
Abstract
Purpose:
We report our initial experience with the first series of laparoendoscopic single-site (LESS) radical cystectomy and urinary diversion performed by a single surgeon using a homemade single-port device at a single institution in China.
Patients and Methods:
Between December 2010 and February 2011, we performed five LESS radical cystectomis using a homemade single-port device composed of an inverted cone device of polycarbonate and a powder-free surgical glove. The port was placed into a 5-cm periumbilical incision. The conventional laparoscope and laparoscopic instruments were inserted through the single-port. No additional ports were needed for radical cystoprostatectomy and bilateral standard pelvic lymphadenectomy. Cutaneous ureterostomy and ileal conduit urinary diversion were used for our patients, respectively. Perioperatively, oncologic data and complications were collected and analyzed.
Results:
All the procedures were completed successfully. The mean extirpative operative time was 208.2 (168–280) minutes, estimated blood loss was 270 (100–500) mL, bowel recovering time was 9.75 (6–12) days, and postoperative hospital stay was 19.5 (14–28) days. One patient needed a transfusion of 400 mL of red blood cells. The pathologic evaluation revealed negative margins and negative lymph node involvement. After the operations, one patient had a bowel obstruction, while another patient died from cardiac disease. Mean follow-up time was 143 (110–173) days.
Conclusions:
In our experience, LESS radical cystectomy is clinically feasible and safe for selected patients, but requires a learning curve. Our homemade single-port device is a cost-effective and convenient device. Although the initial outcomes have been promising, the long-term oncologic evaluation of these patients awaits.
Introduction
Currently, the conventional laparoscopic approaches use five ports to perform both the cystectomy and the lymphadenectomy. With advancements in surgical instruments, consideration of cosmesis, and trends toward minimal invasiveness, the number of laparoendoscopic single-site (LESS) procedures that use a single incision site has increased recently. After Rané and associates 5 performed the first urologic LESS, this technique has been used for various urologic diseases. 6 –8
Although many groups have used a commercially available multichannel trocar, such as the Uni-X™ Single Port (Pnavel Systems, Brooklyn, NY) and the R-Port™ (Advanced Surgical Concepts, Dublin, Ireland), to perform LESS, such devices may not be suitable for the medical environments of other countries. Thus, we used our homemade single-port device composed of a surgical glove and an inverted cone device of polycarbonate to perform LESS operations.
In this article, we report our initial experience with LESS radical cystectomy and urinary diversion performed by a single surgeon using a homemade single-port device at a single institution in China.
Patients and Methods
Patients
Between December 2010 and February 2011, a retrospective analysis of our first five consecutive patients (five men) who underwent LESS radical cystectomy and urinary diversion performed by a single surgeon (LLM) who was skilled in conventional laparoscopic surgery was performed. The same inclusion and exclusion criteria that are used for conventional laparoscopic surgery were applied. Patients were given a choice of conventional laparoscopy, LESS, or open surgery. We performed LESS operations only when the patients provided written consent. The demographic, perioperative, and pathologic outcomes data were evaluated.
Surgical technique
After general anesthesia, the patients were placed in a low modified lithotomy position with both arms adducted and padded. With the patients in a 20- to 30-degree Trendelenburg incline, a 5-cm periumbilical skin incision was made (Fig. 1). Single-port intra-abdominal access was gained by sequence incision to the peritoneum through the periumbilical incision.

Periumbilical skin incision.
We used a size 7½ powder-free surgical glove and an inverted cone device of polycarbonate whose inner diameter was 3.5 cm, height was 4.0 cm, and outer diameter was 5.5 cm as the homemade single-port device (Fig. 2). The surgical glove was inserted into the inner ring, and the wrist of the glove was fixed to the outer diameter of the outer ring with the silk suture. Three fingers of the glove were cut, and two 14-mm trocars and one 5-mm trocar were inserted (Fig. 3). The inner ring of the single port was inserted into the periumbilical incision site, and the outer ring of the single-port, in which there were many pinholes, was fixed to the skin by seaming (Fig. 4).

Components of the homemade single-port device.

Our home-made single-port device.
