
Abstract
Purpose:
To evaluate the effect of an indomethacin-eluting biodegradable urethral stent on the production of inflammatory cytokines in vitro and the degradation and biocompatibility of the new stent in vivo.
Materials and Methods:
The effects of an indomethacin and indomethacin-eluting biodegradable stent on monocyte chemoattractant protein (MCP)-1, RANTES (regulated on activation, normal T-cell expressed and secreted), and transforming growth factor-ß were measured in THP-1 cells by enzyme-linked immunosorbent assay. Stents (copolymer of L-lactide and glycolide acid) that were coated with 50L/50D polylactic acid and two different concentrations of indomethacin were inserted into the rabbit urethra. Stents without the drug were used as controls. Scanning electron microscopy (SEM) was used to assess the degradation of the stents. Biocompatibility was evaluated using histologic analyses of the urethral specimen. The measurements were performed at 3 weeks and 3 months.
Results:
Indomethacin and indomethacin-releasing stent material inhibited MCP-1 and RANTES production in activated THP-1 macrophages. SEM analysis revealed that indomethacin coating had no effect on the degradation process of the stents and less epithelial polyposis had developed in the indomethacin stent group. In histologic analyses at 3 weeks, indomethacin-eluting stents caused more calcification but no significant differences in other tissue reactions. At 3 months, the indomethacin-eluting stents caused less inflammatory reaction and calcification compared with the control stents.
Conclusion:
Indomethacin-eluting property can be safely added to biodegradable stents without major influence on the degradation time. The development of epithelial polyposis in the urethra can be potentially reduced by the new indomethacin-eluting urethral stents.
Introduction
The concept of using biodegradable stents after internal urethrotomy to prevent stricture recurrence has been a long interest of our research group. Biodegradable urethral stents with spiral configuration have already been used in the treatment of recurrent urethral strictures. 5,6 These stents, however, did not significantly reduce the epithelial hyperplasia and the recurrence of urethral strictures.
The idea to start testing drug-eluting stents came from interventional radiology. Drug-eluting stents have been successfully used in endovascular procedures to prevent restenosis from neointimal hyperplasia. 7,8 The drug-eluting stents have shown significant potential to reduce restenosis development after vascular intervention 9 and to reduce cardiac events compared with bare metal stents. 10
To see if we can have a similar effect in the urethra, we developed a new biodegradable urethral stent with indomethacin-eluting properties. The aim of our first study was to assess if we can develop a biocompatible indomethacin-eluting urethral stent. Also we conducted a preliminary study on whether it is possible to affect the tissue reactions in the urethra with the novel drug-eluting urethral stent.
Indomethacin is a well-known nonsteroidal anti-inflammatory drug (NSAID) that inhibits prostaglandin synthesis. 11 No reports of clinical studies about indomethacin-eluting stents have been published, however. We studied the elution profile of indomethacin-coated stents and found out that it is possible to achieve sustained elution with indomethacin from the coating of the novel biodegradable stent. 12 This encouraged us to proceed to biocompatibility studies with indomethacin-eluting stent materials.
In a standardized rabbit dorsal muscle implantation test with potential drug candidates, we found indomethacin-eluting material to have good biocompatibility properties as well as being a good platform for local drug delivery. 13 In our preliminary study of urethral in-situ biocompatibility with drug-eluting stents, we showed the desired biocompatibility. 14
The aim of our present study was (1) to evaluate the effect of indomethacin-eluting coating on the biodegradable urethral stent degradation time, (2) to assess the biocompatibility profile of indomethacin-eluting biodegradable urethral stents by using two different indomethacin concentrations in vivo, and (3) to test the effect of indomethacin-eluting biodegradable urethral stent material on monocyte chemoattractant protein (MCP)-1, regulated on activation, normal T-cell expressed and secreted (RANTES) and transforming growth factor (TGF)-β production in vitro.
