
Abstract
Purpose:
To present the results of our experience with combined endoureterotomy and endoscopic injection of dextranomer/hyaluronic acid (Deflux) for the treatment of primary obstructive refluxing megaureter (PORM).
Patients and Methods:
Eighteen children (12 female, 6 male; mean age–14 months) with 20 PORM units underwent concomitant endoureterotomy and endoscopic subureteral Deflux injection. All patients underwent endoureterotomy at the 6-o'clock position with insertion of a 3F Double-J ureteral stent into the obstructed segment of ureter and subureteral injection of Deflux at the 5-o'clock and 7-o'clock positions. The Double-J stent was left in place with its distal tip fixed with a single knot to the external genitalia for easy removal after 1 week. Patients with refluxing nonobstructive ureter on the contralateral side of the PORM unit (seven children) underwent simultaneous endoscopic subureteral injection of Deflux. Voiding cystourethrography (VCUG) was performed at 6 months, and ultrasonography was performed at 1 week 3, 6, and 12 months postoperatively.
Results:
With a mean follow-up of 30 months, the procedure was uneventful in all patients. Follow-up VCUG showed no evidence of reflux in 15 ureterorenal (75%), significant decrease in reflux grade in 2 (10%), and no change in 3 (15%) in the endoscopic treated PORM units. No evidence of reflux was observed in the treated contralateral refluxing nonobstructive ureters. Ultrasonography revealed no ureterovesical junction obstruction. In 19 ureterorenal (95%) units, there was a complete resolution or decrease in hydroureteronephrosis.
Conclusions:
The results of this study demonstrate that combined endoureterotomy and subureteral injection of Deflux is safe and effective in the treatment of PORM in selected patients.
Introduction
Diagnosis of the PORM is important because the treatment of the obstructive pattern differs from the reflexive pattern alone. The diagnosis is usually based on a dilated ureter, smooth tapering of the lower ureter, refluxing pattern on voiding cystourethrography (VCUG), and ruling out the infravesical or extrinsic obstructions. 4
During the past two decades, the management of primary megaureter has evolved to a conservative approach as the initial management, especially in the nonrefluxing megaureter. 5 The primary goals in the treatment of megaureters are to minimize the potential damage to the affected kidney, maximize the growth potential of the ipsilateral kidney, and prevent the formation of new renal scars resulting from infection and inflammation because of the ascension of bacteria-laden urine from the bladder to the kidney. 6 The decision to perform a surgical intervention is difficult, especially in infants. Very few series have reported the results of megaureter repair in pediatrics. Significant obstruction or breakthrough febrile infection and new pyelonephritic scars, however, are generally considered as indication for surgery and the termination of conservative management.
Tailoring and reimplantation are the most common surgical interventions performed for the correction of megaureter. This method usually needs a long ureteral length and resection of the lateral ureteral wall with a reported efficacy of 90% to 95%. There is a 5% to 25% reported complication rate for this technique. Folding modifications (Kalicinski) and Starr technique are two modifications that are introduced to decrease the damage to the ureteral vasculature. Despite the above-mentioned advantages of these modifications, the folded ureter is bulky and may make the reimplantation difficult. 7 Open surgery is usually associated with significant postoperative pain, long hospital stay, prolonged convalescence, and remaining unsightly scars.
Technical advances with improvement in endoscopic skills provide less invasive treatment alternatives for urologic open surgeries, but there are only a few reports of application of endourologic interventions for the management of megaureters in infants. Our previous report on endoureterotomy for primary obstructive megaureter was promising. 2 The present study reviewed our experience with combined endoureterotomy and endoscopic injection of dextranomer/hyaluronic acid (Deflux®) for the treatment of PORM with long-term follow-up.
