gregoir); a trough is made in the bladder, the ureter placed in the trough, and the detrusor closed over the ureter. The patient is positioned supine with legs spread to allow Foley catheter placement on the field. Ports are placed in the umbilicus and bilateral midlower abdomen lateral to the rectus muscle, to 2 cm above the pubic symphysis. After identification of the course of the ureter into the pelvis, the peritoneum over the ureter is incised just distal to the vas deferens (in females: above the broad ligament lateral to the uterus). The ureter is dissected free from the surrounding tissue, keeping its vessels intact and followed distally to the trigone. The pelvic plexus is readily identified medial and caudal to the ureter. Approximately 4 to 5 cm is dissected to permit mobility and to prevent kinking as the bladder tunnel is created for the ureter. The bladder is inflated and deflated under vision to identify the course of the ureter. A hitch stitch can be placed through the posterior bladder wall to improve the exposure of the ureteral hiatus if the bladder is large.
A detrusor trough is created by incising the muscularis of the bladder for about 3 cm and developing flaps with the cautery scissors. Mucosa perforations are closed using absorbable 5-0 suture before trough closure. The bladder muscularis is then closed over the ureter, using a 4-0 absorbable interrupted suture. Care must be taken to avoid any kinking or excessive compression of the ureter to prevent obstruction. Closure is performed proximal to distal. We catch the adventitia of the ureter with each suture to ensure it does not slip back during the healing process. The urethral catheter is removed the next morning, and the child is discharged after voiding.
Robotic modifications
Positioning is the same as for the laparoscopic approach. A ureteral catheter is placed on the affected side at the beginning of the case and secured to the urethral catheter. Ureteral catheters are used as a safety mechanism to allow visualization if the ureteral integrity is disrupted. The robotic camera port is placed via an umbilical trocar; two working ports are placed each lateral to the rectus muscle at the level of the anterosuperior iliac spine (Fig. 3).
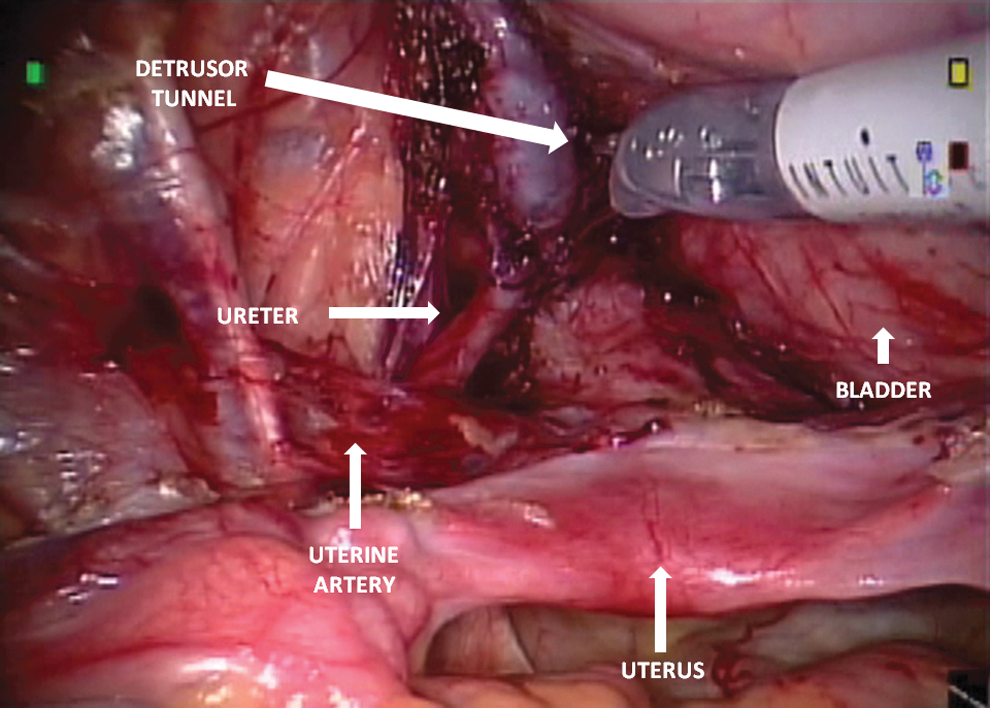
Creation of detrusor tunnel for extravesical ureteral reimplants. Dissection should be kept distal to the uterine artery. Detrusor tunnel is approximately 4 to 5 cm.
Outcome
Open extravesical ureteral reimplantation is an effective method to repair VUR without ureteral obstruction, but it carries an undesired high rate of transient postoperative urinary retention. 66 Robot-assisted laparoscopic extravesical reimplantation has reported success rates as high as 97.6% without the occurrence of urinary retention or significant complications. 67 The improved visualization provided by the robot helps avoid injury to the neurovascular plexus.
