
Abstract
Purpose:
This study evaluates the feasibility, perioperative, and renal functional outcomes with total, selective, and nonarterial clamping techniques during minimally invasive partial nephrectomy.
Methods:
A retrospective review of laparoscopic and robot-assisted partial nephrectomies by a single surgeon from January 2007 to July 2010 was performed. Patients underwent total hilar clamping, selective (segmental) artery clamping, progressive clamping from segmental to main renal artery clamping, or resection without hilar clamping. Patient demographic, perioperative, and oncologic outcomes were analyzed. Change in renal function was assessed by glomerular filtration rate (GFR) calculation and differential function on pre- and postoperative renal scans.
Results:
A total of 68 patients underwent laparoscopic or robot-assisted partial nephrectomy. Those with a history of surgery for renal masses and elective conversion to radical nephrectomy were excluded. A total of 57 patients were analyzed (32 total hilar, 8 progressive arterial clamping, 13 selective arterial, and 4 without clamping). There were no significant differences in preoperative patient or disease characteristics between the groups. The progressive clamping technique was found to significantly decrease the total renal ischemia time compared with the total hilar clamp technique. There was no other significant difference in transfusion rate, complications, or other postoperative outcomes. There were no significant differences between the groups in intermediate-term (mean 411 days) renal function changes.
Conclusions:
Minimally invasive partial nephrectomy without vascular occlusion and with selective arterial clamping is feasible and can be safely performed. With this intermediate-term follow-up there was no clinically significant benefit seen for selective regional or nonischemic techniques.
Introduction
Despite the preservation of renal tissue during laparoscopic partial nephrectomy, there is still concern that total arterial clamping (TAC) may lead to damage of functional nephrons from ischemia and reperfusion injury. To minimize these changes, cold ischemia is frequently utilized in an open approach and regional ischemia approaches have been suggested to allow renal perfusion to uninvolved parenchyma. Selective arterial clamping (SAC) is one such approach and has been utilized during an open approach with kidney cooling. 7 In addition, porcine studies utilizing SAC in a solitary kidney model employing a laparoscopic approach have demonstrated significantly less renal ischemic damage versus those with total clamping. 8,9 Herein we aim to evaluate different approaches to ischemic control during minimally invasive partial nephrectomy.
Materials and Methods
After obtaining appropriate IRB approval, a retrospective review was performed analyzing consecutive laparoscopic and robot-assisted partial nephrectomies performed by a single surgeon (E.P.C.) from January 2007 to July 2010. Patient demographic information, perioperative, and oncologic outcomes between the groups were analyzed using an analysis of variance (ANOVA) calculation. The groups were also reanalyzed after rearranging the groups by including the progressive group in either the selective or the total hilar clamp group. Preoperative and postoperative renal function was assessed with glomerular filtration rate (GFR) calculation using the Modification of Diet in Renal Disease equation. Intermediate-term GFR was calculated using the most recent serum creatinine in the absence of acute disease affecting renal function. Differential renal function was assessed using preoperative and postoperative renal scans at least 1 month after surgery. Those patients who required conversion to radical nephrectomy or who had a history of prior surgical intervention for renal masses were excluded from the analysis. Cancer recurrence was assessed with cross-sectional imaging at time intervals dependant on the tumor characteristics.
All cases were performed by transperitoneal dissection of the renal artery, vein, and mobilization of the kidney. The artery was then assessed for vasculature amenable to selective clamping. In the cases of TAC, the renal artery and vein were occluded with laparoscopic bulldog clamps. In those patients undergoing SAC, the segmental renal arteries leading to the region of the tumor were identified and skeletonized (Figs. 1 and 2). The segmental renal artery was occluded with a laparoscopic bulldog clamp (Fig. 3). If brisk bleeding was noted during deep dissection of the tumor, hemostatic techniques using clips, cautery, or sutures were used to control bleeding points in the nephrectomy bed. A progressive arterial clamping (PAC) technique was employed in cases requiring greater hemostasis, using laparoscopic bulldogs on contributing segmental arteries, and subsequently the main renal artery if necessary during resection. The tumor base was ablated using radiofrequency ablation or argon beam coagulation, followed by hemostatic glue. The renorrhaphy was closed using interrupted suture with bolsters before changing to a sliding hemolock renorrhaphy since March 2008. In all cases of vascular occlusion, intravenous mannitol and lasix were administered. Times of selective, progressive, and total hilar clamping were meticulously recorded.
