
Abstract
Background and Purpose:
The Habib radiofrequency coagulation (RFC) device coagulates bleeding surfaces and may eliminate the need for hilar clamping, thus eliminating warm ischemia time and decreasing the technical complexity of laparoscopic partial nephrectomy (LPN). We retrospectively review a series of patients who underwent clampless LPN with RFC to study the safety and feasibility of this approach.
Patients and Methods:
The Institutional Review Board-approved, Johns Hopkins Minimally Invasive Urologic Surgery Database (1994–2011) was queried for patients undergoing clampless LPN with RFC between September 2008 and January 2010 by a single surgeon (MEA). Respecting a 0.5-cm surgical margin, the lesion was circumscribed with the RFC device to create an avascular plane, and standard laparoscopic shears were used to excise the tumor in a bloodless field without hilar clamping. Patient outcomes were analyzed for safety and feasibility of this approach.
Results:
Fifteen patients underwent RFC LPN. Median tumor diameter in our patients was 1.6 cm (range 1–7.3 cm). Seven (46.7%) tumors were exophytic in nature, and the remainder were mesophytic. Median nephrometry score was 5 (range 4 to 7). Median operative time was 155 minutes (range 100–210 min), and median estimated blood loss was 100 mL (50–500 mL). There were no positive margins, and two postoperative complications (urine leak and clot retention) were encountered. No recurrences were noted with short-term follow-up.
Conclusion:
Clampless RFC LPN can be performed safely in carefully selected patients with favorably positioned tumors. In this initial experience, we observed excellent perioperative and short-term oncologic outcomes. Future comparative studies will dictate the role of RFC-assisted LPN in the armamentarium of kidney surgeons.
Introduction
LPN is an appealing alternative to OPN, because LPN avoids a large flank incision and its associated morbidity. 6 LPN and robot-assisted LPN, however, necessitate a unique technical skill set including intricate laparoscopic suturing techniques and robotic training. Because of the advanced skill needed for LPN, warm ischemia time can be prolonged compared with OPN, 7 and clamping of the renal hilum during PN can lead to renal parenchymal ischemia, which, if sustained, can cause acute tubular necrosis. 8 Thus, there may be a need for technologies that can minimize or eliminate warm ischemia time during LPN.
The Habib radiofrequency coagulation (RFC) device (AngioDynamics, Queensbury, NY) coagulates bleeding surfaces and may eliminate the need for hilar clamping, 9 thus eliminating warm ischemia time and decreasing the technical complexity of LPN. Such a device may increase the adoption of LPN by decreasing technical complexity and ischemia-related complications. As such, it has been described in experimental porcine models 10 and OPN series, 11 but only a few reports exist describing the usefulness in LPN with a limited number of patients. 9,12,13 In this study, we retrospectively review a series of patients who underwent clampless LPN with RFC to study the safety and feasibility of this approach.
Patients and Methods
The Institutional Review Board-approved, Johns Hopkins Minimally Invasive Urologic Surgery Database (1994–2011) was queried for patients undergoing clampless LPN with RFC between September 2008 and January 2010 by a single surgeon (MEA). Patient and tumor characteristics along with perioperative outcomes were analyzed to study the safety and feasibility of this approach. Tumors were classified according to the proportion of the tumor protruding off the surface of the kidney: Exophytic (>60%), mesophytic (40%–60%), and endophytic (<40%) 14 and based on R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score as described by Kutikov and Uzzo. 15 Glomerular filtration rate was calculated using the Chronic Kidney Disease Epidemiology Collaboration formula. 16
The surgical technique used differed from standard LPN in that the RFC device was used to coagulate the tissues surrounding the tumor to create a bloodless field for excision. The tumor itself was not ablated with the device as is performed in laparoscopic radiofrequency ablation of renal masses. Respecting a 0.5-cm surgical margin, the lesion was circumscribed with the RFC device to create an avascular plane around it. After coagulation, we used standard laparoscopic shears to excise the tumor in a bloodless field and without hilar clamping.
In the initial experience (n=5), the renal hilum was dissected in the circumstance that vascular control was needed. In the case of deep tumors, argon beam coagulation and hemostatic adjuncts (ie, surgical) were used to ensure hemostasis. After tumor excision, collecting system entry, if encountered, was closed with laparoscopic suturing; otherwise, reconstruction was not performed. The resection site was observed under low-pressure pneumoperitoneum to ensure adequate hemostasis before tumor extraction. The tumor was retrieved in a standard fashion using a retrieval sac and sent for pathologic analysis.