Surgical technique, laparoscopic transvesical approach
The pure laparoscopic approach uses a Cohen transvesical crosstrigonal ureteral reimplanation technique. Its limitations have been described, and we do not advocate the approach in bladders less than 130 mL. The patient is placed in the dorsal lithotomy position, and trocars are placed under cystoscopic guidance as described by Yeung and coworkers. 68 Two 3-mm trocars are used for the working ports, and a 5-mm trocar is used for the midline camera port housing a 0-degree 5-mm telescope. Typical insufflation pressures are between 7 and 8 mm Hg with high flow rates between 12 and 15 mL/min. After the trocars are inserted, an 8F pediatric feeding tube is left in place through the urethra and connected to a suctioning device that can be clamped and unclamped when suctioning is necessary. Excisional ureteral tapering is performed with a running 6-0 absorbable suture if difficulty is encountered when tunneling the dilated ureter.
Robotic modifications
Patient positioning is the same as for the laparoscopic approach. The bladder is filled with saline solution through the urethra. Using an open technique or visualization via a flexible pediatric cystoscope, the 12-mm camera port is placed in the midline at the bladder dome. A 3-0 absorbable suture secures the bladder wall and skin to the trocar. The working ports, either 8 or 5 mm, are positioned midway between the umbilicus and pubis at the midclavicular line. Ports are fixed to the abdominal wall using a stitch that is also used to close the bladder. The bladder is filled with CO2 to drain the saline, and the robotic device is brought over the patient's feet.
Similar to the open technique, ureteral dissection starts after placement of a 6-cm segment of a 5F feeding tube or 4F open-ended ureteral catheter, secured to the ureter with a 4-0 absorbable suture. Mobilization of the ureters is performed as in the laparoscopic pneumovesical procedure using the hook or scissor cautery. The submucosal tunnels are created by dissecting with scissors from the original hiatus to the other side of the trigone and incising the mucosa at the site of the new mucosal hiatus. Anastomosis of the ureters is performed after bringing them through the mucosal tunnel. Anchoring 4-0 absorbable sutures are used to secure the ureter to the bladder musculature, and the mucosal cuff is attached with 5-0 absorbable suture. The mucosa over the original hiatus is closed with running 5-0 absorbable suture. The working ports are removed and the bladder holding stitches are then tied. The flexible cystoscope is used to inspect the inside of the bladder, and the port sites are also closed at the fascial level. The bladder catheter is kept overnight.
Outcome
There are few reports of this approach using conventional laparoscopy 68 and only one using robotic assistance. 69 Recently Valla and associates 70 reported a mean operative time of 82 minutes with a 92% success rate and a 6% conversion rate in 72 patients undergoing transvesicoscopic Cohen reimplant. Peters and colleagues 69 reported five cases of robot-assisted transvesical cross-trigonal reimplantation. Maintaining pneumovesicum is difficult, however, and small capacity bladders are difficult to navigate. This technique provides excellent visualization and control, although it is extremely challenging.
Appendicovesicostomy
Indication
Bladder outlet obstruction and dysfunction caused by neurogenic bladder, nonneurogenic bladder, posterior urethral valves, and the complex, often lead to urinary incontinence and renal dysfunction in children. Although some of these children can be treated medically or with minimally invasive intervention, in most of them, augmentation cystoplasty with a continent catheterizable channel, usually appendicovesicostomy, is the standard of care.
Surgical technique
Traditionally, the Mitrofanoff procedure is performed through an open incision. With the recent development in laparoscopic techniques and robotics, a minimally invasive approach to this surgery can be considered and may result in diminished postoperative pain, a shorter hospital stay, and improved cosmesis. 71 Robotic technology greatly facilitates laparoscopic appendicovesicostomy. The patient is placed in the modified lithotomy position, and three ports are used: A 12-mm camera port in the umbilicus and the other two 8-mm ports on the right and left sides, in the midclavicular line at the level of the anterior superior iliac spines.
The appendix is mobilized using the appendicular/cecal junction while maintaining the appendiceal mesentery and assuring an adequate length of appendix. After complete cecum mobilization, the appendix is separated from the cecum, leaving a small cuff of appendix with the cecum. 2 The bladder is filled with saline, and the best position for the appendix is determined based on its length, stoma location, and bladder mobility. A 4-cm detrusorrhaphy is made, and the appendix is anastomosed to a small mucosal opening in the apex of the detrusor trough; the defect is closed using 4-0 absorbable interrupted suture (Fig. 4). The base of the appendix is then brought up to reach the umbilicus or the right lower quadrant. A V-flap technique can be used to create a catheterizable stoma via the right lower quadrant trocar site.
