
Abstract
Purpose:
To evaluate the effectiveness of the portable laparoscopic trainer in improving skills in subjects who have had no previous laparoscopic experience.
Materials and Methods:
Twenty-nine medical students were given a pretest of three tasks on a standardized laparoscopic trainer. Subjects were evaluated objectively and subjectively. Fifteen subjects were randomized to receive a portable laparoscopic trainer and 14 subjects were assigned to the standardized laparoscopic trainers at our facility. The portable trainer group subjects were advised but not required to complete at least 3 hours of training. The group at the facility had a proctored 1-hour session each week for 3 weeks. Each subject was then retested and evaluated with the same pretest tasks. Objective and subjective improvements between the groups were compared.
Results:
Baseline demographics and pretest scores were similar between both groups. All students in the facility group completed the three 1-hour proctored sessions. The portable trainer group reported an average 204 minutes of practice. The facility group did objectively better on the post-test in overall time, and in two exercises. Subjectively, the facility group had a significant improvement compared with the portable trainer group (4.6 vs 2.4 point average increase, P=0.03).
Conclusions:
Both groups showed objective and subjective improvement after a 3-week period of training. The portable trainer group did report longer average practice time, but this made no significant difference in subjective or objective improvement. The portable laparoscopic trainer is comparable to the standard trainer for improvement of basic laparoscopic skills.
Introduction
Various simulators and standard trainers have been created to help physicians in this regard. These include models as simple as box trainers to complex virtual reality simulators. 2 A randomized study from Matsumoto and associates 3 showed that low fidelity models are just as effective as high fidelity models in improving endourologic skills and do so at a lower cost.
Several different portable Webcam and box trainers have been tested and validated in the past. 4 –6 Webcam trainers are convenient and can be used anywhere in contrast to the standard laparoscopic trainers and virtual reality trainers. In addition, they are relatively inexpensive, which makes it feasible for subjects to have their own trainer to use at their leisure. This makes it an ideal model for subjects who are novices in laparoscopy who may need extra practice in simple tasks.
We compared the effectiveness of improving laparoscopic skills between the TASKit (Ethicon Endo-surgery Inc.) portable Webcam trainer and the standard video laparoscopic trainer (Karl Storz Endoscopy) in surgical naïve subjects.
Materials and Methods
After Institutional Review Board approval and informed consent was obtained, we recruited 29 first- and second-year medical students to participate in the study. They were given a brief introduction to the use of the laparoscopic instruments and instructions on how to perform three tasks on a standardized laparoscopic trainer.
The first task was a peg transfer exercise in which subjects placed four pegs onto a designated diagonal line of a Peg-Board. The second task involved transferring a fuzzy ball under a plastic hoop between two instruments. The final task consisted of a rope exercise to simulate running the bowel laparoscopically. This involved transferring a 140-cm string at designated marks between two graspers from end to end (Fig. 1). Subjects were evaluated objectively (timed) and subjectively (1–5 point scale on four different parameters, Table 1). The subjective evaluators were not blinded to the groups. Once the pretest was completed, the subjects were asked to complete a survey regarding previous surgical experience, medical specialty interests, and the perceived difficulty of the tasks and use of laparoscopic instruments.

Pre-test and post-test tasks (peg transfer exercise, fuzzy ball exercise, and running the bowl exercise).
After the pretest and survey, medical students were randomized into two groups. Fourteen subjects were assigned to use the standardized laparoscopic trainers (Fig. 2) at the facility (group A). The remaining 15 subjects were randomized into the group who received a portable laparoscopic (TASKit) trainer (Fig. 3) to use at home (group B). The portable trainer group subjects were encouraged to practice at home as their schedules allowed with a suggested 3 hours of total practice time. They were given the equipment and instructions to practice the pretest tasks, as well as 10 additional practice exercises included with the kit.

Students practicing on standard laparoscopic trainers.
