
Abstract
Introduction:
Surgical morbidity and mortality rates are high in patients with Cushing's syndrome. Nevertheless, simultaneous bilateral laparoscopic adrenalectomy (LA) is feasible in these patients with less morbidity and good long-term results.
Background and Results:
Consecutive 22 patients who underwent LA for Cushing's syndrome between 2003 and 2010 in our institute were retrospectively studied. Ninteen patients underwent bilateral simultaneous and three underwent unilateral LA. Seven patients had Cushing's syndrome after failed pituitary surgery and five each had ectopic adrenocorticotrophic hormone dependent syndrome and bilateral macronodular hyperplasia respectively. LA was bilaterally done by lateral transabdominal adrenalectomy in 15 patients and retroperitoneal endoscopic adrenalectomy in 4 on the right side. Mean operative time for simultaneous bilateral cases was 199.45±72.43 minutes with mean blood loss of 72.72±48.6 mL. Patients were fit for discharge by the fifth postoperative day from the surgical aspect. Surgical complication rate was 26% that included wound infections in two, port site hernia, pleural effusion, and atelectasis in one each. One patient died of sepsis (5% mortality). Satisfactory metabolic control was achieved in all observable patients in the long term although Addisonian crisis and Nelson syndrome were seen in 26% and 15% respectively.
Conclusion:
LA has all advantages of minimal access surgery in patients with Cushing's syndrome who are immunocompromised and at high risk of delayed wound healing and infections. Magnification decreases the risk of retained adrenal remnants. Despite advances in minimal access surgery, perioperative morbidity continues to be significant for the procedure.
Introduction
Introduction of laparoscopy has revolutionized the approach to adrenal surgeries. Operative morbidity is considerably low in laparoscopic adrenalectomy (LA) compared with open adrenalectomy (OA). Simultaneous LA is a feasible and an effective therapeutic option in patients after failed pituitary surgery or when the ACTH source cannot be localized or ablated in patients with ectopic ACTH syndrome. 5 –9
Patients and Methods
A retrospective study of all consecutive LA done at our institute from May 2003 to January 2011 was done. Patient demographics, operative parameters, and postoperative events were assessed. Follow-up ranged from 6 to 73 months. The resolution of sequelae from Cushing's syndrome, the number and frequency of Addisonian crisis and Nelson syndrome, and current corticosteroid replacement needs were evaluated.
Preoperative assessment was done with urinary and serum cortisol followed by low dose and high dose dexamethasone suppression tests in all patients with confirmed endogenous Cushing's syndrome. Imaging was done with contrast enhanced computerized tomographic scan of chest, abdomen, and pelvis along with MRI of brain. Intravenous or oral hydrocortisone replacement was started perioperatively and continued postoperatively. All patients received prophylaxis for deep vein thrombosis (DVT).
Surgeries were performed in lateral decubitus. Usually, three ports were placed on the left side and four on the right in lateral transperitoneal adrenalectomy (LTA) and three ports for right retroperitoneal endoscopic adrenalectomy (REA) (Fig. 1). In all cases of simultaneous bilateral surgeries, the left side was done first followed by the right side after repositioning and redraping the patient. Harmonic scalpel was primarily used for dissection and prominent adrenal vein(s) used to be severed between surgical clips. The mobilized adrenal glands were trapped in Endobag for removal, and before termination of the procedure, the retroperitoneal beds were examined for completeness of gland removal. Patients were discharged on replacement steroids with oral prednisolone for all, and fludrocortisone in a few. Postoperative assessment was done with stress Synachtan test after stopping the replacement steroid for 24 hours. Undetectable serum cortisol levels confirmed absence of adrenal tissue.
