
Abstract
Background and Purpose:
An integral component of many urologic reconstructive surgical procedures is the positioning of a Double-J stent to span the anastomosis. Some surgeons prefer to place a retrograde stent during cystoscopy, either during or after the reconstruction. In this communication, we describe our straightforward and effective approach of performing this critical step intracorporeally using robotic assistance in a variety of upper tract urologic reconstructive procedures.
Patients and Methods:
We examined our Institutional Review Board-approved database of robotic surgeries to identify reconstructive operations that included the intracorporeal placement of a Double-J stent since 2008. Our step-by-step method for stent placement during various robotic urologic reconstructions is detailed, including procedures involving the proximal, mid, and distal ureter. With the aid of a bedside assistant-surgeon, we delineate how the console surgeon is able to perform this step of the procedure completely intracorporeally, without the need for repositioning or cystoscopy.
Results:
Since the inception of our robotic surgical program in 2008, we have used these robotic stent placement techniques in 150 patients. The average time of robotic intracorporeal stent placement across the anastomosis was 3.5 minutes. Three patients did experience proximal stent migration, as documented on postoperative radiographs, but all were treated with conservative measures, because their anastomosis was not affected and severe symptoms did not develop. No patient needed stent replacement, and each stent was subsequently removed ureteroscopically without sequelae.
Conclusions:
Our robotic intracorporeal Double-J stent placement approach is simple and effective, avoids the need for cystoscopy and fluoroscopy, and can be used in any type of upper urinary tract urologic reconstruction.
Introduction
There is no consensus regarding the optimal approach and timing to ureteral stent placement during pyeloplasty. 2 Preoperative retrograde Double-J stent placement adequately decompresses the renal pelvis but may make clear delineation of the obstructing segment difficult; in addition, a decompressed redundant pelvis can lead to a challenging dissection. Furthermore, excision of the obstructed segment as well as repair of the neoureteropelvic junction anastomosis, particularly during the posterior aspect, may be more difficult in the presence of the preplaced stent. 6 Alternatively, antegrade Double-J stent placement may be performed after the completion of the anterior or posterior ureteropelvic anastomosis repair. 6
Previous reports have described the use of a 14-gauge angiocatheter for the introduction of the Double-J ureteral stent, using the Seldinger technique, and relying on intraoperative ultrasonography for confirmation of placement. 7 While this technique avoids many of the limitations of preplaced stent placement, there may be a learning curve, and confirmation of the distal stent curl location in the bladder can also be difficult without additional procedures. Also, the 14-gauge angiocatheter technique may not be possible in adult patients, especially in the setting of obesity. Other urologic reconstructive procedures, such as ureteroureterostomy and ureteroneocystostomy, also often involve placing a stent across the repair, yet there is no solidarity on how to approach this. We describe our simplified, time-saving technique of intracorporeal antegrade and retrograde stent placement during robotic urologic reconstruction with a discussion of potential advantages.
Patients and Methods
Our technique for intracorporeal antegrade or retrograde stent placement and manipulation during robot-assisted renal and ureteral reconstructive surgery precludes the need for cystoscopy and patient repositioning. This approach can be used for patients in the full flank, semilateral, semilateral with modified lithotomy, and supine position with or without modified lithotomy. With Institutional Review Board approval, we searched our database of robotic procedures to identify those reconstructive operations that involved intracorporeal Double-J stent placement since 2008 and identified 150 such cases. Below is a description of the technique.
Preparing the stent
The floppy tip of the 0.035-inch guidewire is passed through the open end of the Double-J stent. The floppy tip of the guidewire is allowed to project 4 to 5 cm ahead of the tip of the stent to keep the end of the Double-J stent straight. A hemostat forceps may be applied extracorporeally to hold the assembly. This premounted stent is ready to be passed through a 14-gauge angiocatheter, 3-mm trocar, or larger trocar as needed. We typically pass it through an assistant trocar of any size. While this may cause a decrease in the pneumoperitoneum, it usually is minimal because this step only needs a short time to perform. If needed, a moist gauze piece can be placed around the stent assembly to minimize the loss of pneumoperitoneum from the stent being passed through the trocar.