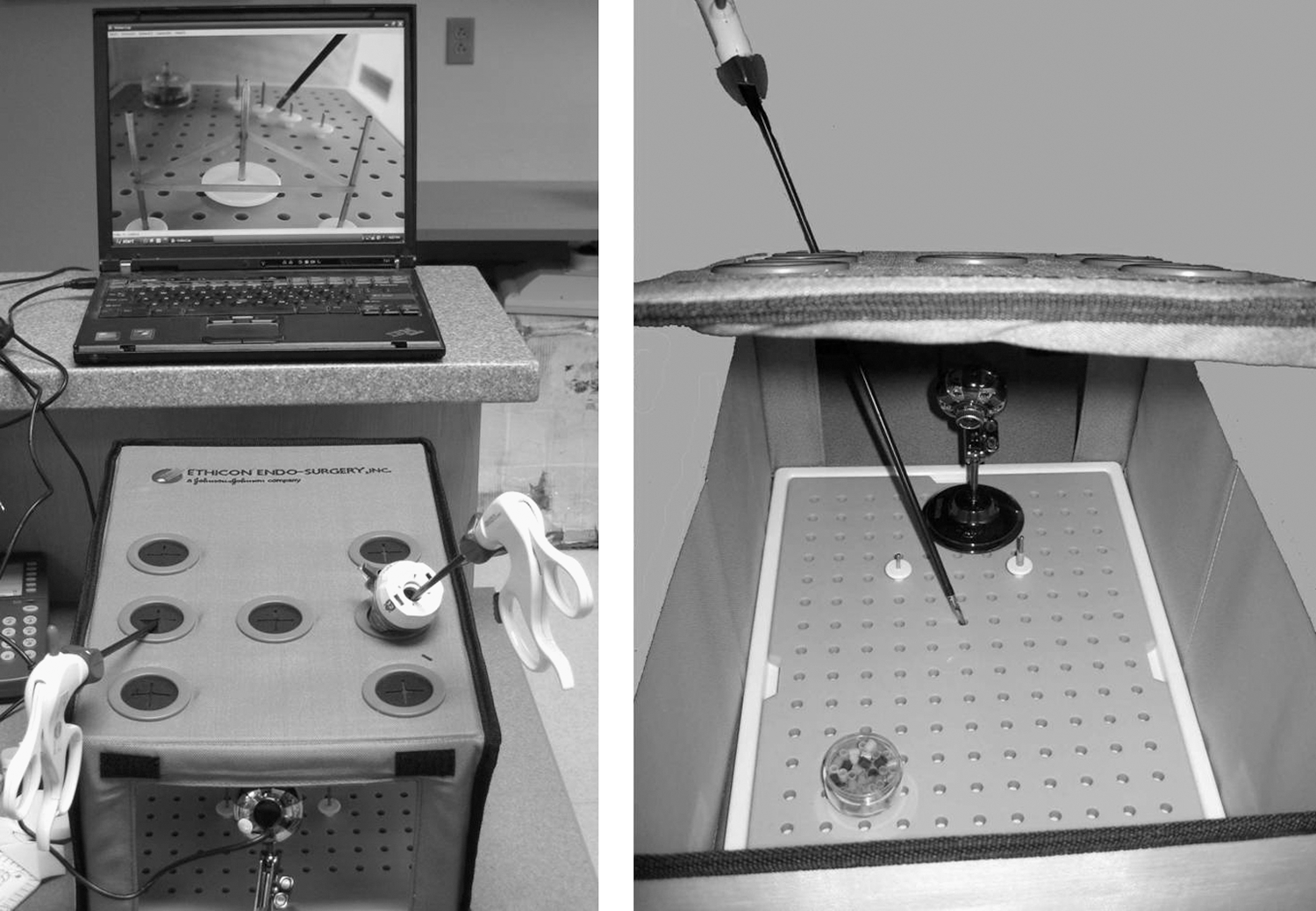
Portable laparoscopic trainer (TASKit).
The facility group attended a proctored 1-hour session every week for 3 weeks. The facility group also had access to practice on the portable laparoscopic trainer during their proctored sessions. Group A practiced the same tasks as group B and had two additional exercises they could practice that also focused on hand-eye coordination.
At the end of 3 weeks, each subject was then retested and evaluated with the same three tasks. Objective and subjective improvements between the groups were compared; hours of training and barriers to training were also compared. Statistical analysis was performed using the Fisher exact test for nominal variables and Wilcoxon rank-sum tests for continuous variables.
Results
There were 14 subjects in the standard laparoscopic trainer group (group A) and 15 subjects in the portable laparoscopic trainer group (group B). There were equal numbers of men and women in each group (Table 2). The average age of the portable trainer group was 26.4 years, whereas the average age of the facility group was 24.2 years (P=0.03). Overall, only one student had previous laparoscopic experience that involved holding the camera in one surgical case and was randomized into the facility group. His scores were not statistically better compared with the remaining students in his group. There were more second-year medical students in group B compared with group A. There were no other statistically significant differences in baseline demographics between the two groups (Table 2). There were no statistically significant differences in the pretest scoring between the two groups (Table 3).
Group A=standard laparoscopic trainer; group B=portable laparoscopic trainer.