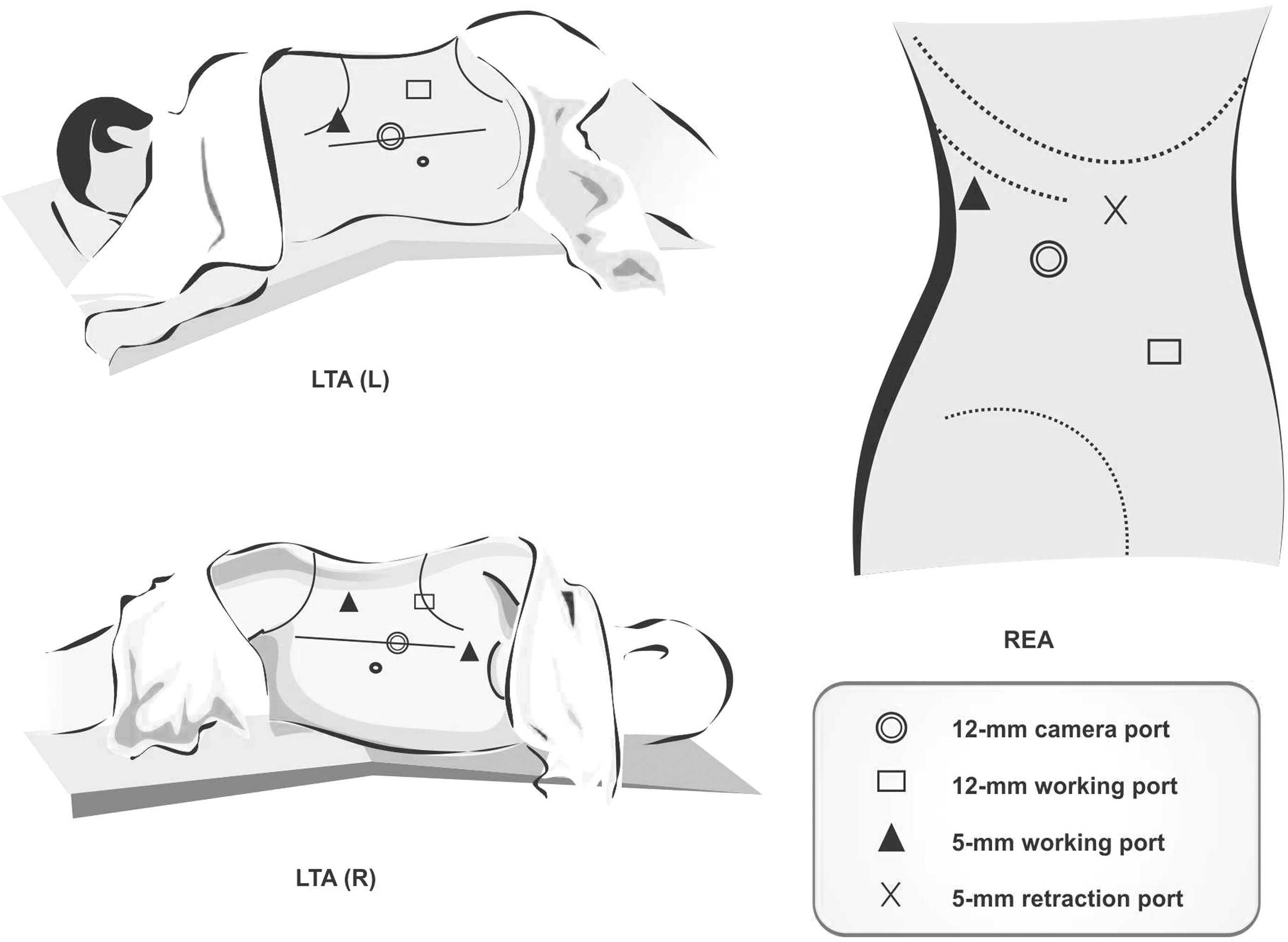
Port position in laproscopic adrenalectomy. L=left; LTA=left transabdominal approach, R=right; REA=retroperitoneoscopic endoscopic approach.
Results
Over a period of 7 years 148 LA were done at our institute of which 19 patients underwent simultaneous bilateral LA. The mean age of patients was 37.72 (range 16–65) years with a female preponderance by 15:7. Eight patients had Cushing's syndrome after failed pituitary surgery while five had ectopic ACTH dependent syndrome and six had bilateral macronodular hyperplasia (Table 1). Preoperatvely, 4 patients (20%) had steroid-induced psychosis and 10 (50%) had hypokalemia. Two patients with ectopic ACTH-dependent Cushing's syndrome and two with ACTH-dependent Cushing's syndrome posthyposphysectomy with pituitary microadenoma, who were severely ill with rapidly progressing hypercortisolism causing proximal muscle weakness and uncontrolled hypertension, underwent emergency bilateral LA. Fifteen patients underwent bilateral simultaneous LA by LTA on both sides. Four patients underwent LTA on left side and REA on the right side of which one patient had previous cholecystectomy.