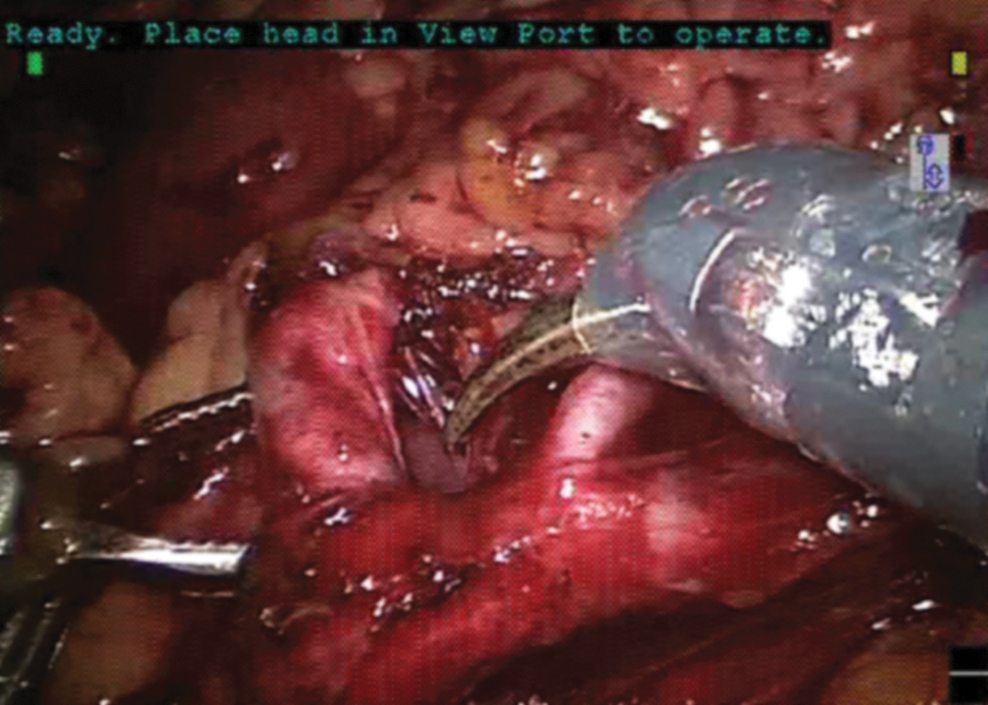
Dissection of segmental artery in preparation for selective clamping.
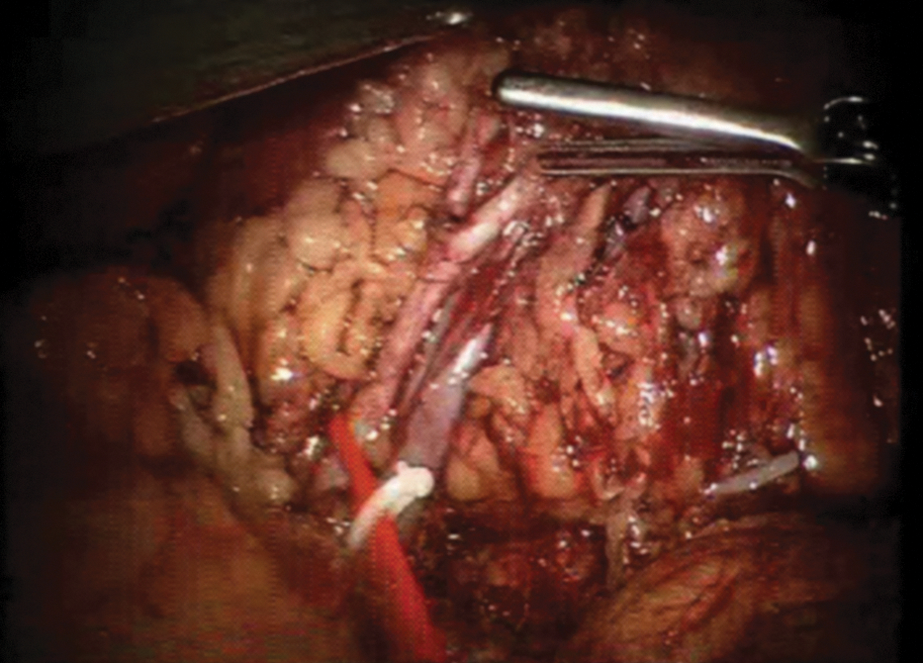
Another example of dissection of segmental artery, before clamping.