Materials And Methods
Cell culture
Human THP-1 monocyte-macrophage cell line (American Type Culture Collection, Rockville, MD) was cultured at 37°C in humidified 5% carbon dioxide atmosphere in RPMI 1640 medium with 2 mM L-glutamine (Camprex Bioproducts Europe, Verviers, Belgium) adjusted to contain 1.5 g/L sodium bicarbonate, 4.5 g/L glucose, 10 mM HEPES, and 1.0 mM sodium pyruvate and supplemented with 0.05 mM 2-mercaptoethanol. The culture medium contained 10% heat-inactivated fetal bovine serum, 100 U/mL penicillin, 100 μg/mL streptomycin, and 250 ng/mL amphotericin B (all from Gibco, Paisley, Scotland, U.K.). All other reagents were from Sigma Chemical Co. (St. Louis, MO).
Cells were seeded on 24-well plates for enzyme-linked immunosorbent assay (ELISA) measurements. Monocytes were differentiated to macrophages by phorbol myristate acetate (PMA) administration (100 nM for 72 h). Indomethacin-releasing stent material was added to the cells at the time cells were seeded, and lipopolysaccharide (LPS) was added after 72 hours of incubation. At 24 hours after addition of LPS, the culture medium was collected for measurements. Cells without stent material were incubated 72 hours; after that LPS and indomethacin were added. The culture medium was collected for measurements at 24 hours after LPS addition.
ELISA measurements
The concentrations of TGF-β, MCP-1, and RANTES (R&D Systems, Inc, Minneapolis, MN) were determined by ELISA.
Animal studies
We used biodegradable braided pattern poly(lactic-co-glycolic acid) (PLGA) urethral stents (Fig. 1). The polylactic acid (PLA)/polyglycolic acid (PGA) polymer ratio in the material was 80:20; the material was obtained from PurAc biochem b.v., Groeningen, the Netherlands, and the stents were designed and manufactured at the Institute of Biomedical Engineering, Tampere University of Technology, Finland. The diameter of the stents was 6 mm and the length was 30 mm. The stents were coated with rasemic 50L/50D PLA. The coating was blended with two different concentrations of indomethacin (Orion Pharma, Finland). The indomethacin amount in the coating was 699±86 μg (low concentration) and 1943±249 μg (high concentration). For control groups, we used pure 50L/50D PLA coated stents and stents without the coating.
Biodegradable indomethacin-eluting copolymer of L-lactide and glycolide acid urethral stent. The bar in the image is 5 mm.
The institutional committee for animal research and the Western-Finland Provincial Government reviewed and approved all the animal protocols. The investigation conformed to the Guide for Care and Use of Laboratory Animals published by the United States of America National Institutes of Health.
A total of 24 male New Zealand White rabbits were used and divided into four groups. The stents were inserted into the prostatic urethra as described by Vaajanen and associates. 15 Half of the animals in each group were sacrificed after 3 weeks and the other half after 3 months.
Histologic analyses
The urethra surrounding the stent was dissected en bloc, and representative samples were taken for histologic analyses. Tissue blocks were fixed in 10% formalin and embedded in paraffin, and sections were cut and stained with hematoxylin and eosin following routine techniques. All histologic analyses were performed by an experienced pathologist who was unaware of the treatment.
The following biologic response parameters were assessed and recorded: Inflammatory changes (neutrophil infiltration), chronic inflammatory changes (lymphocyte and plasma cell infiltration), foreign body reaction, fibrosis, calcification, and eosinophil infiltration. All tissue reactions were scored semiquantitatively according to the following criteria: 0=no reaction, 1=mild reaction, 2=moderate reaction, 3=severe reaction.
Scanning electron microscopy (SEM) analyses
The degradation process in the stent and the development of epithelial hyperplasia (polyposis) was evaluated by SEM at the Department of Electron Microscopy, University of Kuopio, Finland.