Group A=standard laparoscopic trainer; group B=portable laparoscopic trainer.
All students in the facility group completed the three 1-hour proctored sessions. The portable trainer group had an average practice time of 204 total minutes (range 30–330 min), with the majority of time spent practicing in the week before the post-test (average 102 min). Eight students practiced for more than 180 minutes in the portable trainer group. Practicing longer than 180 minutes, however, resulted in no improvement both subjectively and objectively when these students were compared with those who practiced for 180 minutes or less (Table 4).
Group B=portable laparoscopic trainer.
Group A did statistically better than group B when comparing post-test peg and fuzzy ball exercise average times as well as the total post-test average times (Table 5). There was no statistically significant difference in objective improvement between the two groups. This is likely secondary to the fact that group B's initial pretest times were overall longer than group A (but not statistically significant). Therefore, although they had similar improvement, group A ended up with faster overall times on the post-test compared with group B. In regard to subjective scoring improvement, group A had a statistically significant improvement compared with group B (4.6 point average increase vs 2.4 point average increase, P=0.03). Group A also had better average scores on the post-test peg transfer test and greater overall score improvement.
Group A=standard laparoscopic trainer; group B=portable laparoscopic trainer.
Students who played at least 1 hour/week of video games had statistically faster average times in the pretest peg transfer exercise (108 sec vs 142 sec, P=0.02). They were also faster in the post-test fuzzy ball exercise (37 sec vs 48 sec, P=0.05). Previous musical instrument use and participation in sports showed no statistically significant difference in performance both subjectively and objectively.
Sixty-four percent (9/14) of the students in group A and 73% (11/15) of the students in group B had an interest in surgery at the time of the pretest. Three students in group A and six students in group B became more interested in surgery at the completion of the study. Forty-three percent (6/14) of group A thought that the portable laparoscopic trainer group had the advantage in the study. Only 27% (4/15) of the subjects thought the same about group B. The primary barriers to training at home, as reported by group B participants, were time management and boredom with the tasks.
Table 6 highlights the anonymous subjects' responses to the difficulty of the tasks and ease of use of the instruments. Interestingly, although group A did subjectively and objectively better on most of the post-tests, they thought that the tasks and use of the instruments were more difficult after the completion of the study.
Group A=standard laparoscopic trainer; group B=portable laparoscopic trainer.
Discussion
Learning and mastering laparoscopic skills is essential for any surgical resident. Teaching residents in the operating room, however, is expensive and inefficient. A study done by Bridges and Diamond 7 estimated the annual cost of training residents in the operating room to be $53 million. Therefore, many efforts are being made to teach and prepare residents outside the operating room to reduce this burden. Because of the steep learning curve, laparoscopic skills laboratories are becoming an integral part of surgical training.
Numerous studies have demonstrated that subjects who participate in laparoscopic skills laboratories improve their performances in the operating room. 2 With more stringent restrictions on working hours, taking time away from the operating room to participate in these laboratories becomes difficult for surgical residents. A study by Chang and colleagues 8 found that residents chose not to participate in a simulation laboratory partly because of time and location. The residents need a way to practice and improve their skills outside of the operating room and outside of the workplace. These two constraints make portable at-home trainers the ideal solution. Previous randomized trials found that portable at-home trainers are just as effective as the standardized facility trainers in improving performance. 4,5 In addition, portable laparoscopic trainers are inexpensive and some can even be homemade. 6,9 Our study is the first to investigate and validate the TASKit trainer as another low-cost alternative for laparoscopic training.
Most of the aforementioned studies used subjects with previous laparoscopic experience (residents, surgeons, physicians, etc.). Chandrasekerea and associates 10 compared the standard pelvic trainer to a simple cardboard box model in medical students and found they were both effective in improving laparoscopic skill performance. Our study also focused on medical students with no previous surgical experience.
Hagen and coworkers 11 surveyed a group of general surgery residents and found that laparoscopic simulators were beneficial and those who had an opportunity to train with simulators had overall better performance during skills testing. This was consistent with what was noted in our study. Both groups had improved performance even after a short 3-week training period. Will this improved performance on inanimate models translate to improvement in the operating room for surgical residents? Scott and associates 12 addressed this question in a randomized trial of surgical residents. The group who completed 10 days of 30-minute training exercises had improved performances both on the video trainer tasks as well as in the operating room. On the other hand, Traxer and colleagues 13 found that there was no difference in performance of a porcine laparoscopic nephrectomy between those who underwent a 10-day (30 min/d) course of inanimate skills training compared with controls.