After clamping with laparoscopic bulldog clamp.
Results
There were 68 patients identified who underwent a laparoscopic or robot-assisted partial nephrectomy performed by a single surgeon from January 2007 to July 2010. Five patients were excluded from analysis secondary to previous renal surgery including contralateral partial nephrectomy, contralateral total nephrectomy, and history of renal embolization in one patient. Six patients in the total hilar clamp group were excluded from analysis secondary to conversion to radical nephrectomy for deep tumor involvement in five and to open partial nephrectomy in one patient for multifocality of several tumors who also had a history of contralateral nephrectomy. There was one conversion from robotic to laparoscopic partial nephrectomy in the nonhilar clamping group (nonarterial clamping [NAC]) due to robotic arm collision. There were no conversions in the selective and progressive groups.
While there was a trend in the NAC group to be older, have smaller masses, and lower GFR, there was no significant difference in patient or disease characteristics preoperatively (Table 1). There was no difference in mean tumor size between the groups. There was one focal positive margin in the total arterial clamp group (total positive margin rate 1.7%), without positive margins in the other groups. Six patients in the TAC group, one in the PAC group, five in the SAC group, and two in the nonclamp group were found to have benign disease (23% total), all others had renal cell carcinoma. One patient in the total clamp group was found to have systemic progression of disease at a mean follow-up of 411±382 days. There were no local recurrences of disease.
In mL/minute/1.73 m2, calculated using MDRD.
BMI=body mass index; MDRD=Modification of Diet in Renal Disease; GFR=glomerular filtration rate.
There were four complications in the TAC group; two pseudoaneurysms requiring embolization, one inferior epigastric artery pseudoaneurysm from port placement, and one patient with acute renal failure which resolved without intervention. There were two complications in the PAC group; one pseudoaneurysm which required embolization and subsequent nephrectomy, and one thrombosis of a lower pole renal artery after performing upper pole segmental clamping with progressive TAC. There were two complications in the SAC group; one urine leak requiring percutaneous drainage, and one episode of urinary retention requiring temporary foley drainage. There were no complications in the nonclamp group.
There was a trend toward higher blood loss in the nonclamp and progressive clamp groups compared with the total hilar clamp group (288 and 250 v 150 mL, p<0.05), but no significant difference was found on ANOVA analysis (p=0.058). There was a significantly shorter total renal ischemia time utilizing the progressive technique versus the total clamp technique (18 v 32 minutes) (Supplementary Fig. 1). There were no other differences in perioperative outcomes noted between the three groups (Table 2) (Supplementary Fig. 2). The mean warm ischemia time in the TAC group was 32±10 minutes (range 14–53). The mean segmental arterial clamp time was 28±3 minutes (range 24–30) in the PAC group with progression to a mean total renal artery clamp time of 18±3 minutes (range 15–23) in this group. The mean regional ischemia time in the SAC group was 22±10 minutes (range 14–43). Although we did note increasing comfort with segmental arterial dissection over time, there was no learning curve trend noted in complication rate, operative time, or warm ischemia time within the groups.