Statistics
Results are expressed as the mean±standard error of the mean. When appropriate, statistical significances of the differences were calculated by analyses of variance supported by the Dunnett multiple comparisons test. Differences were considered significant at P<0.05.
Results
Effects of indomethacin and indomethacin-releasing stent material on MCP-1, RANTES, and TGF-β production in human THP-1 cells
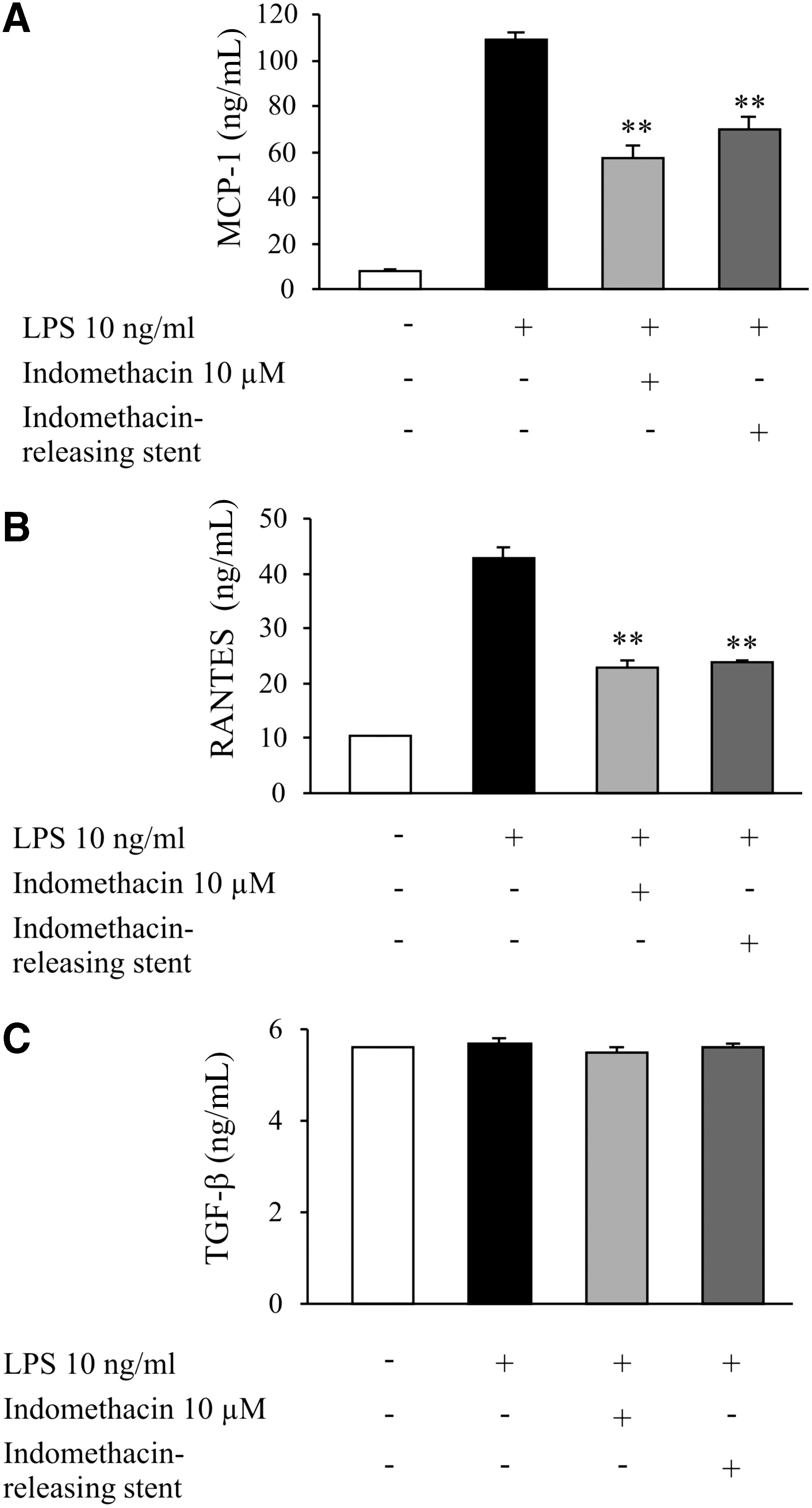
We investigated the effects of indomethacin and indomethacin-coated stent material on MCP-1, RANTES, and TGF-β production in activated human THP-1 macrophages to evaluate effects on local mediators of inflammation and fibrosis. Indomethacin at the concentration of 10 μM inhibited the production of MCP-1 and RANTES significantly, whereas it had no effect on TGF-β production (Fig. 2). Accordingly, indomethacin-releasing stent material reduced MCP-1 and RANTES production but had no effect on TGF-β release (Fig. 2), showing that the indomethacin-coated stent material was able to release bioactive indomethacin at concentrations