Stent manipulation and placement
The Foley catheter is clamped (after using it to distend the bladder) before stent placement to ensure that the bladder is full. Alternatively, we have administered intravenous furosemide to help distend the bladder. Some have found the use of this diuretic to increase urinary extravasation during the repair, but we have not experienced this. Either method is efficient, and we leave it up to surgeon preference. At the appropriate time during the reconstruction, the stent is advanced intracorporeally through the assistant port. The console surgeon uses robotic instruments to manipulate the stent into the ureter.
For antegrade intracorporeal stent placement, as required during a pyeloplasty, once the posterior anastomosis is complete, the stent is passed through the ureter and down into the bladder until approximately 20 cm of the stent has been passed or resistance is encountered (Fig. 1). At this point, the assistant surgeon removes the wire approximately 3 to 4 cm, while the console surgeon simultaneously advances the stent further. The console surgeon then stabilizes the stent intracorporeally while the assistant surgeon removes the guidewire completely, resulting in the curling of the proximal and distal portions of the stent. This proximal stent curl can be placed into the renal pelvis, and the pyeloplasty can subsequently be completed. In young and adolescent children, if a pyeloplasty is performed without an assistant port, a 14F intravenous canula (angiocatheter) is placed transcutaneously to allow for passage of the premounted stent.
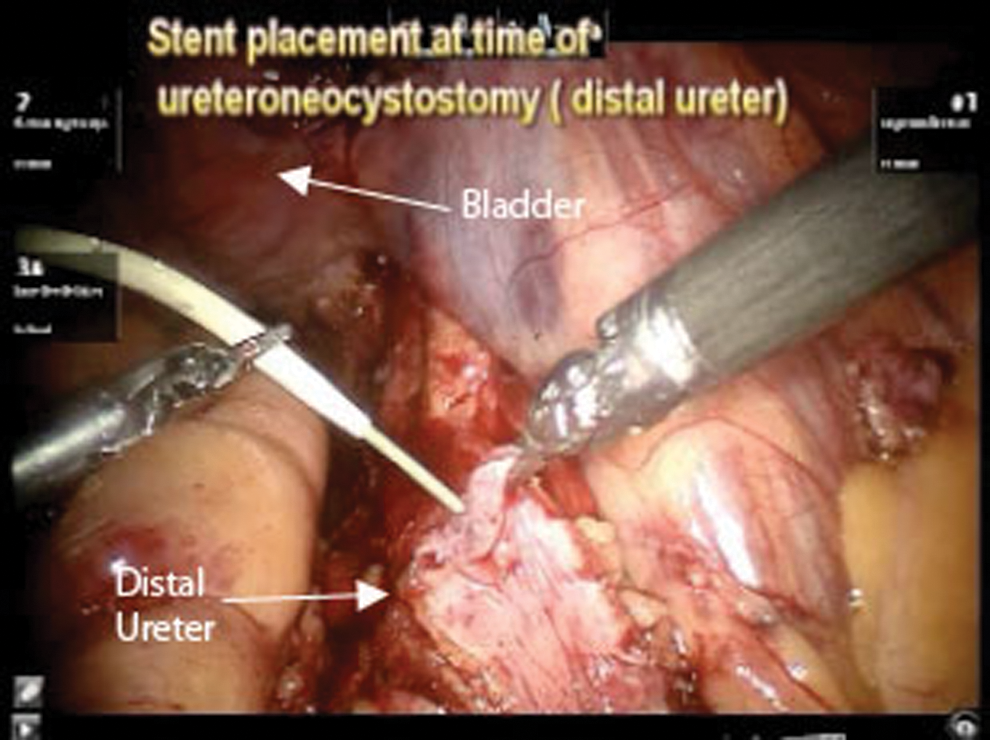
Stent placement at time of ureteroneocystostomy (distal ureter).
For retrograde intracorporeal stent placement, as needed during an ureteroneocystostomy, the stent/wire complex is introduced as previously detailed. The console surgeon then manipulates the stent/wire assembly retrograde through the ureter until the appropriate length of the Double-J stent has been advanced or resistance is met, at which point the assistant surgeon removes the wire, causing the distal end of the stent to curl (Fig. 2). The console surgeon then places the distal curl of the stent into the bladder through the cystotomy, and the neocystotomy reconstruction can be completed over the stent.