The inferior subjective performance of the portable laparoscopic trainer group reinforces the importance of supervision and feedback. Junior residents and laparoscopic naïve subjects should first learn in the presence of professional experienced instructors before practicing on their own. Proficiency targets have been found to be beneficial in improving performance in other studies. Gauger and coworkers 14 compared a group of surgical interns training on a laparoscopic simulation trainer with and without proficiency targets. They found that it not only improved practice and task performance but also improved operating room performance as well.
Another way to provide proficiency targets and objective feedback is through the use of a virtual reality simulator. 2 Hamilton and associates 15 compared two groups of residents who underwent a 2-week course (ten 30-min sessions) of training on a standard trainer vs a virtual reality trainer. There was no overall objective difference in their task performances at the end of the study; however, the virtual reality group performed better in the operating room. Subjects in Hamilton's study and other studies have shown that participants prefer the standard box trainers over the virtual reality simulators. 15 –17 Virtual reality trainers are more expensive and less accessible than the inanimate trainers.
Regardless of the type of laparoscopic trainer available, motivating students and residents to practice can prove to be difficult. In our study, the medical students who took the trainers home found that time management and boredom with the tasks were the two major barriers to practice. The inanimate trainers are designed to develop hand-eye coordination and familiarize the trainee with use of the instruments. 18 They are not effective, however, in simulating dissection or higher level tasks that become more important for more advanced trainees.
Now that we have validated the portable laparoscopic trainer, our future studies will focus on tackling some of these issues with the inanimate trainer. We hope to create exercises that generate more interest in use of the trainer as well as simulate important steps of laparoscopic surgeries. Some ideas to increase interest include surgical scenarios, competition with classmates, and more advanced tasks. As far as time management is concerned, it will be difficult to combat the human nature to procrastinate. Weekly checkpoints or incentives, however, may improve consistency of training. Further investigation is necessary to examine these two constraints to portable training.
As other studies have shown, we found that previous experience with video games impacted a subject's performance in laparoscopic skills. Rosenberg and colleagues 19 found that video game ability predicted the level of laparoscopic skills in novice subjects. Grantcharov and coworkers 20 also found that those who played computer games made fewer errors on a virtual reality simulator compared with nonusers. Madan and associates 21 looked at medical students' performances on both a box trainer and virtual reality trainer. They found that computer game experience, typing, use of chopsticks, and musical instruments had no impact on predicting performance on the box trainer but did impact the virtual reality trainer scores. Our study also found that previous musical instrument use and participation in sports did not impact overall performance in laparoscopic skills.
Based on our survey data, exposure to laparoscopic skills laboratories has a positive impact on student interest in surgery. This is important, because there is evidence suggesting that the total number and quality of surgical residency applicants is declining. 22 As medical students choose their careers, early exposure to laparoscopic skills labs, whether through facility or portable trainers, may increase their interest in surgery. This suggests that studies similar to ours may help generate interest and maintain a high quality applicant pool in all fields of surgery.
One of the weaknesses of the study was that the evaluators were not blinded to which group the subject was in. This could have affected their subjective scoring. In addition, the facility group may have had an advantage because they trained on the standard laparoscopic trainer, which was also used for pre- and post-testing. This variable could have been eliminated if we had the subjects perform a pretest and post-test both on the portable trainer as well as the standard trainer. It would have also been beneficial to have an additional control group that did not have any practice; however, recruitment was difficult, and this would have lowered the number of subjects in each group.
Conclusion
After 3 weeks of training, both groups showed objective and subjective improvement. The portable trainer group reported longer average practice time than the facility group, but despite this, had less subjective improvement compared with the facility group. Overall, our results suggest that practice on the TASKit portable laparoscopic trainer improves skills performance among surgically naïve subjects and is comparable to the standard laparoscopic trainer. Continued research is necessary to create tasks that will keep students motivated and to establish proficiency targets.
Footnotes
Acknowledgments
We wish to thank Dr. Richard Schlinkert, Dr. Richard Gray, Dr. Kristi Harold, and Denise Schlinkert for their assistance in the use of the laparoscopic skills laboratory.
All laparoscopic portable trainers were provided by Ethicon Endosurgery Inc. Funding for this study was provided by the Multidisciplinary Simulation Center at the Mayo Clinic Arizona.
Disclosure Statement
Dr. Humphreys is a consultant/advisor for Boston Scientific Inc., and Lumenis Inc. Dr. Castle is a consultant for Baxter and a lecturer for Intuitive Surgical. For the remaining authors, no competing financial interests exist.