Patients and Methods
Between November 2000 and November 2008, a total of 856 children with a diagnosis of dilating megaureter were referred to the children's Center of Excellence (the national referral center for pediatric urology) for surgical intervention. Of these, 378 children had a diagnosis of obstructive megaureter by ultrasonography before and after 3-hour free bladder drainage. 8 In this method, the ureteral diameter is measured using ultrasonography with a full and empty bladder; then an appropriate-sized urethral catheter is inserted into the bladder for free drainage and remains inside for 3 hours. Ultrasonography is repeated for reevaluating the degree of hydroureteronephrosis and ureteral diameter. The diagnosis of obstruction is reconfirmed by 99m-technetium diethylenetriaminepentaacetic acid (99mTc-DTPA) diuretic renography as the gold standard test for obstruction. Among these 378 patients, 24 children were consistent with the diagnosis of PORM after obtaining voiding VCUG. Among these, 6 were stable with conservative management and regular follow-up evaluation, but 18 children needed surgical intervention.
We retrospectively reviewed the medical records of these 18 patients who underwent endoscopic treatment for PORM in 20 ureterorenal units. Patient demographics are summarized in Table 1. The mode of presentation was prenatal or neonatal hydronephrosis in 12 patients, recurrent urinary tract infection (UTI) and urosepsis in 4, flank pain or mass in 1, and pyelonephritis in 1. Concurrent renal abnormalities included seven patients who had vesicoureteral reflux (VUR) in the contralateral ureters, and one patient with a kidney stone.
VUR=vesicoureteral reflux; PORM=primary obstructive refluxing megaureter.
As the first line of treatment, all children received conservative management with follow-up visits every 6 months. The decision to proceed to surgery was based on breakthrough febrile UTI, pyelonephritis, and symptoms such as flank pain or in asymptomatic patients, factors such as worsening of hydronephrosis, deterioration of renal function on DTPA scan, or new renal scars (Table 2). Exclusion criteria were ureteral dilation secondary to bladder or urethral pathology and <12 months of follow-up.
UTI=urinary tract infection.
No child had undergone any type of ureteral surgery. Preoperative diagnostic evaluation included serum biochemical analysis, urine analysis and culture, renal function tests, renal ultrasonography, VCUG to rule out urethral obstruction, renal 99mTc-DTPA scan, dimercapto-succinic acid (DMSA) scan, and MRI in selected cases. The International Reflux Study Classification was used to grade reflux on VCUG (1–5). 9 All patients had acceptable renal function on the obstructed side as assessed by radionuclide scan (>20%). In patients with UTI, the imaging study was postponed until the infection was under control.
Prophylactic antibiotic was administered after diagnosis. The study was approved by the local ethics committee, and a written informed consent was obtained from all children's caregivers. All procedures were performed under general anesthesia with the patient in the lithotomy position. Using a 6/7.5F pediatric cystoscope with an offset lens, the bladder was filled to half volume to permit direct visualization of the ureter.
After visualization of the bladder and ureteral orifice, a flexible guidewire was inserted into the ureter. The criteria for performing the modified technique were the presence of intravesical ureteral obstruction, a stricture length of <1.5 cm, and proportionally shorter cutoff points with regard to the individual ureteral length and age based on our previous experience in children with primary obstructive megaureter. 2 The ureterovesical junction was dilated by passing a 3F Double-J stent over the guidewire through the ureteral orifice. In cases with a narrow ureteral orifice, a 1F guidewire was advanced through the ureterovesical junction followed by the 3F Double-J stent. The distal tip of the Double-J stent was secured by a 5-zero polypropylene single suture to the external genitalia to facilitate stent removal without cystoscopy and induction of general anesthesia.
The 4.5/6F neonatal ureteroscope (Richard Wolf GmbH, Knittlingen, Germany) was then introduced up to the obstructed segment of the ureter, and a longitudinal intramural incision was made at the 6 o'clock position with pure cutting current using a 2F diathermy coagulation Bugbee electrode (Fig. 1). The incision was generated to the extent that the adipose tissue surrounding the bladder was visualized in a linear fashion. The bladder adventitia was kept intact to prevent urinoma formation.