ACTH=adrenocorticotrophic hormone; L=left; LTA=lateral transperitoneal adrenalectomy; MAH=macronodular adrenal hyperplasia; R=right; REA=retroperitoneal endoscopic adrenalectomy; S/P=status post; SOL=space occupying lesion.
The mean operative time for simultaneous bilateral cases was 199.45±72.43 minutes with a mean blood loss of 72.72±48.6 mL. Patients were tube free and on oral feeds on the first postoperative day; they were fit for discharge from surgical perspectives by the sixth postoperative day on an average but were retained in the hospital for 1 week or more for adjusting the dose of steroids.
Early complications occurred in five patients (26% Clavien Grade II-V) (Table 2) who underwent bilateral simultaneous LA that included two cases of minor wound infection/delayed wound healing, and one each of port site hernia, pleural effusion, atelectasis, and sepsis leading to death. The port site hernia through the 10 mm subcostal working port on the right side (LTA) was laparoscopically repaired using Proceed™ surgical mesh (Ethicon, Inc.). The port site hernia was observed at 3 months after adrenalectomy and repaired 5 months after the detection. The pleural effusion was minimal and transudative that resolved with aspiration and chest physiotherapy. The 65-year-old woman who expired had undergone emergency adrenalectomy for a suspected small cell carcinoma of lung causing rapid deterioration of health in the form of proximal muscle weakness and respiratory distress. She developed acute respiratory distress syndrome, sepsis, renal failure, and acute coronary syndrome leading to death.
DM=diabetes mellitus; HT=hypertension; LRTI=lower respiratory tract infection; NA=none available; RT=radiation therapy; UTI=urinary tract infection.
Long-term follow-up (Table 3) of the 19 bilateral LA patients ranged from 6 to 73 months with a mean duration of 32.6 month. Three patients were completely lost to follow-up after surgery. Of the 19 patients, there were 3 deaths, 1 on the 13th postoperative day mentioned above. Two patients died 2 years after adrenalectomy. One of them died from acute intestinal obstruction although his Cushing's syndrome was symptomatically and biochemically under good control. The other patient did not improve after surgery, and continued getting recurrent infections and fluctuating blood sugars. Of the three deaths, two had ectopic ACTH secreting Cushing's syndrome and the third had failed pituitary ablation for Cushing's disease.
FP=failed pituitary surgery; E=ectopic; Hyp=hyperplasia.
Three patients developed Nelson syndrome after 4 months, 1 year, and 2 years of adrenalectomy respectively (Table 2). Two of them were successfully treated with radiotherapy; and one was lost to follow-up. Five patients had adrenal crisis and all of them developed in the first year the earliest at 2 weeks postoperatively precipitated with a urinary tract infection. One patient had pulmonary embolism 3 months after surgery that was successfully treated with anticoagulants and continued on maintenance warfarin. Twelve patients had diabetes before surgery of whom the diabetic status of only nine patients is available for long-term evaluation. Six of them had good glycemic control after surgery within the first year out of which four patients could completely stop and two could substantially reduce their antidiabetic medication. Two patients continued to have psychosis.