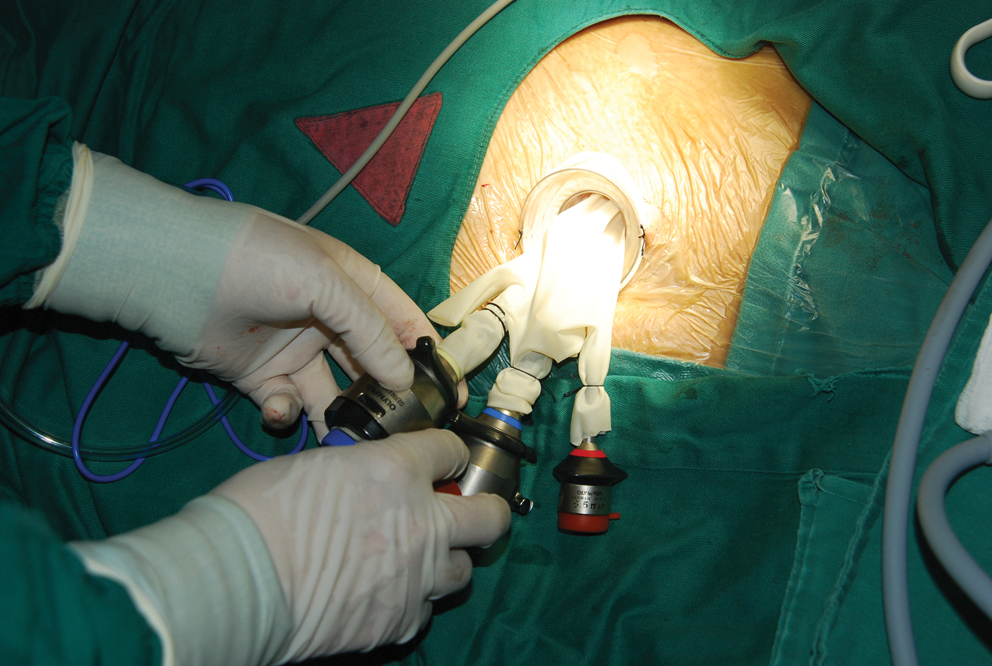
Fixed to the skin by seaming.
The homemade single-port device was constructed by securing the fingers of the glove to the end of the three trocars with a silk suture and fixed to the outer ring of the single-port followed by insufflation of the peritoneum with CO2 to 14 mm Hg. A 10-mm rigid 30-degree Olympus laparoscope was inserted into the peritoneum through the 14-mm trocar, and the conventional laparoscopic instruments were inserted through the remaining trocars.
After intra-abdominal access, the ureters were identified and mobilized from the bifurcation of the common iliac artery to the ureterovesical junction and subsequently dissected distally toward the bladder to assist in urinary diversion formation. We attempted to preserve the gonadal vessels and periureteral tissue to ensure a rich vascular supply to the distal ureter. A 5-mm Hem-o-lok clip (Weck Closure Systems, Research Triangle Park, NC) was placed at the distal ureter. A ureteral margin was sent for frozen section analysis to rule out malignancy.
After the ureteral dissection, we performed bilateral standard pelvic lymph node dissection. Anatomic boundaries of the standard lymphadenectomy include the genitofemoral nerve laterally, the obturator nerve medially, the node of Cloquet distally, and the area of the aortic bifurcation proximally. The vessel sheath of the external iliac vessel was split longitudinally with J-hook electrocautery. The tissue anterior to the external iliac artery and vein was dissected longitudinally, and then we skeletonized the two vessels circumferentially. After dissection along the medial aspect of the external iliac vein, the obturator nerve was identified, and the fatty tissue surrounding it was dissected. Then, the fatty tissue along the external iliac artery medial to the genitofemoral nerve was removed. The adipolymphatic tissue that surrounded the common iliac arteries and the aortic bifurcation was dissected cephalad. All nodal specimens were sent separately to the pathology department according to their respective anatomic locations.
Radical cystectomy began with a transverse peritoneotomy deep in the rectovesical cul-de-sac at the second (distal) peritoneal fold. Dissection was performed along the posterior aspect of the bilateral seminal vesicles and vasa deferentia, which were not mobilized and dissected individually but were maintained en bloc along with the bladder specimen. This retrovesical dissection was carried distally toward the prostate, where the Denonvilliers fascia was incised horizontally to enter the Denonvilliers space, with care taken to avoid rectal injury. An inverted U-shaped peritoneotomy was performed along the undersurface of the abdominal wall, dividing the urachus high near the umbilicus and extending caudad widely, lateral to the right and left medial umbilical ligaments, respectively. The anterior surface of the bladder and the Retzius space was developed, maintaining all prevesical fat with the bladder specimen. The endopelvic fascia was incised bilaterally. The anterior inverted U and the posterior transverse peritoneotomies were now joined on either side, bringing the lateral vesical pedicles into view.
