
Abstract
Background and Purpose:
Renal cryoablation has gained popularity as a treatment option for localized renal masses. Treatment success is typically defined by the absence of contrast enhancement on follow-up imaging. We investigate the evolution of lesions that demonstrate contrast enhancement on CT after renal cryoablation.
Patients and Methods:
Retrospective review of records of laparoscopic and percutaneous cryoablation (LCA and PCA) was performed, identifying records with postoperative radiographic enhancement. Imaging studies were reviewed and radiographic (pre- and post-contrast Hounsfield units, pattern and location of enhancement) and clinical data including follow up were collected.
Results:
One hundred and seventy-two cryoablation procedures were analyzed. Of these, 30 (17.4%) showed enhancement on follow-up CT. In 28 cases, contrast enhancement was demonstrated on the first postoperative study. Seven patients underwent salvage treatments. Spontaneous resolution of enhancement was noted in 17 (56.7%) cases. No association was found between enhancement pattern (diffuse/nodular/rim) and resolution. Of lesions enhancing >35 HU, only 14.3% resolved spontaneously. Delayed enhancement (after negative imaging studies) occurred in two patients; both underwent salvage treatments.
Conclusions:
Most of the time, contrast-enhancements after cryoablation are evident on the first follow-up imaging study. More than 50% of these resolve spontaneously, and only one of four patients need salvage treatment. Delayed appearance of enhancement after previously negative imaging and highly enhancing lesions (>35 HU) are unlikely to resolve and should be considered suspicious for local recurrence or incomplete ablation. Further investigation is warranted to reach a consensus on a radiographic definition of local recurrence after renal cryoablation.
Introduction
Despite the rising popularity, there are little data regarding the oncologic outcomes of cryoablation. Moreover, there is no consensus on the definition of treatment failure with many authors using absence of contrast enhancement and decrease in size of the ablation site as a surrogate to define treatment success. While in line with pathologic validation, 3 this definition does not address the cases with evidence of postoperative enhancement on CT, whereas a decrease in size is of difficult interpretation 4 considering the slow growth rates of renal tumors and interobserver variability. Although postoperative contrast enhancement at the cryoablation site is a worrisome finding, it does not necessarily represent treatment failure, 5 because biopsy confirms viable cancer cells in fewer than 40% of these cases. 3
A postcryoablation CT demonstrating contrast enhancement at the treated site often prompts intensified follow-up imaging, percutaneous biopsy, or defines treatment failure necessitating outright salvage therapy. Little is known regarding the evolution of these enhancing foci after ablation. The purpose of the present study was to evaluate the imaging characteristics and the outcomes of renal lesions demonstrating contrast enhancement on CT after cryoablation.
Patients and Methods
A retrospective search of our prospectively maintained electronic database was performed to collect consecutive LCA and PCA procedures that were performed between 2001 and 2009. We excluded records with no contrast-enhanced CT imaging follow-up available. Cases with CT evidence of contrast enhancement at the ablation site were identified. All CT studies were performed at our institution using multidetector scanners, 120–140 kVp with mAs adjusted for body size, and with 5-mm thick sections reconstructed at 5-mm intervals. Imaging studies were reviewed by a board-certified radiologist (CYK) for characterization of the enhancing lesions.
The pre- and postcontrast attenuation of the lesion was measured in Hounsfield units (HU), with significant enhancement defined as ≥10 HU. The morphology of the enhancing lesion was characterized as diffuse or focal enhancement, the latter including circumferential rim enhancement and focal nodular enhancement (Fig. 1). The maximum axial dimension was recorded for diffuse and nodular enhancing lesions; the maximum thickness was recorded for rim-enhancing lesions. For focal enhancements, the location in relation to the ablation site was characterized as deep or peripheral.