In cases of progressive clamping, selective clamping time was recorded from the onset of segmental artery clamping until arterial revascularization. Clamp time was recorded as time of complete renal artery occlusion until arterial revascularization.
Significantly longer total kidney ischemia in the total clamp group compared with the progressive clamp group.
EBL=estimated blood loss.
No significant difference in intermediate-term GFR was found between the four groups (Table 2) at a mean follow-up of 411±382 days. Both preoperative and postoperative renal scans were available in 22 (TAC), 4 (PAC), 7 (SAC), and 2 patients (NAC). There was no statistically significant difference in decreased ipsilateral renal function found on MAG-3 study (Table 2). There were no other significant differences found when including the progressive clamping group with either the selective or the total clamp groups and reanalyzing the data.
Discussion
Small renal masses are being increasingly discovered corresponding to the increased prevalence of cross-sectional imaging. Nephron sparing surgery has emerged as the preferred treatment option for these lesions with equivalent oncological outcomes to radical nephrectomy and preserved renal function for T1 renal cancer. 1,2,6 Although kidneys are frequently extracted for live donation without fear of subsequent renal impairment, nephrectomy for renal masses occurs in a vastly different patient population. Evaluation of uninvolved ipsilateral renal parenchyma has shown vascular sclerosis or renal parenchyma abnormalities in up to 90% of cases, 10 stressing the importance of renal preservation.
Emerging studies are revealing decreased risk of renal insufficiency, cardiovascular morbidity, and overall mortality in those patients undergoing nephron sparing surgery versus total nephrectomy. 3 –5 Increasing emphasis should therefore be placed on not only preventing patients from requiring dialysis, but also maximizing renal function. The current AUA guidelines recommend partial nephrectomy as standard of care for anatomically amenable T1a lesions and as an alternative standard for T1b renal masses. 6
Although functional parenchyma is spared during partial nephrectomy, TAC may lead to damage of functional nephrons due to ischemia and reperfusion injury. Studies have suggested minimizing warm ischemia time to <30–40 minutes. 11,12 Alternatively, kidney cooling may be utilized in an open approach to decrease ischemic damage. Laparoscopic hypothermic techniques have also been described, which may be of benefit in preserving renal function. 13 Laparoscopic techniques to minimize hilar clamping times such as selective arterial embolization, “on-demand” clamping, and early clamp release have also been described. 8,14
Several series have reported laparoscopic partial nephrectomies without hilar clamping. In a study by Koo comparing 11 laparoscopic partial nephrectomies without hilar control with 10 with hilar control, no difference was found in blood loss, transfusion rate, or complications. There was no difference in postoperative serum creatinine levels between the two groups. 15 Gill et al has reported a series of 15 patients who underwent “zero ischemia” laparoscopic and robot-assisted partial nephrectomy after pharmacologically inducing hypotension during excision. They noted no transfusion requirement, morbidity related to hypotension, and minimal change in postoperative GFR. 16 In our series, there was a trend toward higher estimated blood loss (EBL) in the NAC and PAC groups compared with the TAC group (288 and 250 vs. 150 mL); however this was not statistically (p=0.058) or clinically significant, as there were no differences noted in transfusion rate. There was a lower change in GFR and renal function based on renal scan in the NAC group compared with the other groups, however this did not reach statistical significance and the sample size was small with four patients.
There have been several reports of attempts to occlude blood flow to the renal mass while minimizing ischemia to normal functional parenchyma. Renal parenchymal clamping with vascular clamps has been used to perform open partial nephrectomy without hilar clamping with success. 17,18 Segmental artery occlusion with intravascular gel polymer has also been described in a porcine model. 14
Selective segmental arterial clamping is another option which is anatomically possible in a number of kidneys. In a study of 30 cadaveric kidneys, two-thirds of kidneys had four or greater segmental arteries. 19 Porcine studies utilizing SAC in a solitary kidney model have demonstrated significantly less renal ischemic damage versus those with total clamping. This was manifested by lower serum creatinine levels at 1 week and viable renal parenchyma comparable to nonclamped parenchyma. 8,9 Nevertheless, this was only at 1 week and may have little significance as the kidney recovers over a longer term.