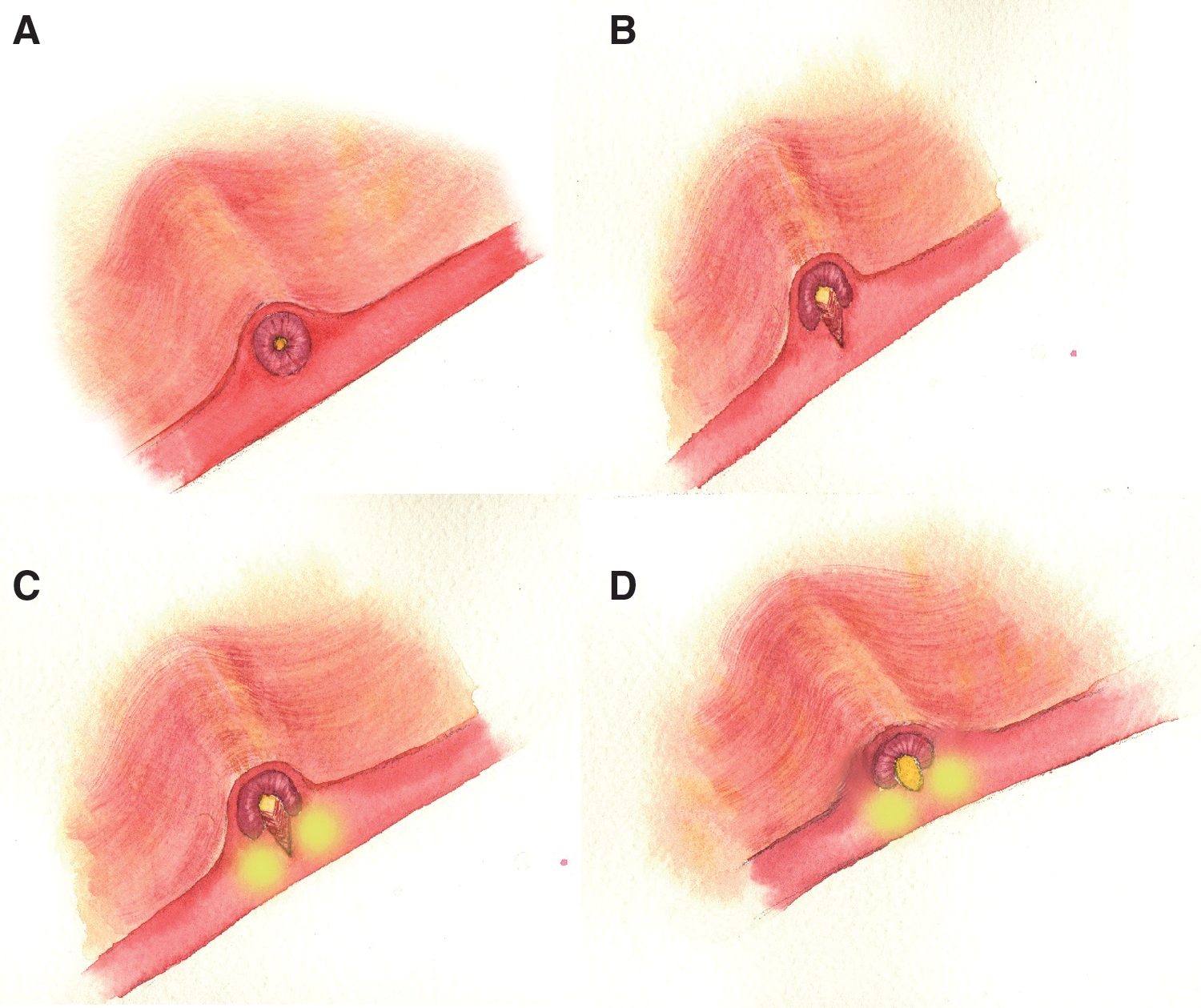
Schematic representation of endoureterotomy and endoscopic injection of Deflux.