Discussion
Adrenal surgery has been revolutionized with advances in laparoscopy in the past two decades. LA has replaced OA in Cushing's syndrome. 10 LA in Cushing's syndrome can be unilateral adrenalectomy for cortisol-producing adenoma but otherwise usually needs bilateral adrenalectomy. Indications for bilateral simultaneous partial LA are bilateral cortisol-secreting adenomas and asymmetric ACTH-independent macronodular adrenal hyperplasia (AIMAH). Bilateral simultaneous total LA is done in ACTH-independent Cushing's syndrome caused by primary pigmented nodular adrenal disease or AIMAH and ACTH-dependent Cushing's syndrome that failed attempts at removal of ACTH-secreting tumor (pituitary or ectopic). 11 LA is contraindicated in patients with invasive adrenocortical carcinomas, very large tumors (e.g., >10 cm in diameter), and patients with malignant ACTH-secreting pheochromocytomas. 11
Trans-sphenoidal surgery is the treatment of choice for Cushing's disease but it has a failure rate of 20%–40%. 12 –14 The success rate of trans-sphenoidal surgery is highest for microadenomas (90%) followed by macroadenoma (65%). 13,14 Macroadenomas may invade areas that are not resectable as in our series where a lady had the macroadenoma invading the cavernous sinus and the base of the skull, encasing a segment of the right carotid artery, infiltrating the right tentorial leaf, and extending to the posterior fossa. Pituitary gland could not be separately identified from the mass. Microadenomas may escape detection and resection at the time of pituitary surgery.
Options following failed pituitary surgery include medical adrenalytic therapy, repeated trans-sphenoidal operation, γ-knife irradiation, and bilateral adrenalectomy. Medical therapy is poorly tolerated due to the side effects of long-term treatment. γ-knife irradiation has a slow onset of action with patients achieving normal cortisol in 6–18 months. It is effective in 63%–83% but causes pituitary insufficiency in 17%–50%. 15,16 Bilateral simultaneous adrenalectomy immediately reverses the hypercortisolic state in Cushing's disease and laparoscopic approach decreases the operative morbidity of this procedure 17 as seen in two of our patients who had undergone pituitary surgery for micoradenoma but progressed and developed recurrence of Cushing's disease. One of them a young lady who was being managed in the intensive care unit (ICU) on ventilatory support was administered intravenous infusion of etomidate (inhibitor of 11 and 17 alpha hydroxylase) for acute control of hypercortisolemia. 18
Patients with ectopic ACTH secreting Cushing's syndrome often have an occult or unresectable source of ACTH. 19 The manifestations of hypercortisolism suddenly appears and rapidly progresses as seen in two of our patients. One was a young lady who had all evaluations including inferior petrosal sinus sampling negative. The other was an elderly lady with comorbidities (coronary artery disease, diabetes mellitus) who succumbed in the postoperative period to Multiple organ dysfunction syndrome. Usually ectopic ACTH secreting tumors are indolent like bronchial or thymic carcinoid, islet cell tumors, and medullary carcinoma of thyroid. 19 Some of these tumors like carcinoid even with careful radiological imaging take >20 years to localize. 19 Simultaneous bilateral LA in such situations is an effective treatment modality with reduced morbidity when compared with OA. 9,20 In patients with no identifiable source or malignancy, urgent bilateral simultaneous LA helped in relieving the progression of and resolving Cushingoid symptoms (proximal muscle weakness, hypertension, diabetes, and weight gain) in a month.
LA scores over medical management of Cushing's syndrome in its safety, tolerance, and efficacy. With medical management complete blockade is only transient; ACTH levels rise and override the blockade so that larger dose of enzyme inhibitor is needed. Side effects and intolerance to medications are high and only a few patients are able to continue long-term medications. 9
Technically bilateral simultaneous LA involves performing two LAs in a single patient. This leads to a prolonged operating time, but it reflects the learning curve as seen in various series and also entails the time required for repositioning and redraping the patient before proceeding to the second side. 7 The learning curve probably reflects the increased time taken in identifying the landmarks and the adrenal gland immersed in the excessive fatty tissue in patients with Cushing's syndrome. 4 The prolonged operating time has not been found to result in the sequelae of extended laparoscopic surgery such as hypercarbia, hypertension, dysrhythmia, or hypoxemia. 21 In our series, the operating time was prolonged (>210 minutes) in the initial few cases and no patient had any sequelae of prolonged surgery. Retroperitoneopscopic approach was attempted only on right side because the inferior vena cave (IVC) is a constant and easily identifiable landmark; dissection along it in the suprahilar region facilitates rapid localization of the adrenal gland and its vasulature. It is also a better option in patients with previous transabdominal surgery as in one of our case where the said patient had previously undergone surgery on this side (cholecystectomy) and in patients with pre-existing cardiorespiratory disease. 