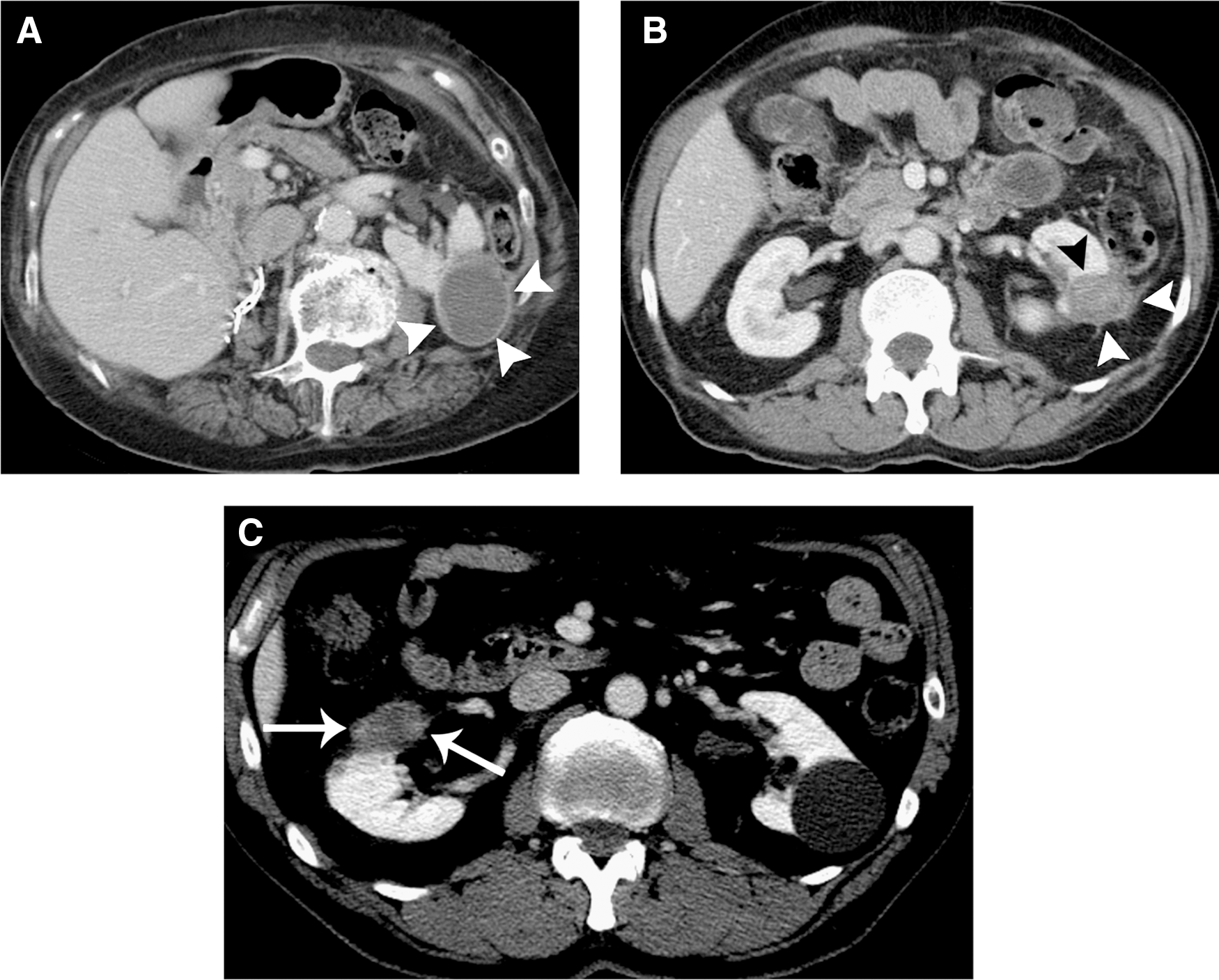
CT enhancement patterns after cryoablation.