After completion of endoureterotomy, a Storz cystoscopic injection needle consisting of a 10 mm long, 21 gauge, 3F needle connected to a 30 cm long plastic tube was advanced through the working channel of a miniature (6/7.5F) Wolf neonatal cystourethroscope. The needle tip was inserted at the 5 o'clock and 7 o'clock position, with the bevels facing laterally, into the subureteral space approximately 1 to 2 mm distal to the ureteral orifice and was advanced proximally. An average of 0.3 to 0.5 mL Deflux was injected slowly until a volcano bulge obliterated the ureteral orifice. The needle was kept in position for 2 minutes before it was withdrawn to minimize extravasation of injected material through the needle track. The guidewire was kept in place during the procedure to straighten up the curl during the incision and injection. Prophylactic antibiotics (third-generation cephalosporin preoperatively and first-generation cephalosporin postoperatively) were started and continued until removal of the Double-J stents after 1 week.
To assess outcome, follow-up VCUG was performed 3 months after injection. The antibiotic prophylaxis was resumed postoperatively until the VCUG showed no reflux at 3 months. Patients were evaluated with ultrasonography after 1, 3, and 6 months. A renal 99mTc-DTPA scan was performed after 6 months, and the follow-up for clinical symptoms was continued yearly with ultrasonography studies. The postoperative success rate was defined as no sign of obstruction on radiographic examinations, resolution of hydroureteronephrosis, reflux grade reduction, and improvement or maintenance of renal function on renal scan. Complications such as UTI and increase in VUR grade or new onset contralateral reflux were recorded.
Results
The overall operative time ranged from 23 to 54 minutes (mean time 37 min). The procedure was performed successfully in all patients, except one, whose procedure needed conversion to open surgery and who underwent tailoring and reimplantation because of the ureteral opening into the Hutch bladder diverticulum. This patient was included in the total failure rate. The blood loss was minimal, and the procedure provided excellent homeostasis that led to a clear field of view during the procedure. No intraoperative complication was noted. All 18 patients had a smooth postoperative period, with no morbidity. No postoperative complication, including ureteral obstruction, wound infection, or urinary leakage, was observed. No patient needed narcotic analgesics in the postoperative period, and patients were discharged after 1.1±0.5 days (mean±standard deviation [SD]) postoperatively (range 1–2 d).
The mean postoperative follow-up was 30 months (range 11–72 mos). The overall success rate (according to our definition) was 85% (17 of 20 ureterorenal units with PORM). In 75% of uretrorenal units, there was no evidence of reflux, and in the other 10%, there was a significant decrease in reflux grade on the follow-up VCUG (Fig. 2). The distribution of reflux grade and cure rate are shown in Table 3. Hydroureteronephrosis resolved completely in 45% of the ureterorenal units, and the other 50% showed a significant decrease in hydroureteronephrosis. Relative renal function was preserved in 88.9%, and there was a significant increase in two children (11.1%); worsening of renal function was not observed as assessed by serial plasma creatinine and urea assays or differential renal function on DTPA scan.

A 1-year-old girl with a history of recurrent urinary tract infection with left primary obstructive refluxing megaureter and contralateral reflux.
All patients underwent preoperative and postoperative renal scans to determine differential renal function. The median preoperative renal function in the affected kidney was 40.15%±8.09%. Follow-up renal scans performed at a mean of 21 months after surgery (range 8–72 mos) revealed a relative function of 41.25±7.62%. There was no significant difference between the preoperative and postoperative renal function based on renal scans. The T1/2 had been more than 100 minutes in five ureterorenal units preoperatively (mean±SD=66.15±30.02). Diuretic washout normalized in all ureterorenal units postoperatively (T1/2 <12 min). No evidence of reflux was observed in the treated contralateral refluxing nonobstructive ureters. No children experienced breakthrough UTI during the follow-up period, and flank pain resolved in the child with the preoperative history of flank pain and mass.