22 Though the dense retroperitoneal fat and small space would seem to make the surgery difficult, meticulous dissection and identification of the psoas muscle helps in the longitudinal orientation. During LA careful monitoring of other parameters like maintaining intra-abdominal pressures <15 mm Hg and end tidal carbon dioxide <45 mm Hg is pertinent. 23 Additional maneuvers like DVT prophylaxis, interruption of pneumoperitoneum during repositioning, and post procedure early ambulation with chest physiotherapy help in preventing complications, reducing morbidity, and facilitating early recovery of patients from this disabling disease. No patient developed any thromboembolic complication in the early postoperative period but one had pulmonary embolism at 3 months postoperatively. Cushing's syndrome has a hypercoagulable state related to the abnormalities in Factor VIII and von Willebrand Factor, higher levels of plasminogen activator inhibitor-1 and reduced fibrinolytic capacity. Improvements in these factors start after 1 month and normalization can take up to 1 year. 24,25
Patients with Cushing's syndrome are immunocompromised and have fragile tissue, and are predisposed to delayed wound healing, easy bruisability, and increased bleeding. LA is associated with less tissue injury. This has been studied in animal models at Mayo clinic. 26 It revealed that nitrogen balance, wound scores, and tensile strength at 24 hours and 1 week were more favorable in the LA than the OA. Thus bilateral simultaneous LA in Cushing's syndrome offers all the advantages of minimal access surgery with reduced morbidity and early wound healing (Table 3). 7,8,11,21 Nevertheless, the majority of complications in this study was wound related (3/19), two of which were minor and could be managed with conservative measures. Port site requires meticulous closure and one may avail the use of port closure device to prevent hernia. Quicker convalescence with early ambulation indirectly helps in preventing many of the complications of morbid open surgery in Cushing's syndrome. Patients with hypercortisolism undergoing adrenalectomy have increased morbidity and mortality rates. Morbidity rate of as high as 40% and mortality of 14% has been reported. 14,27 Mortality rate of 0.2% has been reported by Assalia and Gagner 28 in a large series of 2550 LAs of which the majority of deaths occurred in patients with Cushing's disease (4/7). Our series of 148 adrenalectomies had two deaths (mortality rate 1.3%) with one being in a patient with Cushing's syndrome.
Laparoscopy improves the visualization of the adrenal gland and its resection to completion, thereby reducing the chances of retained remnants and adrenal rest tissue, 11 although significant truncal obesity and retroperitoneal fat may make the dissection difficult. Intraoperative laparoscopic ultrasonography facilitates the identification of glands in difficult situation and thus its complete removal. 7 Fracture and seeding of the fragments of adrenal tissue resulting in residual functioning adrenal tissue is known with experiences in open total bilateral adrenalectomy 29,30 and specimen retrieval should be done using an endobag. In the present series, none of the patients had any residual adrenal tissue as confirmed by the stress Synachtan test.
The management of adrenal pathologies is a team-based approach involving the endocrinologists, anesthetists, intensivists, and surgeons. The endocrinologists help in the postoperative adjustment of replacement hormones. The length of hospitalization tended to be longer with a mean hospital stay of 9.6 (range 4–15) days for adjusting the dosage of medications though the patients were deemed fit for discharge from the surgical perspectives (drain and tube free, on oral feeds) at a mean of 4.2 days.
Majority of our patients got good metabolic control in the long run with regard to diabetes and the effects of hypercortisolism like proximal muscle weakness. Patients, however, need to be carefully observed for developing Addisonian crisis and Nelson syndrome, particularly within the first year.
Conclusion
Bilateral simultaneous LA is an effective, safe, and curative treatment option for recurrent Cushing's disease after pituitary surgery and in ectopic Cushing's syndrome. The main advantage is the reduced morbidity; wound related complications, and cosmesis in these patients. The visualization and magnification help in better identification and complete removal of the gland within a reasonable operating time and learning curve. Good knowledge of the surgical anatomy and delicate tissue handling and dissection are important for the success of LA. A team based approach with the endocrine, anesthesia, and ICU services are pertinent in the success of bilateral simultaneous LA in this subset of patients with higher rates of surgical morbidity and mortality.
Footnotes
Acknowledgments
Disclosure Statement
No competing financial interests exist.