Segmental arterial occlusion during an open approach with kidney cooling has been described by Nohara et al. This series demonstrated a significantly lower increase in serum creatinine during short-term follow-up in those undergoing selective clamping versus total vascular occlusion. 7 Shao et al has reported a series of 38 patients undergoing laparoscopic SAC compared with 37 with total hilar clamping. They noted an increase in warm ischemia time and EBL, but no statistically significant difference in complication rates. There was an advantage in postoperative renal function in the selective versus total clamping group (22% v 26% decrease in ipsilateral GFR). 20
We noted a comparable selective warm ischemia time in our series compared with Shao et al, but did not note a difference in change in renal function between the TAC, PAC, and SAC groups in our series. There was a significantly shorter total renal ischemia time when utilizing a PAC technique versus starting the resection with total hilar clamping (18 vs. 32 minutes). The challenges of segmental clamping stem from intrarenal branching. We found the technique more feasible on the right because of increased prehilar branching secondary to the increased arterial length. There were no statistically significant differences in operative blood loss, transfusion rates, or postoperative complications between the SAC, PAC, and TAC groups in our series.
Our follow-up is longer than most of the other series and may reflect the significant ability of functional recovery of the kidney. Our total arterial clamp group had a mean clamp time within the acceptable ranges historically described (30–40 minutes), and may have also contributed to the lack of statistical difference observed between the groups. However, the total clamp time was longer than most of the times touted in the literature achievable with complex techniques such as early unclamping and no clamping. This underscores the question of whether or not ischemia time is of concern as long as it is within the 30-minute range.
There are some limitations of our study that need to be considered. First, all patients had a normal contralateral kidney which limits the ability to interpret serum creatinine changes. However, we did have renal scans evaluating functional changes in the operated kidney. Other than cannulating the ureter and collecting the creatinine clearance of the operated side, renal scans are presently the only reasonable way to evaluate functional change. Another limitation is sample size. We may have seen a greater trend or even statistically significant difference if the nonclamping group had been larger. This may be especially true when comparing nonclamp versus TAC. Finally, additional variables that are difficult to analyze include the amount of normal parenchyma excised along with the tumor and intra-renal vascular and parenchymal changes. Renal biopsy may be one way of evaluating parenchymal changes that may have an impact in the long run.
Several questions remain unanswered. Does it matter if regional or no ischemia can be achieved in the setting of a two-kidney model? What effect does total and regional ischemia have on residual nephrons over a longer period of time (>10 years)? What is the best way to evaluate functional changes in residual parenchyma in the long-term? Do we really know the genuine capacity of functional recovery of a human kidney in the in vivo model? Despite these questions, most patients undergoing partial nephrectomy with total, segmental, or no ischemia do not require dialysis or develop significant chronic kidney disease based on most reports.
Our series highlights the advancements that can be made to minimize total renal ischemia. Although there was no statistically significant difference found with regard to renal function, every attempt should be made to minimize ischemia time within reason. Further, total hilar clamping was not found to have a significant impact in the intermediate-term, and the surgeon should not sacrifice vision, patient safety, or the ability to perform an oncologically appropriate operation simply to minimize ischemia.
Conclusions
Laparoscopic and robotic partial nephrectomy without clamping and with selective and PAC is feasible and can be safely performed. Progressive clamping techniques did lead to a significantly shorter total renal ischemia time, however there was no statistically significant difference found in renal function between those undergoing total, progressive, selective, and nonarterial clamping during intermediate-term follow-up in this series. Larger sample size and a longer follow-up are needed to determine if there are long-term benefits for renal function with these techniques.
Footnotes
Disclosure Statement
Humphreys is consultant for Boston Scientific, Lumenis, and Medafor. Castle is a consultant for Baxter and speaker for Intuitive Surgical. No competing financial interests exist for the other authors.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.