Discussion
With the new advances in endourologic techniques, endoscopic approaches have become the first line of management in most patients with urologic problems. 10 Our previous report on the value of endoureterotomy showed definite advantages of the endourologic approach over the conventional open surgical procedure. 2 We showed that endoureterotomy could be considered over open surgery as a temporizing alternative in selected patients. On the basis of the results of the previous study, we developed a new modified technique for the treatment of PORM. This technique combines the advantages of minimally invasive techniques and initial conservative management. This approach is the only one that avoids any incision in the skin, which reduces the hospital stay and decreases the postoperative pain along with no cosmetic sequelae.
PORM implies the simultaneous presence of obstruction with reflux. 1 The exact etiology of PORM is not fully understood. The obstruction at the distal part of the ureter is thought to be a functional obstruction arising from an immotile juxtavesical segment rather than a true narrowing. 11 Reflux is usually attributed to the architectural deficiencies in the intramural portion of the ureter.
The widespread use of ultrasonography during pregnancy has led to the detection of many asymptomatic neonates with megaureter. A large proportion of these dilated ureters tend to improve or resolve completely without any surgical intervention. 6
During the past two decades, the trend in the management of primary megaureters has evolved completely to an initially conservative approach that involves close clinical and radiographic evaluation along with antibiotic chemoprophylaxis. 4 Our approach to asymptomatic cases was initial conservative management that includes a complete history and physical examination, renal ultrasonography, VCUG, and renal 99mTc-DTPA scan. Follow-up radiographic assessments were performed every 6 months after the diagnosis. Keating and associates 12 noted that up to 13% of patients with primary megaureters could not be treated conservatively, and because the primary goal in the management of megaureter is to preserve the upper urinary tract function, they needed surgery.
The decision to proceed to surgical intervention in adolescents and adults includes impairment of renal function, breakthrough UTI, pyelonephritis, pain, worsening of hydronephrosis, and tense flank mass on physical examination. 2 The decision for operative treatment in the young infants and children younger than 1 year with severe hydroureteronephrosis is difficult, however. Few studies have reported the results of megaureter repair in this patient population. 13 Tailoring and reimplantation could be unfeasible because of the small bladder capacity in these patients. 7 As Defoor and colleagues 7 have noted, tailoring and implantation before the age of 1 year can potentially compromise the vascularity of the distal ureter and can result in further stricture.
In the present study, 50% of patients (n=9) were less than 1 year old who needed immediate surgical intervention because of the deterioration of renal function, and as mentioned earlier, the classic ureteroneocystostomy was not feasible. Our procedure avoids the abovementioned complications by minimizing the surgical trauma to the ureteral vessels and eliminating the need for a large working space in the presence of small bladder capacity.
Once surgical intervention is indicated, ureteroneocystostomy with ureteral reimplantation after resection of the obstructed segment and tapering of the dilated ureter is the most common procedure. 14 –16 Ureteral tailoring is usually indicated to satisfy the 5:1 ratio of tunnel length to ureteral diameter recommended by Paquin, which can be performed through a folding or excisional technique. The complications of these two methods are well known and range from 4% to 25% in different series. 14 So, the plication and the folding methods were developed. One of the disadvantages of the plication method, however, is the bulkiness of the plicated ureter that necessitates a larger and wider tunnel. In addition, this technique may have a stricture risk, because of the compression by the folded wall on ureteral vessels and, finally, the plicated ureter can go through fibrosis. Hence, Parrot and coworkers 17 reported to avoid folding of ureters larger than 1.75 cm.
In addition, the conventional open surgeries are associated with significant postoperative pain and morbidity, long hospital stay, high degree of invasiveness, aesthetic sequelae, and high cost. Accordingly, avoidance of conventional open surgeries as the first-line of treatment is no longer a subject of continuous debate. 2 Our favorable results of endoureterotomy for treatment of congenital obstructive megaureter and the good success rate of endoureterotomy in the management of subtotal ureteral strictures encourage us to apply a modified endoscopic technique for the treatment of congenital obstructive refluxing megaureters. Surprisingly, the success rate with this modified technique is high, although there is no study that has reported the success rate of open surgery in the treatment of PORM. Besides the hospital stay, postoperative pain and cost are reduced prominently compared with conventional open surgery.