that were high enough to cause significant anti-inflammatory effects. Stent material used was 96L/4D-PLA (poly-96D/4L-lactic acid) covered with 50L/50D-PLA coating blended with 0.51±0.06 mg of indomethacin. The rods were of 1.1 mm in diameter and 11 mm in length. Estimated in vitro degradation time of stent material was 30 weeks.
Effects of indomethacin and indomethacin-releasing stent material on lipopolysaccharide (LPS)-induced
Animal studies
All the animals started to void normally during the first postoperative day after the insertion of the stent without prolonged bleeding.
The stents were voided out of the urethra in three rabbits during the first postoperative day and were excluded from the study. All the lost stents were from the 3 weeks group, including one from the PLGA group, one from the 50L/50D PLA-coated group, and one from the low-dose indomethacin stent group.
SEM revealed that coating had no effect on the degradation process of the stents. Coating had started to degrade at 3 weeks in the indomethacin-eluting stent group as well as the control group (Fig. 3). At 3 months, there was no stent material left in either group.
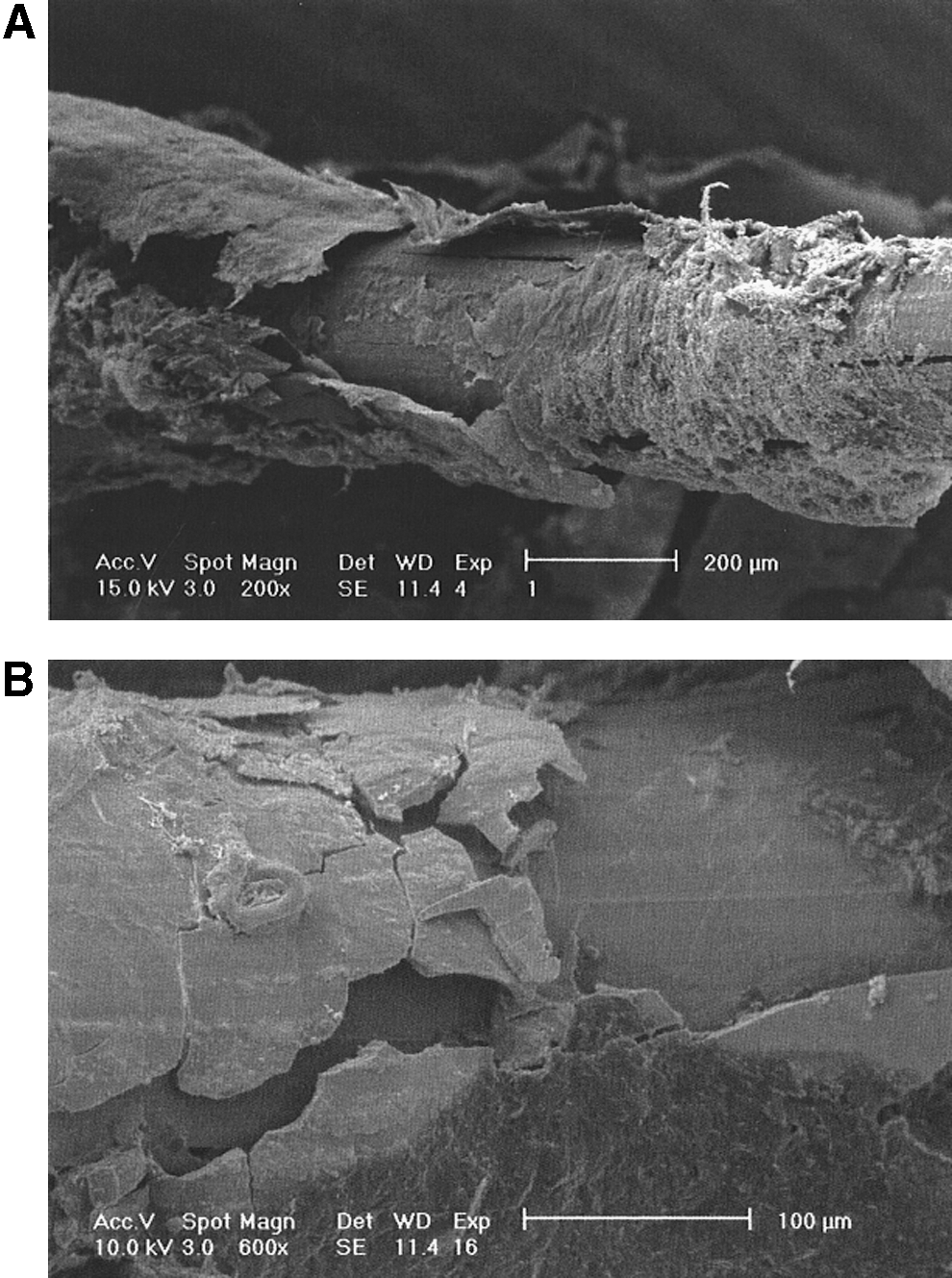
Scanning electron microscopy image of degrading coating at 3 weeks of indomethacin-eluting biodegradable stent with low indomethacin concentration
At 3 weeks, stents that contained either high or low concentration of indomethacin had induced significantly less severe epithelial polyposis than the pure 50L/50D PLA-coated stent (Fig. 4). At 3 months, the amount of polyposis was significantly decreased in all groups, and there were no differences between the groups.
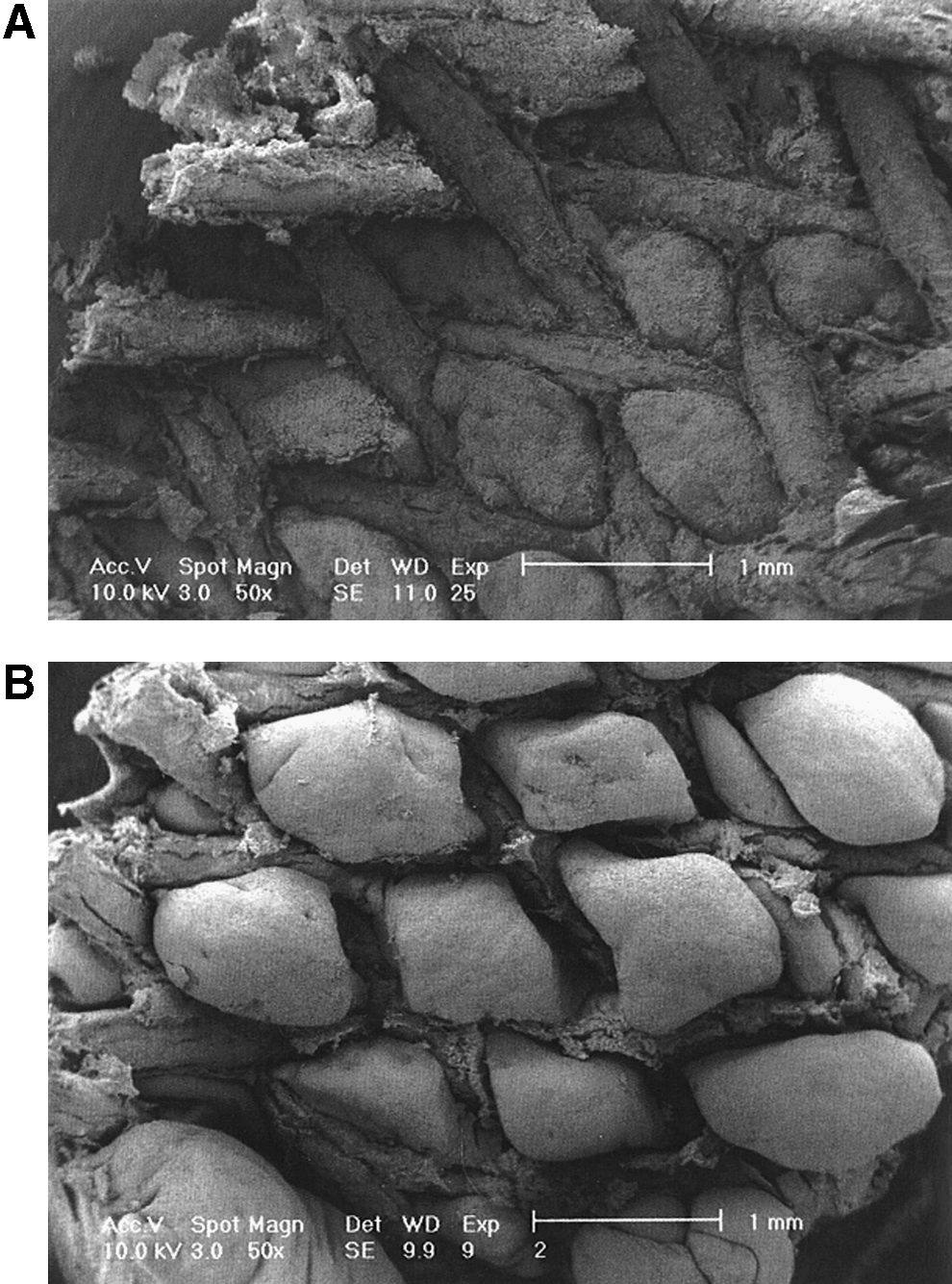
Scanning electron microscopy image of indomethacin-eluting biodegradable stent (high concentration)
Histologic analyses are shown in Table 1. At 3 weeks, high-dose indomethacin caused less chronic inflammatory changes than 50L/50D PLA-coated stents, whereas low-dose indomethacin caused slightly more chronic inflammatory changes than 50L/50D PLA-coated stents. Fibrosis was not found in the low-dose indomethacin group, whereas high-dose indomethacin caused slightly more fibrosis than 50L/50D PLA-coated stents. The amount of fibrosis with high-dose indomethacin was about the same as it was with pure PLGA stents. Both concentrations of indomethacin caused more calcification than control stents. Low-dose indomethacin had no effect on the amount of eosinophils, whereas in the high-dose indomethacin group, the amount of eosinophils was a bit higher than in the 50L/50D PLA-coated stents group but did not differ from the PLGA stent group. There were no acute inflammatory or foreign body reactions found at 3 weeks in any group.
Mean±standard error of the mean, n=3 (*n=2).
PLGA=copolymer of L-lactide and glycolide acid; PLA=polylactic acid.
At 3 months, the tissue reactions in all the stent groups were minimal. Both indomethacin stents caused slightly less chronic inflammatory changes and calcification compared with the control 50L/50D PLA-coated stents. Eosinophilia was a little more prominent in the low indomethacin stent group, but there were no reactions in any groups in acute inflammatory reactions, fibrosis, and foreign body reactions.