The bladder specimen was tautly retracted anterolaterally to the left, placing the right lateral pedicle on stretch, which was defatted and transected up to the incised endopelvic fascia with the harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH). Similarly, the left lateral vesical pedicle was controlled. The dorsal vein complex was controlled with a suture of 2-O polyglactin to guarantee good hemostasis and then cut with the puboprostatic ligament; the urethra was mobilized circumferentially and occluded with a Hem-o-lok clip to avoid spillage of urine, and then transected with a harmonic scalpel. A full-thickness circumferential biopsy specimen of the urethral stump was obtained for frozen-section analysis. The cystoprostatectomy specimen was completely separated, entrapped in a self-made bag, and extracted through the port site. We chose intrafascial nerve-sparing prostatectomy for one patient, whose age was less than 60 years, to improve sexual function after the operation.
We chose two types of urinary diversion: Cutaneous ureterostomy for the first two patients and ileal conduit urinary diversion for the other patients. The cutaneous ureterostomy was performed in the same manner as conventional laparoscopic urinary diversion. The ileal conduit urinary diversion was constructed extracorporeally through the periumbilical incision.
Results
We have successfully performed five LESS radical cystectomies and urinary diversion procedures in five patients without the use of additional extraumbilical ports. Table 1 lists the patient demographics and surgical results. The median operative time was 208.2 (168–280) minutes for LESS radical cystectomy and bilateral pelvic lymphadenectomy, 32.5 (20–45) minutes for creating the cutaneous ureterostomy, and 135 (130–140) minutes for ileal conduit urinary diversion. Successive LESS cases have resulted in improved operative times (for LESS radical cystectomy) with our increased experience. Mean estimated blood loss was 270 (100–500) mL, and only one patient needed a transfusion of 400 mL of red blood cells in the operation. No intraoperative complication was observed. Postoperative pain management consisted of tramadol and oxycodone and acetaminophen.
BMI=body mass index; OR=operating room; EBL=estimated blood loss; MI=myocardial infarction.
Histopathologic examination of the specimens, according to the 7th American Joint Committee on Cancer cancer staging, revealed one pT1N0M0, one pT2aN0M0, two pT2bN0M0, and one pT3aN0M0. The World Health Organization grading was high grade in three patients and low grade in two patients. The surgical margins were tumor free in all the patients. One patient, who received the ileal conduit urinary diversion, had a small bowel obstruction that resolved spontaneously after placement of a nasogastric tube. One patient died 1 day after operation, but this was related to myocardial infarction.
The initial surgery was performed in December 2010, with the average follow-up time of 143 (110–173) days. Except for the deceased patient, the other patients were alive and tumor free at the last time of follow up in July 2011, and they were satisfied with the cosmetic results. At the last follow-up, the incision of the urinary diversion appeared healthy, with no evidence of diversion-related complications. We use the International Index of Erectile Function (IIEF-5) questionnaire to assess the patients' sexual function at follow-up. In these five patients, we used intrafascial nerve-sparing prostatectomy for only one patient (age 48 years), and his IIEF-5 score was 13 (mild erectile dysfunction), while the other alive patients did not have sexual intercourse.
Discussion
Radical cystectomy and bilateral pelvic lymph node dissection constitute the most definitive treatment for urothelial carcinoma of the bladder. 1,9 Since Sánchez de Badajoz and associates 10 first performed laparoscopic radical cystectomy for bladder cancer in a patient, this technique have been spread around the world and continued to evolve. The oncologic outcomes after laparoscopic radical cystectomy have been comparable to the open approach. 11 With the significant technical progress that has occurred over the past several years, LESS surgeryhas advanced rapidly in the urologic field. 12 Although Kaouk and colleagues 13 have reported three cases of LESS radical cystectomy with an ileal conduit, its role in complex oncologic procedures is still under investigation.