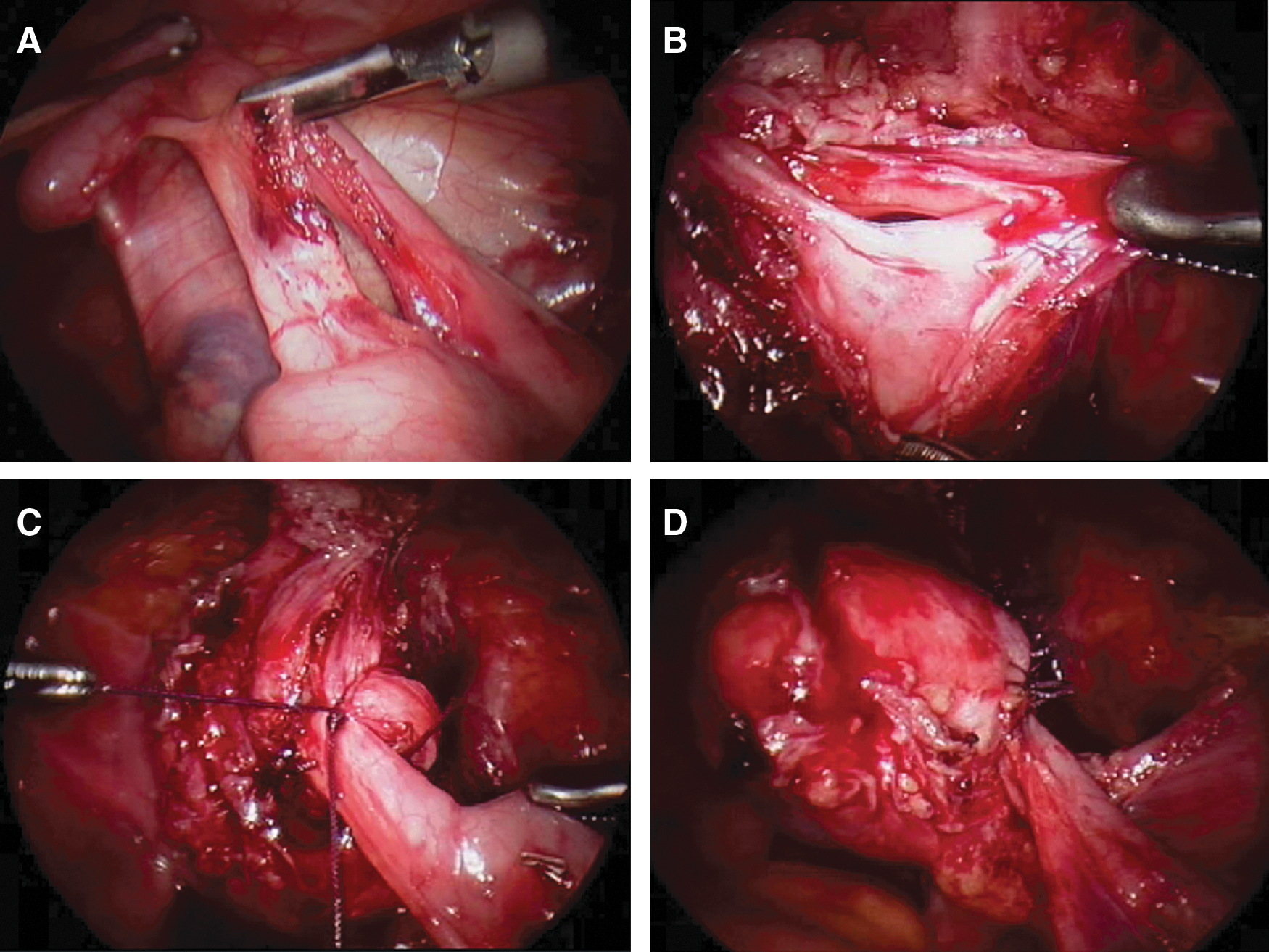
Robot-assisted laparoscopic appendicovesicostomy. The appendiceal mesentery is freed with sharp dissection and hook electrocautery at the base of the cecum, avoiding injury to the appendiceal artery
Outcome
Despite the high success and low complication rate of the open Mitrofanoff procedure, it remains a morbid operation necessitating an open abdominal incision associated with high success and low complication rates, respectively. 72 Nguyen and colleagues 71 presented their series of 10 patients undergoing robot-assisted laparoscopic Mitrofanoff appendicovesicostomy with satisfactory outcomes and minimal complications. There are also several case reports of appendicovesicostomy using a pure laparoscopic approach. 73 –75
There are several case reports of robot-assisted Mitrofanoff procedures in children. 76 –79 Laparoscopic Mitrofanoff has the potential to significantly lessen morbidity compared with the open approach. Robotic assistance provides wristed instruments that facilitate manipulation and suturing, enhanced vision providing depth perception, and a learning curve that is less steep. Robot-assisted laparoscopic appendicovesicostomy is an effective technique that remains in its infancy. Continued improvements and reporting by others are vital for continuing evolution of this technique.