Results
From September 2008 to January 2010, 15 patients underwent RFC LPN. Patient demographics are detailed in Table 1. Of note, median age was 49 years (range 38–83 y). The series had nine (60%) men and six (40%) women. Preoperatively, 4 of 15 (26.7%) patients had a Charlson score of 0, 7 (46.7%) had a score of 1–2, and 4 (26.7%) had a score of 3–4. The majority of patients, 9 of 15 (60%), had an American society of Anesthesiologists (ASA) score of 2 while 6 of 15 (40%) had an ASA score of 3.
ASA=American Society of Anesthesiologists; EBL=estimated blood loss; OR=operative time; WIT=warm ischemia time; LOS=length of stay; GFR=glomerular filtration rate.
Median tumor diameter in our patients was 1.6 cm (range 1–7.3 cm). On preoperative imaging, seven (46.7%) tumors were exophytic in nature, and the remainder were mesophytic lesions. Median nephrometry score was 5 (range 4 to 7). The 7.3-cm tumor was an angiomyolipoma exophytic (>60%) in character, 7 mm from the collecting system, posterior in location, and entirely below the polar line. Thirteen (86.7%) patients underwent surgery with three or four laparoscopic ports; the remaining 2 patients underwent single port surgery. Median operative (OR) time was 155 minutes (range 100–210 min) with a median estimated blood loss (EBL) of 100 m: (50–500 mL). None of the patients needed hilar clamping, and there were no positive margins on final pathologic analysis. CT images of the kidney bed at 1 month and 17 months after surgery for a patient are shown in Figure 1.
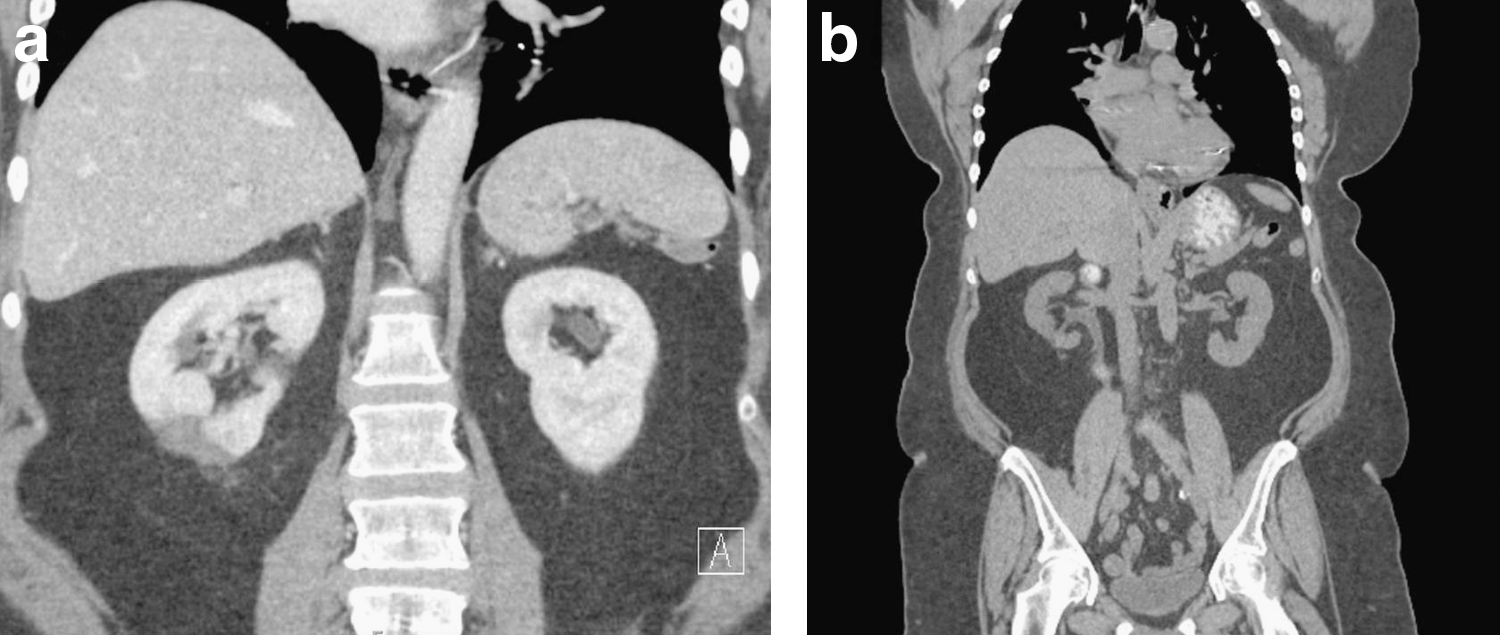
Coronal postoperative CT images at
There were two postoperative complications. One patient experienced a persistent urine leak that resolved after 4 weeks with conservative measures. Another patient experienced ureteral clot obstruction 5 days postoperatively and was treated successfully with ureteral stent placement. The patient did not need transfusion, and no pseudoaneurysm or arteriovenous fistula weas noted. The stent was removed after 21 days. There was not a significant difference in mean preoperative and postoperative creatinine levels (P=0.6) or glomerular filtration rates (GFR) (P=0.4). No recurrences were noted at a mean follow-up of 1 year (median 8 mos; range 4–17 mos).