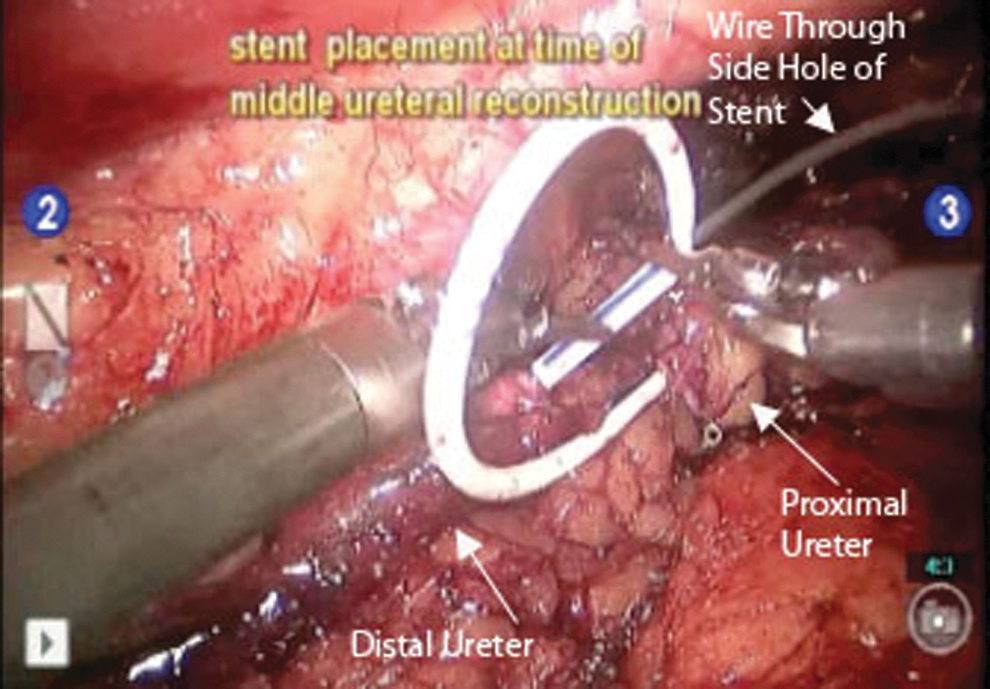
Stent placement at time of middle ureteral reconstruction.
Occasionally, intracorporeal stent placement may require both antegrade and retrograde manipulations, as during ureteroureterostomy for mid ureteral reconstructions (Fig. 3). The stent/wire assembly is passed into the surgical field, as described, before initiating the repair or after a few anastomotic sutures have been placed, as per surgeon preference. Typically, it is our propensity to pass the stent in the retrograde direction first, until resistance is met in the kidney. At this point, the console surgeon, while stabilizing the stent, gently removes the wire, leaving it intracorporeal. The exposed floppy tip of this same wire is then inserted through a side hole of the Double-J stent by the console surgeon and passed distally through the stent until the distal curl is straightened. Now, while buttressing the previously placed proximal portion of the stent, the console surgeon passes the distal stent until the appropriate length has been advanced or resistance is met in the bladder. At this time the wire is removed, while holding the stent in place, and the ureteroureterostomy is completed.
