
Abstract
Background and Purpose:
Efforts to improve postprostatectomy incontinence have led to many modifications in surgical technique. We present our experience with a novel technique to improve continence outcomes in patients who are undergoing robot-assisted radical prostatectomy (RARP).
Patients and Methods:
A consecutive series of 159 patients after initiation of a bladder neck plication stitch was compared with the most recent group before the change. After completion of the vesicourethral anastomosis, a single suture was used to plicate the distal bladder neck. A structured questionnaire was used for follow-up. Continence criteria used were 1 pad per day for social continence and 0 pad per day for total continence.
Results:
A total of 334 patients were included in the study: 159 in the plication stitch group vs 175 in the control group. Average age was 59.1 vs 59.6 years, average body mass index was 27.9 vs 28.3 kg/m2, and average prostate volume was 58.1 vs 60.9 cc, respectively. The mean time to reach social continence was 3.63±3.01 vs 5.33±4.89 weeks (P=0.004), and total continence was 5.10±3.80 vs 8.49±6.32 weeks (P=0.002), respectively. Chance of total continence improved with the bladder plication stitch: Odds ratio of 1.95±0.72 (P<0.001) at 1 month, 1.25±0.56 (P=0.113) at 3 months, and 2.07±0.66 (P=0.005) at 12 months. There were no bladder neck contractures or other urinary complications noted in either group.
Conclusions:
The bladder plication stitch is a simple and effective technical modification for shortening the period of recovery of urinary continence in RARP patients. Randomized controlled trials are under way to further evaluate this technique.
Introduction
In the long term, RARP has been shown to have continence rates of >90% in several large, single-center prospective studies, 1 –3 but the literature shows that the time to return to early postoperative continence varies with technical modifications. Such modifications include posterior rhabdosphincter reconstruction, 4,5 modifications in apical dissection, 6 anatomic bladder neck preservation. 7 total reconstruction of the vesicourethral junction, 3,8 seminal vesicle sparing techniques, 9 and puboprostatic ligament sparing. 10,11 There are also nonsurgical adjuncts that may affect a patient's functional outcome, such as pelvic floor muscle exercise therapy. 12 While many techniques have been evaluated, not all options have been exhausted.
The concept of the bladder plication stitch was derived from the intussusception stitch technique of Walsh and Marschke 13 introduced in open radical prostatectomy to improve postoperative recovery of incontinence. After 3 months, patients with the stitch had a significant improvement in return of urinary control. 13
This is a retrospective study of consecutive patients of our experience with a novel robot-assisted bladder neck plication technique. Our primary objective was to evaluate the efficacy of a bladder neck plication stitch in achieving early postoperative continence in comparison with the standard “no stitch” technique in patients undergoing RARP.
Patients and Methods
This study was performed under an Institutional Review Board-approved protocol. Adult subjects who have been diagnosed with prostate cancer and who choose RARP as treatment for their prostate cancer were included in the study. Inclusion criteria were patients with a new diagnosis of prostate cancer who were undergoing RARP for prostate cancer treatment without any previous urethral or continence surgery, urethral trauma, or previous radiation to the pelvis or abdomen. A consecutive series of patients after initiation of the use of the plication stitch (n=159) was compared with the most recent group before the change (n=175). No other changes in technique were performed. A single surgeon with more than 1500 RARP experiences performed the entire anastomosis and plication stitch. The patients were blinded to this change in surgical technique.
All anastomoses begin with a Rocco technique of posterior reconstruction of the Denonvilliers fascia, 4,5 , followed by Van Velthoven stitch 14 using a running, double-armed 3-0 poliglecaprone suture. After completing this vesicourethral anastomosis, we use a 3-0 Maxon™ (Covidien, Mansfield, MA) single suture to plicate the bladder neck in a figure-of-8 fashion (Figs. 1, 2). The first bite of suture is taken at about the 3 o'clock position about 2 cm proximal to the edge of the bladder neck or anastomosis. A similar small bite is taken on the 9 o'clock position. This process is repeated 5 mm more proximal on the bladder neck. The suture is then tied down directly on top to create the plication akin to a Nissen fundoplication. This plication of the bladder neck creates a funnel configuration such that the distal bladder neck remains relatively narrow during bladder filling. We plicate the bladder neck to a size where the inflated 10-mL Foley balloon will not retract to the anastomosis if pulled on.

Bladder plication stitch illustration. The anterior bladder plication stitch is positioned 2 cm proximal to the vesicourethral (V-U) anastomosis at 3 o'clock and 9 o'clock. When tied securely, this creates funneling of the distal bladder neck.