Discussion
Recent epidemiologic data shows that, OPN is performed in 10.3% of eligible patients and LPN is performed in 0.8%, with the remainder of patients (88.9%) undergoing radical nephrectomy. On further investigation, the major factor determining whether a patient received a PN or radical nephrectomy was surgeon preference rather than patient characteristic. 17 Although there has been no attempt to determine the exact barriers that prevent surgeons from adapting OPN and LPN, fear of complications and technical complexity of the procedures likely hinder the adoption of LPN for some surgeons.
Traditionally, PN is performed by clamping the renal hilum and excising the lesion. Even relatively shorter warm and cold ischemia times of >20 minutes and >35 minutes, respectively, however, are associated with an increase in both acute and chronic renal failure, temporary dialysis, and urine leak. 8 Recent data have demonstrated that increasing clamp times increases the likelihood of acute kidney injury, chronic kidney disease, and the sequelae of renal disease. 18,19 These time-dependent complications make it more difficult for inexperienced surgeons to perform PN. Such complications may even prevent well-experienced surgeons from performing PN on larger or more complex renal tumors or in patients who cannot tolerate long, complicated procedures or renal injury. Complex reconstruction and the difficulty of laparoscopic suturing during LPN and robot-assisted LPN magnify these risks and highlight the utility in performing a clampless procedure where applicable. Indeed, studies have demonstrated improved renal functional outcomes when no ischemia was used. 20
The Habib device is a bipolar RFC device in which current flows between two electrodes in the target tissue. This results in heating of the tissue to >50°C with peak heating exceeding 100°C. 21 These temperatures are sufficient for tissue destruction and, while the device was designed for liver tumor resection, studies have shown that use of bipolar RFC devices in kidney parenchyma results in a necrotic zone defined by lack of viable vasculature. Thus, this technology allows for the creation of an excisional plane with both short-term and long-term hemostasis without the need for hilar clamping. 22
Patients in this cohort were highly selected. The majority were in excellent health by Charlson score and ASA index. Of note, four patients in our series had a Charlson score of 3–4, two of whom had baseline renal dysfunction. Renal functional outcomes were excellent using this clampless technique (Table 1). In addition, the tumors in our series had a median nephrometry score of 5 and were often smaller, more exophytic, at the periphery of the kidney, and either above or below the polar lines. Given the coagulative nature of the device, we were hesitant to use this in central or hilar tumors, fearing damage to large arterial branches that feed the remainder of the kidney.
We demonstrate rapid OR times (median 155 min), highlighting the selection of favorable tumors in this report and reflecting the omission of hilar dissection as familiarity and confidence in the technique improved. We cannot directly compare studies using the RFC device with different methodologies, but there is some current progress of note in managing small renal masses, as summarized in Table 2. In a recently published study, Wu and associates 13 analyzed the use of Habib-assisted robot-assisted PN in 42 patients for tumors of similar nature and patients at similar risk of renal disease. 13 Mean OR time for this group of patients was 373 minutes, while Nadler and colleagues 12 reported a median OR time of 435 minutes with their robotic approach (although patient and tumor characteristics were not provided). 12 Other groups, however, have demonstrated OR times on the order of 150 minutes using a more traditional LPN approach. 9 In addition, Wu and coworkers 13 reported a mean EBL of 337 mL in their robotic series, while mean EBL was 133 mL when the RFC device was used in open surgery. 11 The relatively short OR time and favorable EBL (median 100 mL) in our series are testaments to the relative ease and short learning curve of RFC LPN when used in selected patients with amenable tumors.