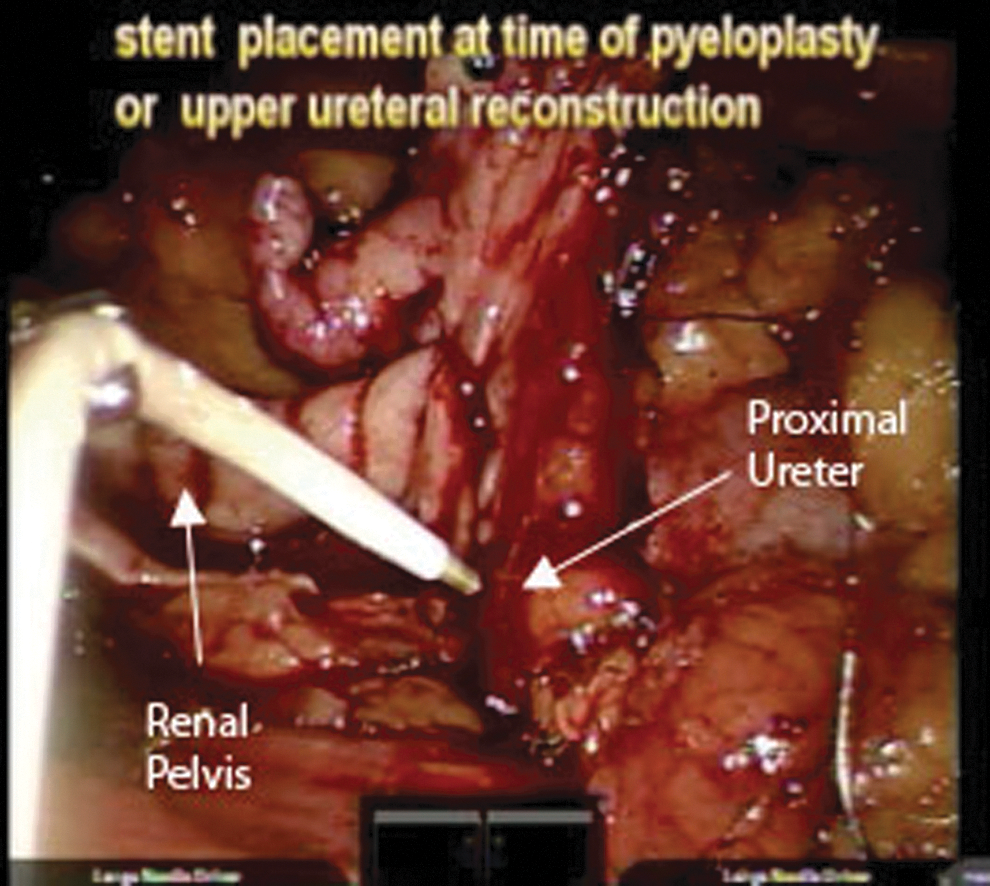
Stent placement at time of pyeloplasty or upper ureteral reconstruction.
Reflux of clear fluid through the stent holes helps confirm appropriate placement, and if there is doubt, one can instill methylene blue into the bladder to help better visualize fluid extravasation from the stent. We usually use a fixed length Double-J stent, chosen based on measurement of ureteral length on intravenous pyelography or urography (if available) or as estimated based on patient height. 8 It remains surgeon preference whether the posterior anastomosis needs to be completed before passing the stent, but it is generally appreciated that completing the reconstruction may be easier if the posterior anastomosis has already been performed before passing the stent. In certain cases, however, individual patient anatomy may dictate the passing of the stent before performing any aspect of the anastomosis.
A video of our technique for robotic intracorporeal Double-J stent placement for upper tract urologic reconstruction can be viewed at Journal of Endourology Part B, Videourology. 9
Results
Over the last 3 years, we have used this approach in 150 patients during the following procedures: Pyeloplasty (103), ureteroneocystostomy (20), ureteroureterostomy (9), ileal conduit urinary diversion (7), megaureter repair (7), ureterocalicostomy (2), ureterolysis (1), ureterolithotomy (1). Mean time of insertion (from the time the stent is introduced into the surgical field) was approximately 3.5 minutes (range 1–6 min) for all procedures. No difficulties or perioperative complications were noted. In 3 of the 150 patients, on the postoperative radiography of the kidneys, ureters, and bladder, it was found that the stent was not coiled in the bladder, but, rather, had migrated into the ureter. These patients did not have any discomfort, so we did not make any attempt to reposition the stent. The stent was ultimately removed ureteroscopically at the appropriate time.
Discussion
Multi-institutional experience with robot-assisted laparoscopic pyeloplasty and upper tract reconstructive surgery demonstrates that this approach is safe, durable, and efficacious for primary and secondary ureteroplevic junction obstruction with or without concomitant stones, and for patients with a solitary kidney. 4 There is still considerable debate on which method is best suitable for placement of a stent across the anastomosis. 2,10 In the above multicenter review, 71% preferred the antegrade technique while 29% preferred the retrograde approach. 4
The published literature has several anecdotal techniques of antegrade and retrograde stent placement during laparoscopic and robot-assisted pyeloplasty or ureteral reconstruction. One report describes laparoscopic stent placement after ureterolithotomy. In this technique, the stent is passed over a stylet, cut just short of the stent length, and pushed with the help of a grasper. 11
Other groups have described insertion of a 14-gauge angiocatheter and advancing an external-internal ureteral stent under direct vision down the ureter. A percutaneous access to the intrarenal collecting system was then performed with another 14-gauge angiocatheter. A 1.9F stone basket was next passed through the angiocatheter to grasp the proximal arm of the stent and manipulate it out through the skin. 7
Mandhani and associates 6 describe their technique of antegrade stent placement whereby the stent and ureteral catheter are straightened over the guidewire and introduced through the lumen of a 5-mm hook or suction canula via a subcostal port.