Follow-up radiographic and clinical data were reviewed to document treatment and imaging evolution of the enhancing lesions. Specifically, we defined these enhancing lesions as resolved (no enhancement on follow-up imaging studies), stable (comparable or decreased enhancement with no increase in size), or salvaged if there was need for there was need for additional treatment not meeting the above criteria or according to patient preference.
Our cryoablation techniques have been previously described. 6 Briefly, for LCA, a standard transperitoneal approach is used, the lesion is identified, and under intraoperative ultrasonographic guidance, the cryoprobes are placed for a dual freeze/thaw cycle. For PCA, a pretreatment CT is obtained for procedure planning and, under moderate conscious sedation and local anesthesia, the probes are placed under low-mA-CT-fluoroscopy for a dual freeze/thaw cycle. With either technique, a 5 to 10-mm rim of normal parenchyma surrounding the tumor was ablated to achieve the equivalent of a surgical margin. Third generation cryotechnology was used. Routine contrast-enhanced CT imaging follow-up was scheduled every 6 months in the first year for LCA patients; for PCA patients, imaging follow-up was scheduled every 3 months for the first year. A yearly imaging surveillance schedule was undertaken after 12 months.
For comparisons, we used chi-square and rank sum tests as appropriate. P values < 0.05 were considered significant. Data are reported as median (interquartile range, [IQR]) or number (%) unless otherwise specified. All analyses were performed using the SPSS v17 software (SPSS Inc, Chicago, IL). This study was approved by the Institutional Review Board.
Results
A total of 195 cryoablation procedures were performed including 72 LCA and 123 PCA. In 23 cases, there was no contrast-enhanced follow-up imaging available for review, and they were excluded from the present analysis. Of the remaining 172 procedures, 30 (17.4%, 8 [11.1%] LCA and 22 [17.9%] PCA) had evidence of contrast enhancement on follow-up CT. In this study cohort, the median age of the patients was 65 years (57–73), 25 (83.3%) were Caucasian, and 14 (46.7%) were males. Primary tumor size was 2.1 cm (1.7–2.7) and in four (13.3%) patients, multiple tumors were treated simultaneously. Over a median follow-up of 11.6 months (6.4–24.5), there were no disease progressions.
Imaging characteristics on CT including enhancement morphology are detailed in Table 1. CT evidence of contrast enhancement was detected at a median of 3.1 months (IQR 2.8–5.9) after the procedure. In the vast majority of patients with evidence of postablation enhancement (n=28, 93.3%), this was identified on the first postoperative imaging study. In two cases, contrast enhancement was noted after 39 and 50 months of uneventful follow-up, respectively. One patient elected to undergo a radical nephrectomy revealing oncocytoma (original biopsy suggested an oncocytic lesion) whereas another patient chose PCA; in both cases, there is no evidence of recurrence or progression to date.
LCA=laparoscopic cryoablation; PCA=percutaneous cryoablation; IQR=interquartile range; HU=Hounsfield units.
A total of seven (23.3%) patients underwent salvage treatments including PCA (n=6) and surgical extirpation (n=1) based on physician and patient preferences. The remaining 23 patients are being followed with stable (n=6) or resolved (n=17) foci. Contrast enhancement on CT resolved spontaneously on subsequent imaging in 17 patients with similar proportions between diffuse (12/20, 60%) and focal enhancing foci (5/10, 50%). Interestingly, none of the four patients with evidence of rim enhancement needed salvage treatment; in two patients, enhancement spontaneously resolved, and in two, stable enhancement is undergoing surveillance.
When stratified by enhancement morphology (diffuse vs focal), we noted differences in the enhancement patterns whereby both pre- and postcontrast attenuation of the lesion were higher in the focal enhancing lesions (33.0 vs 39.0 HU, P=0.008 and 54.5 vs 69.5 HU, P=0.044, respectively). The degree of enhancement, however, was similar between the groups (23 vs 26 HU, P=0.502).