Five pigs had one kidney operated on during phase 1 and the contralateral operated on during phase 2 after a 2-week observation period.
RFC=radiofrequency coagulation; OR=operative; EBL=estimated blood loss; LPN=laparoscopic partial nephrectomy; OPN=open partial nephrectomy; RALPN=robot-assisted laparoscopic partial nephrectomy.
One of the limits of the Habib device is that the prongs penetrate tissue to a maximum length of 3 cm, thus limiting its use to small, peripheral, and exophytic neoplasms. Conversely, we would not recommend this technique for large, endophytic, or central tumors where complex reconstruction would be needed. In the series by Wu and associates, 13 53% of tumors were endophytic and 52% were interpolar, necessitating collecting system entry and repair in nearly 80% of patients and a high, resultant urine leak rate of 17%. We do not advocate use of the RFC device in these patients, but recommend standard LPN techniques using minimal warm ischemia, which has been demonstrated to maximize oncologic outcomes while preventing short-term complications. 23,24
Additional concerns with a RFC device involve the coagulation of tissues adjacent to the tumor. First, this may distort the appearance of the tissue during tumor resection. For surgeons who rely on these visual cues to identify a safe margin of resection, this can be confusing, especially during intended tumor enucleation. To overcome this limitation, we advocate a disciplined approach to tumor resection, maintaining at least a 5-mm margin at all times and discourage enucleation when using this technique. Fortunately, our pathologists had no problems examining the specimens and delineating a clear tumor margin. As a result, the oncologic results in this small group of patients were excellent, with no positive margins or tumor recurrences at 1-year follow-up.
Second, the RFC zone and margin may result in more destruction of viable and healthy renal parenchyma than standard LPN, and preserved renal volume and nephrons are correlated with improved renal function after PN. 25 While we did not find any significant decrease in GFR, anatomic studies of functional renal volume after RFC LPN and LPN and long-term renal functional outcomes in this cohort may delineate the ability of this technique to preserve nephrons in patients at risk for long-term renal function.
Third, there is concern that coagulation necrosis of the collecting system may cause long-term tissue breakdown, delayed closure of the collecting system, and prolonged urine leaks in Habib-assisted cases. 12 We did not find this assertion to hold true in our limited patient cohort because of the selection of patients with tumors at minimal risk of collecting system entry and meticulous closure of the collecting system when it was entered. While one patient experienced a urine leak, this leak presented immediately postoperatively and healed with standard conservative management. We believe it was not related to this technique, and future comparative studies are needed to evaluate this question in an appropriately powered analysis.
In two patients, we performed the PN with RFC assistance using a single-port technique. One of the patients was an 83-year-old man with coronary artery disease, hypertension, and hyperlipidemia. The other patient was a 43-year-old woman with no medical comorbidities. Tumor size in these patients was 4.7 and 4.2 cm, respectively, larger than the average tumor size of 1.6 cm in our series, but both were exophytic lesions. There were no complications or recurrences experienced in either patient. This is in contrast to the robot-assisted approach selected by Wu and colleagues 13 that required a minimum of five ports. Whether the use of RFC-assisted PN facilitates the use of single-port surgery in this context remains to be seen. The benefit of the single-port approach also remains unknown.
In this era of cost containment and with the wide adoption of expensive robotic equipment in urology, it is important to note that the Habib RFC device is also associated with a significant financial cost on the order of approximately $2000 per case. The emergence of further clinical data and future cost efficacy studies will help better define the role of this expensive technology in the armamentarium of the kidney surgeon.
Our study is limited in scope and lacks a control group for comparison and is meant as an initial report of feasibility and safety of this technique. Additional limitations of our report that limit generalizability include its retrospective nature and our sample of highly selected patients (good to fair health, tumors with low nephrometry score). Nevertheless, we hope that these data trigger future studies to answer important questions regarding this method of clampless PN.
Conclusion
Clampless RFC LPN can be performed safely in carefully selected patients with favorably positioned tumors. In this initial experience, we observed excellent perioperative and short-term oncologic outcomes. While we reserve the use of this technology for small, exophytic tumors in patients at risk for renal compromise with warm ischemia, future controlled studies will dictate the role of RFC-assisted LPN in the armamentarium of kidney surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.