Although the procedure seemed to add technical complexity and take longer than conventional laparoscopic radical cystectomy, LESS surgery still provides the advantages of laparoscopy, including reduced blood loss and postoperative pain. In our series, the extirpative operative time and blood loss were comparable to that of published LESS radical cystectomy series. 13,14 The low doses of analgesic demonstrated minimal postoperative discomfort. There was only one patient who needed a transfusion of 400 mL of red blood cells as a direct result of the procedure. This patient died 1 day after operation, but death was related to cardiac disease. This prompted us to adopt stricter preoperative screening criteria in the recent era.
Sexual function after operation should be considered for the radical cystoprostatectomy patients. We chose intrafascial nerve-sparing prostatectomy for selected patients whose age was less than 60 years to improve sexual function. There were two reasons: The intrafascial nerve-sparing prostatectomy effectively enabled limited trauma to the neurovascular bundles and the prostatic anatomy of the bladder cancer was clear; as a result, it was easier to perform intrafascial nerve-sparing prostatectomy. In these five patients, we used intrafascial nerve-sparing prostatectomy for only one patient (age 48 years), and his IIEF-5 score was 13 (mild erectile dysfunction), while the other surviving patients did not have sexual intercourse. We need continue the follow-up, however, to observe the effect of this operation.
The surgical margin status and lymph node yield are significant prognostic variables of patients with bladder cancer. The importance of a greater lymph node yield was illustrated by Brunocilla and associates, 15 but the optimal number has still been debated. 16 Thus, extended lymphadenectomy is the optimal option for radical cystectomy, 17 and it can be approached laparoscopically. 18 Although we would like to perform LESS extended lymphadenectomy in the future, in our series, we performed bilateral standard lymphadenectomy because extended lymphadenectomy could be complicated by severe lymph leakage and our LESS technique for radical cystectomy is still at the beginning. The negative surgical margins and negative lymph nodes of the bladder specimen in all patients, however, demonstrate that the LESS radical cystectomy procedure has good tumor control.
Urinary diversion after cystectomy must be chosen for the urologist technically and also for the patient's physiologic status. For old and high-risk patients, who are associated with major complications, cutaneous ureterostomy may be indicated, and the operative risk is low. 19 Thus, we chose cutaneous ureterostomy for the first two patients because of their poor physical status. The ileal conduit, however, has been the most widely used diversion after radical cystectomy for bladder carcinoma. 20 Thus, in the other three patients, ileal conduit urinary diversion was constructed extracorporeally with advantages in terms of costs saved, time saved, and surgical technique in comparison with intracorporeal creation. Nevertheless, these patients' ileus and hospital stay time was a little longer than the first two patients, because of interference with the bowel to construct the ileal conduit. Even more, one patient had a small bowel obstruction after the operation that resolved spontaneously after placement of a nasogastric tube. These complications can be resolved, however, with more experience.
There are several trocar options for LESS including the R-port and Uni-X single laparoscopic port system. We used our homemade single-port device, however, which has several merits. First, this device consists of common equipment and materials and is more cost-effective than current commercial ports. Second, the elasticity of the surgical glove minimizes the interference of the instruments with the laparoscope and magnifies the range of motion. These advantages may make it easier to control the instruments. Third, it can prevent subcutaneous emphysema and bleeding, caused by a tamponade effect of the inverted cone device and the surgical glove. Lastly, conventional surgical equipment can be used, and even more, different numbers and sizes of instruments can be accommodated with our homemade device with no difficulty.
This is the first published series of LESS radical cystectomy and bilateral standard pelvic lymph node dissection performed by a single surgeon using a homemade single-port device for urothelial carcinoma at a single institution in China. This operation has a steep learning curve, including coordination between the surgeon and the camera holder, navigating the instruments within a limited range of motion, and counterintuitive movements. The initial oncologic results have been approved through the single site. At the average 143 days of follow-up, except for the dead patient, no evidence of recurrent or metastatic disease was identified in the other patients. More large and long-term studies are needed, however, to determine how this technique compares with the traditional laparoscopic and open approach.
Conclusions
In our experience, LESS radical cystectomy is clinically feasible and safe for selected patients, but requires a learning curve. Our homemade single-port device is a cost-effective and convenient device. Although the initial outcomes have been promising, the long-term oncologic evaluation of these patients awaits.
Footnotes
Disclosure Statement
No competing financial interests exist.