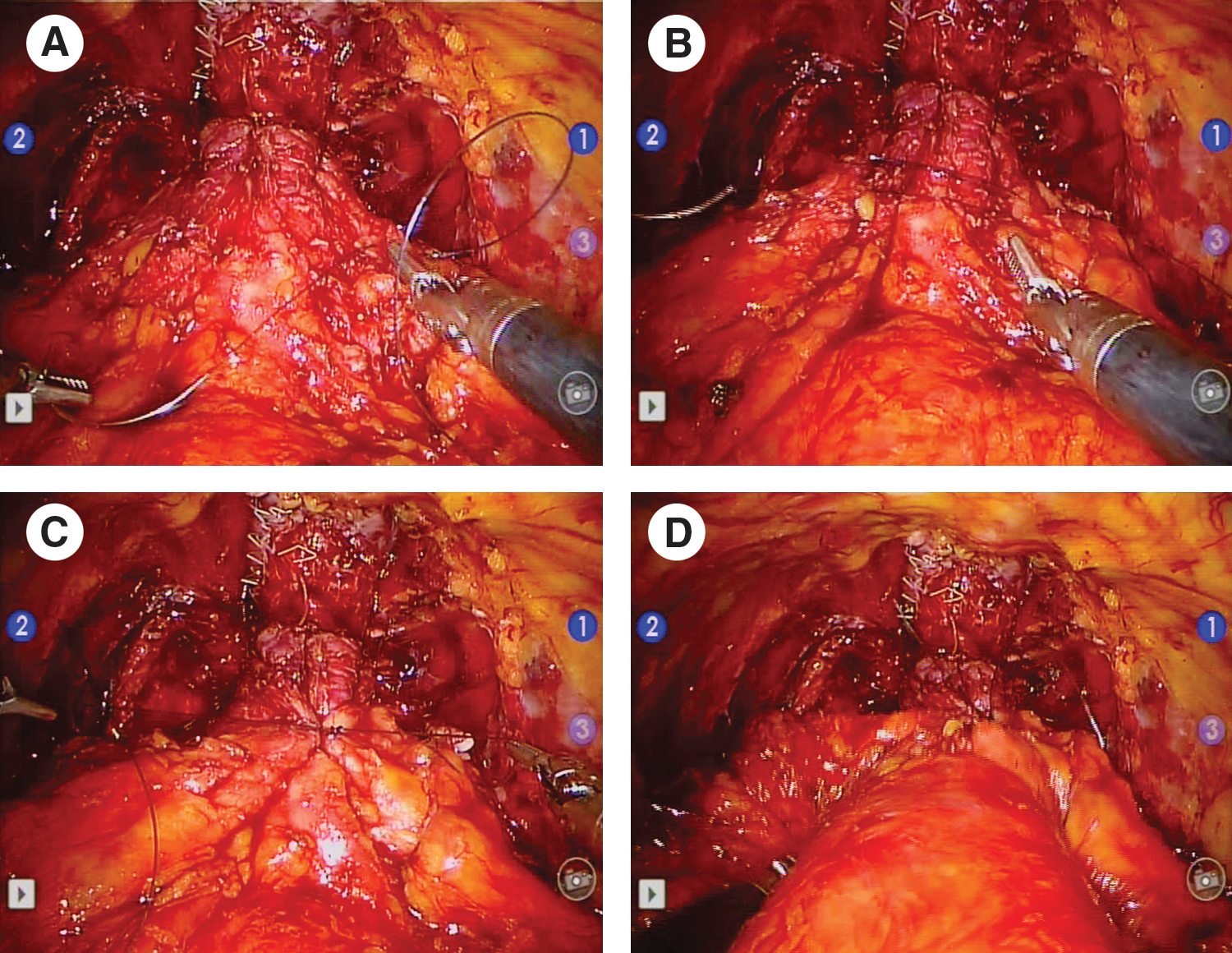
Bladder plication stitch intraoperative views.
Our primary outcome variables were time to reach continence, defined as zero pads per day (PPD), and time to reach social continence, defined as one PPD or use of a security pad. Follow-up visits were scheduled at 1 month, 3 months, and 12 months postoperatively, with any other visits scheduled if prostate-specific antigen level concerns arose or at the patient's discretion. At the start of each visit, the patient was asked to complete the structured questionnaire, which included pad use at the current time point and when he reached social/total continence, if recalled. Patient-specific parameters also analyzed included age, body mass index (BMI), and prostate size.
Data were compared using unpaired t tests, one way analysis of variance, odds ratio testing, and chi-square test for categorical variables to determine any significant difference between the two groups with respect to reaching early continence. Two-tailed two-proportioned z-tests were used between outcome percentages. A P<0.05 was considered statistically significant.
Results
A total of 334 patients were included in the study: 159 in the plication stitch group vs 175 in the control group (Table 1). The average age was 59.1 vs 59.6 years, the average BMI was 27.9 vs 28.3 kg/m2, and the average prostate volume was 60.94 vs 58.12 cc, respectively. Mean preoperative American Urological Association symptom score for both groups was 6.71, with a range from 5 to 33. There was no statistical difference between the two groups for any preoperative parameter. Final survey response rates at 12 months were 69.15% (n=121) for the no stitch group and 74.84% (n=119) for the bladder neck plication group (P=0.3).
BMI=body mass index; AUA=American Urological Association.