Wu and colleagues 12 describe their novel combined antegrade and retrograde technique of stent placement in retroperitoneal laparoscopic dismembered pyeloplasty in 22 patients. A ureteral catheter was inserted into the midureter cystoscopically. During pyeloplasty, the ureteral catheter was pushed up and grasped outside the body through the laparoscopic port. Its proximal end was extracorporeally sutured to the distal end of the Double-J stent with a silk thread. The length of the silk was about that of the urethra. The ureteral catheter was then pulled down until its proximal end exited the external orifice of the urethra, while the stent was pulled smoothly and antegrade into the ureter and bladder. After the proximal end of the stent was positioned in the renal pelvis, the silk was cut and the ureteral catheter was removed.
Another technique of antegrade stent placement was described, in which a 19F polytetrafluoroethylene coated needle is passed through the anterior abdominal wall in line with the ureter and negotiated into the proximal ureter. A 0.032-inch guidewire is then passed through the needle into the bladder and a double pigtail catheter is placed. 12 Other groups have used an Alken needle, passed percutaneously adjacent to the anastomosis, and then a straight guidewire was steered through the anastomosis into the bladder and a 4.8F stent was passed over this guidewire into the bladder. 13
Wayment and coworkers 14 describe their technique of intraoperative cystoscopic stent placement in robot-assisted pyeloplasty. Unique patient positioning and draping allow access to the urethra for intraoperative cystoscopy. As the surgeon performs the posterior portion of the anastomosis, the assistant performs simultaneous flexible cystoscopy and retrograde stent placement. Stent location is confirmed by direct vision.
Viprakaset and coworkers 15 described a similar technique in 111 consecutive patients undergoing laparoscopic pyeloplasty. The patient was positioned in the lateral decubitus position, with a lower extremity support modification used in female patients. This allowed initial open-ended catheter placement and subsequent access to the perineum and final stent placement throughout the procedure without need for patient repositioning. In addition, intraoperative fluoroscopy was possible to delineate any complex ureteral anatomy.
Preoperative retrograde stent placement has several possible disadvantages—namely decompression of the renal pelvis by the stent, thus rendering dissection and full mobilization of the renal pelvis and ureteropelvic junction more difficult. 16 The entire extent of the stenosis and dysplastic segment is not as well defined, thereby hindering optimal spatulation and posterior anastomosis. 6,16 Furthermore, preoperative retrograde stent placement may make it difficult to appreciate the influence of crossing vessels as possible causes of hydronephrosis, which would influence the surgical approach and technique. 5,17 Subsequent laparoscopic manipulation may result in stent migration, moving the distal end of the stent out of the bladder and into the distal ureter, and the stent may be accidentally cut during dissection.
Thus, it has been suggested that intracorporeal stent placement is easier to perform after the completion of the posterior anastomosis. Some authors, however, do mention that during intracorporeal antegrade stent placement, it may be sometimes difficult to negotiate past the ureterovesical junction and thereby result in stent malposition. 6 We have encountered stent malposition in only three (2%) cases in our practice, and we have not needed to replace those stents because patients have been asymptomatic.
Conclusions
The described intracorporeal antegrade and retrograde stent placement techniques during robotic urologic ureteral reconstructive procedures are efficient, cost-effective, and relatively simple to master. There is no need for patient repositioning, cystoscopy, or fluoroscopy, thereby avoiding increased operative time, cost, and radiation exposure. In upper tract robot-assisted reconstructive surgery, intracorporeal Double-J stent placement should be the ideal choice.
Footnotes
Disclosure Statement
No competing financial interests exist.