Ureteroureterostomy
Indication
Laparoscopic upper-tract surgery remains extremely challenging in children. We consider laparoscopic or robot-assisted (RAUU) ureteroureterostomy for children with a duplicated collecting system and an upper pole ectopic ureter with function in that moiety. An upper-tract reconstructive approach is chosen depending on concomitant entities, such as lower pole reflux or the necessity of bladder neck reconstruction with ectopia. We have previously reported that robotic assistance greatly facilitates this technically challenging procedure.
Surgical technique
All patients undergo cystoscopic evaluation with retrograde ureteropyelography and open-ended ureteral catheter placement into the lower pole ureter. We maintain access to the ureteral catheter throughout the procedure and inject methylene blue dye as needed to assess the integrity of the anastomosis and collecting system. The ureteral catheter also secures access for indwelling stent placement after completion of the anastomosis. The transperitoneal robotic approach is similar to the approach described above for robotic extravesical reimplantation. The upper pole ectopic ureter is spatulated before transection, and reapproximation of the upper and lower pole ureters is performed with 6-0 absorbable sutures in a running fashion. In girls and boys, the distal ureteral segments are removed at the level of the vagina and prostate, respectively. We do not leave ureteral stumps when we perform this procedure via a laparoscopic transperitoneal approach because of the relative ease of access.
Outcome
We have previously demonstrated the safety and feasibility of RAUU in 15 patients. 2,80 RAUU has also been used successfully for the correction of ureteral obstruction in children with single and duplicated collecting systems. 81,82 Laparoscopic upper-tract reconstruction in children is a viable alternative to the open approach, but needs further investigation.
Laparoendoscopic Single-Site (LESS) Surgery or SILS
Although in its infancy, LESS surgery has the potential to minimize the number of incisions while maximizing intracorporeal access. The theoretical advantage of LESS surgery is that an entire procedure can be performed using an incision that would have been necessary for specimen removal in conventional laparoscopy. The umbilical location of the incision improves cosmesis; however, the advantages of LESS surgery compared with conventional laparoscopic surgery have yet to be proved. A limited number of case reports and small series have described the use of LESS surgery for pediatric urology procedures including nephrectomy, 83 –85 nephroureterectomy, 86 and pyeloplasty. 87,88
Access is obtained using an open technique by way of the umbilicus, and a single-port access device is deployed. Two commonly employed ports include the Olympus TriPort (Olympus, America, Melville, NY, and Advanced Surgical Concepts, Wicklow, Ireland) and the Covidien SILS port (Covidien, Norwalk, CT). The Olympus port includes an associated introducer, which allows for placement of the single port using a 10-15–mm umbilical incision. The SILS port can be placed through an incision as small as 15 mm, and it allows access for three 5-mm cannulas or two 5-mm cannulas and one 12-mm cannula. All ports are single-access multichannel laparoscopic ports. A combination of flexible forceps and scissors and conventional laparoscopic (straight) instruments can be used. Procedures are performed in similar fashion to that of conventional laparoscopy.
Outcome
Koh and coworkers 85 performed LESS nephrectomy in 11 children ranging from infants to adolescents and had similar perioperative parameters to those of a historical cohort. The mean operative time and hospital length of stay were 139 minutes and 1.5 days, respectively. Two of their procedures were performed in infants without complications. Complications included two patients with de novo unilateral ipsilateral hydroceles that were presumed to be secondary to a subclinical patent processus vaginalis. Other smaller series have reported similar results. 83,84.86 Successful completion of LESS nephroureterectomy has also been reported in 2 patients. 86
Successful completion of LESS pyeloplasty has been reported in one series of 11 patients. 87 Mean patient age was 10 years, and mean operative time and estimated blood loss were 182.5 minutes and 97.3 mL, respectively. Mean hospital stay was 2 days, and complications included a port site skin infection and UTI. The success rate was 100% when defined by symptom resolution and improvement of renal function and drainage of the affected kidney. Their early experience suggests improved cosmesis with comparable outcomes to conventional laparoscopic surgery. Additional studies are necessary, however, to determine whether a single umbilical incision in children is associated with improved operative outcomes, reduced pain medication requirements, shorter convalescence, and validated measures of postoperative cosmesis.
Footnotes
Disclosure Statement
No competing financial interests exist.