Despite the high success rate with this new approach, one may argue that this was achieved in a highly selected proportion of children. With the application of this procedure, the ureteral vessels are usually kept intact, which is the main concern with open surgeries. With the introduction of a 6-o'clock intramural incision, the detrusor muscle bulks prevent the urine reflux after the surgery and avoid the unroofing of the ureter that is associated with incisions on the 12-o'clock position. By applying the ureteral incision at 6 o'clock, we had no new onset VUR on postoperative VCUG. With the injection of Deflux at the 5-o'clock and 7-o'clock positions, the buttress that is formed beside the incision site helps coapt the distal end of the ureter. The accuracy of the injection site is an important component for the success of this procedure.
In the present study, a ureteral stent was left in place for 1 to 2 weeks to prevent the immediate ureteral obstruction by edema and facilitate urothelialization and healing of the muscular layer. As Kerbl colleagues 18 have noted, with the 1-week stent period, sufficient urothelialization will occur. Davis and associates 19 discussed, however, that muscular regrowth will occur after 6 weeks. Consequently, the stent duration is currently a matter of debate. Because long-term stent placement may result in inflammation that leads to scar formation, no stent was kept in place for more than 1 to 2 weeks.
Van Cangh and coworkers 20 have noted that secondary causes may have a negative impact on the success rate of endopyelotomy; therefore, this procedure may not be promising in secondary megaureters.
Because most of our patients received a diagnosis prenatally and underwent regular evaluations after birth, all patients have an acceptable renal function that might have contributed to the high success rate of our study. The obstruction length was an important factor that had a reverse effect on the success rate of endoureterotomy in our previous study; therefore, we established a 1.5 cm cutoff for the maximum obstruction length in this study that might have added to the success rate. A shorter cutoff was used for younger children based on the individual ureter length.
To the best of our knowledge, this is the first series of combined endoureterotomy and endoscopic injection of Deflux for the treatment of patients with PORM. In properly chosen cases, this method could be feasible with an acceptable success rate. The authors think that this success may be because of the minimally invasive nature of this procedure and less surgical trauma to the ureteral vessels. Despite the favorable outcomes of this technique, we acknowledge the limitations of our study, including the retrospective design with no control group and the short-term follow-up of this series. One may argue that according to the literature, some failure of Deflux injection occurs after 6 months postoperatively; in this series, all patients underwent VCUG at 6 months, so further long-term randomized trials are needed to recommend this method. Health-related quality of life assessment, as well as hospital stay, is also necessary to accurately evaluate the advantages of this new technique.
Conclusion
These results suggest that combined endoureterotomy and endoscopic injection of Deflux is a safe, effective, and minimally invasive technique for the treatment of patients with PORM. It enables the urologists to manage obstructive refluxing megaureters with a minimally invasive approach before converting to more invasive procedures. Lower rates of hospitalization in comparison with open surgery are remarkable in this procedure. In the hands of a veteran surgeon, it is a safe and feasible procedure. It offers patients with severe hydroureteronephrosis the opportunity to avoid the highly invasive experience of open surgery. Further controlled studies in pediatric patients are needed, however, to accurately assess the effectiveness of this approach in comparison with its open counterparts.
Footnotes
Acknowledgment
We highly appreciate Mr. Majid Kajbafzadeh at the Simon Fraser University in Vancouver, Canada, for his final invaluable linguistic revision of the manuscript and Mrs. Bita Ahmadi, who provided great assistance in preparing the schematic pictures of the surgery. Illustration by Bita Ahmadi (bita_ahmadi77@yahoo.com).
Disclosure Statement
No competing financial interests exist.