With the bladder plication stitch, 16% of patients were totally continent at 1 month vs 8.9% in the control group (P=0.097). Total continence was 36.3% vs 31.3% at 3 months (P=0.63) and 85.7% vs 74.4% at 12 months (P=0.042) for the bladder plication and control groups, respectively. Social continence was 44.3% vs 40.8% at 1 month (P=0.48), 72.6% vs 73.9% at 3 months (P=0.94), and 95.8% vs 95.9% at 12 months (P=0.77), for the bladder plication and control groups, respectively.
Odds ratio testing with chi square values for all time points (Table 2) showed that total continence at both 1 month and 12 months was significantly higher using the bladder plication stitch with odds ratio of 1.95±0.72 (P<0.001) and 2.07±0.66 (P=0.005), respectively. No significant differences were found in social continence at any time point.
Furthermore, the mean time to reach social continence was 3.63±3.01 vs 5.33±4.89 weeks (P=0.0036) for the plication and no plication groups, respectively (Table 3). The mean time to reach total continence was 5.10±3.80 vs 8.49±6.32 weeks (P=0.0021), respectively. There were no bladder neck contractures in either group. No other urinary complications were noted. The stitch was easy to perform and typically took no more than 2 minutes to complete.
PPD=pads per day.
Discussion
Walsh and Marschke 13 in 2002 described buttressing sutures used to intussuscept the bladder neck to achieve earlier continence recovery after radical retropubic prostatectomy (RRP). These sutures decrease the tension on the bladder neck as the bladder fills. Their technique begins with a 2-0 Maxon suture placed on the edges of the posterior bladder wall mainly in the adipose tissue, where the bladder was previously attached to the prostate, approximately 2 cm from the reconstructed bladder neck. The suture is then tied in the midline. The next suture is a figure-of-eight 2-0 Maxon placed 2 cm lateral to the bladder neck on each side. At this point, the bladder neck should protrude beneath the anterior hood of tissue created by the anterior stitch, similar to a turtle head outside its shell. After installation of saline, the bladder neck should be competent with very little leakage.
In a comparative study, Wille and associates 15 reported that intussusceptions of the bladder neck during RRP resulted in a significantly greater continence rate of 77% vs 60% at 3 months postoperatively, although the continence rates at 12 months were not significantly affected. In addition, overall urinary symptoms were significantly better in the intussusception group compared with control.
Our plication stitch was conceived to be similar to that described by Walsh and Marschke. 13 We found, however, that it was technically difficult to recreate this stitch robotically because the posterior bladder neck stitch is difficult to perform. Thus, we began by performing only an anterior stitch after the anastomosis is performed. We think that this likely acts in a different mechanism to help with continence than the Walsh stitch. The bladder neck becomes more funneled in appearance, similar to a Nissen fundoplication, and therefore probably decreases the amount of stretch on the bladder neck and urinary sphincter at rest. It is also possible this funneling acts to lengthen the functional length of the urethra.
In our retrospective study, patient outcomes did show statistically significant earlier improvement in both social and total urinary continence for those with the plication stitch during RARP. Because of our practice patterns, follow-up of our post-RARP patients was focused on oncologic follow-up, with typical visits scheduled at 1, 3, and 12 months after surgery. Consequently, determining the exact timing of return to continence was not ideal for all patients. Using our questionnaire, the precise return to continence date was only captured for 57% of all patients with respect to social continence and 27% of all patients with respect to total continence. A large component can be explained by the 22.5% and 46.5% of patients who achieved social and total continence, respectively, between the 3- and 12-month visits but many of whom were unable to recall at what precise time this continence had been regained. Our claim that the bladder plication stitch improves continence is also supported by pad use at those follow-up visits. The bladder plication stitch doubled the chance of total continence at both 1 month and 12 months. With an 86% response rate at 1 month, the odds ratio was 1.95±0.72 (P<0.001). Similarly, with a 72% overall response rate at 12 months, the odds ratio was 2.07±0.66 (P=0.005).
Notably, the stitch's simplicity and ease of its application poses little challenge during surgery and should be easy to learn and reproduce by most robotic surgeons. There has been concern raised about the Walsh intussusception stitch causing a slightly increased risk of bladder neck contractures. We did not identify any bladder neck contractures or stricture complications in either arm of the 334 patients of this bladder plication study.
While our bladder plication data support our expectations for RARP and correspond to existing literature for RRP, a randomized study is needed to verify these results. Although promising, the current study is limited because it is retrospective and nonrandomized. Before the initiation of the plication stitch, the previous 175 patients in the database were used as the subjects for the no-stitch group and the subsequent 159 patients formed the bladder plication stitch group. The strength of the study is that it is a single surgeon performing all plication stitches with no other changes in technique; the difference in surgical experience between each group is unavoidable and inherent for the application of any novel procedure. This primary surgeon, however, had already performed more than 1500 cases at the time of this study and thus it is unlikely that progression along the learning curve accounted for the difference in the results.
Conclusions
The bladder plication stitch is a simple and effective technical modification for improving recovery of urinary continence in RARP patients. The stitch is simple and quick to perform. No complications were noted. A randomized trial is under way to further evaluate this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.