Discussion
Many techniques and procedures exist in the treatment of urethral strictures. The number of different techniques refers to the fact that none is really perfect and without its certain limitations. One of the basic ideas of a biodegradable urethral stent is to overcome the large scale of very serious problems that usually come with the need to remove the stent after it has fulfilled its purpose.
The preliminary results with biodegradable urethral stents in avoiding urethral stricture recurrence were promising. 5 As further studies were carried through, there came a sense of disappointment. 6 Long-term results with an increased number of patients did not confirm the preliminary optimistic outcome. Without a doubt, a significant problem was the unsatisfactory stent configuration of a helical spiral that caused large fragments to obstruct the urethra during degradation. At the same time, however, the problem of epithelial polyposis still existed. Our new generation stent was one of braided mesh configuration. 15 –17 The new stent overcame the earlier problem of migration and sudden breakdown of its configuration, but it was not preventing the recurrence of urethral strictures. The experience with Urolume® urethral stents showed that the cause of failure could be intrastent fibrosis and scarring development. 18
Using stents as drug delivery scaffolds to the specific site in the human body is a new and exciting area. Because the biodegradable stents per se, regardless of their structural configuration, were not capable of preventing epithelial polyposis and fibrosis formation, we developed a new drug-eluting urethral stent. As a primary potential drug to affect urethral stricture recurrence, we chose a well-known NSAID, indomethacin. An important aspect in the selection was also cost-effectiveness.
We started the project by evaluating whether indomethacin can be added into the stent coating in a manner that allows a proper release of the drug from the stent. Indomethacin was found to elute from the stent in two large peaks. The first elution burst was at the beginning and lasted less than 5 days; the second peak was between 30 and 60 days. The study demonstrated that it is possible to achieve sustained elution with indomethacin and that the drug elution profile can be tuned. 12
Our primary target in the present study was to evaluate the biocompatibility of the new indomethacin-eluting stent, and in this point we succeeded. Previously PLA-stent material and LPS have been shown to stimulate the production of inflammatory mediators in THP-1 macrophages. 19 Interestingly, in activated macrophages, indomethacin-releasing stent material and indomethacin itself inhibited the production of chemotactic and proinflammatory factors MCP-1 and RANTES, which are involved in leukocyte transmigration. MCP-1 and RANTES are chemokines that act by regulating the recruitment of inflammatory cells into tissue during inflammation. 20 In the in vivo experiments, the indomethacin-releasing stents showed comparable biocompatibility profile with the stents without drug-eluting properties. It is also important that in adding indomethacin-eluting coating, the degradation of the stent was not significantly affected, and we can still count the same degradation time.
Previously indomethacin was shown to decrease the development of fibrosis in a renal ischemia model. 21 In the present study, indomethacin did not inhibit TGF-β in vitro or effect the development of fibrosis. The lower polyposis rate seen in the indomethacin-eluting urethral stents is encouraging, but it is not clear whether the stents could prevent stricture formation in the urethra.
Because there are no previous works with indomethacin stents clinically, optimal drug doses need to be evaluated. In addition, the new stents need to be tested in urethral injury settings where the effectiveness of the drug-eluting property can truly be evaluated.
Conclusion
Our study demonstrated that indomethacin-eluting biodegradable urethral stents are highly biocompatible, and the new drug releasing property does not remarkably affect the degradation time of these stents. Epithelial polyposis can be potentially reduced by drug-eluting stents, but further studies are needed to evaluate whether it is possible to prevent urethral stricture formation with drug-eluting stents.
Footnotes
Acknowledgments
This study was financially supported by The National Technology Agency of Finland (TEKES) and the Competitive Research Funding of the Pirkanmaa Hospital District.
Disclosure Statement
No competing financial interests exist.