Stratified by contrast enhancement, only one of seven lesions enhancing >35 HU had a spontaneous resolution, whereas 16 of the remaining 23 lesions with lower enhancement values resolved (P=0.025). On multivariate analysis adjusted for age, race, and sex, however, we found no significant association between spontaneous resolution and lesion morphology, enhancement degree, or time from surgery to evidence of enhancement.
Discussion
Cryoablation is a recognized and effective treatment option for localized renal tumors. Local recurrence remains a concern and its radiographic definition lacks consensus. While no radiographic enhancement of the treated lesion represents a favorable outcome, little is known about persistent contrast enhancement after cryoablation. In the present study, we investigated the outcomes of cryoablation sites that demonstrate contrast enhancement on follow-up CT imaging in a large single institution series of LCA and PCA.
Although some authors use postcryoablation biopsy to determine treatment success, this approach is not common and remains controversial. 3,7,8 Several radiographic definitions of local recurrence or incomplete ablation have been used in the literature, and they rely on contrast enhancement and lesion growth. 8 –14 Contrary to radiofrequency ablation, cryoablation success correlates well with imaging findings. 3 Evidence of contrast enhancement postcryoablation has been considered a criterion for intensified imaging follow-up, biopsy, or surgical exploration of the ablated site. 3,12 Contrast enhancement by itself, however, may not be representative of residual cancer, 5 and an aggressive approach to postcryoablation enhancement may not be necessary in all cases.
There is no agreement on what enhancement should be defined as significant in the setting of follow-up after cryoablation. Although a 15 to 20 HU cutoff has been proposed to characterize renal masses by CT, 15 this proposal is not widely agreed on, and we believe that after treatment of a renal mass, the threshold of suspicion should be lowered. Hence, we chose to use the cutoff of ≥10 HU to define significant enhancement.
Contrast enhancement after cryoablation may indicate a number of underlying processes. First, and most worrisome, viable cancer can be the cause of increased vascularity reflected by contrast enhancement. Second, increased vascularity is a typical feature of granulation tissue and the normal healing process at the ablated site, which can manifest as contrast enhancement. Finally, pseudoenhancement and other technical issues (such as partial volume averaging) may be responsible for apparent contrast enhancement 16 at the ablated site. An optimally executed imaging study and experienced abdominal radiologists are critical to avoid these pitfalls.
In the vast majority of cases (93.3%) with evidence of postablation enhancement, it was identified on the first follow-up imaging study, whereas in two (6.7%) cases, an enhancing lesion appeared after 3 and 4 years of negative follow-up. This finding suggests that a negative (no contrast enhancement) first follow-up imaging study should be considered reassuring and the subsequent imaging schedule can be safely stretched out at longer intervals, thus reducing radiation exposure and avoiding excessive costs. A once yearly schedule may be sufficient after a first negative scan. Because late recurrences can occur years after treatment imaging, however, follow-up is needed and can be similar to that after extirpative nephron-sparing surgery.
Overall incidence of CT enhancement after renal cryoablation was 17.4%. Albeit these rates may appear higher than those generally reported in the literature, this is likely because of different study designs (eg, review of imaging studies) on one hand and the specific focus on contrast enhancement in our study on the other. Beemster and associates 8 evaluated enhancement patterns after cryoablation in 26 patients and found 1 incomplete ablation and 5 postablation enhancements, comparable to the rates of enhancement found in the present analysis. Yoost and colleagues 17 performed imaging review in their series of LCA and found a 17% failure rate, defined as persistent enhancement and/or no decrease in size of the cryolesion. Contrast enhancement on CT was evident more frequently in PCA patients (17.9%) compared with LCA (11.1%). While this finding is not dissimilar from previously reported data, 12 it may be potentially explained by the different imaging follow-up schemes whereby LCA patients underwent the first routine postoperative imaging at 6 months and PCA after 3 months. This finding suggests that earlier follow-up imaging may have a higher chance of demonstrating contrast enhancement, which will spontaneously resolve upon further follow-up imaging. This phenomenon may reflect granulation tissue and inflammation that could account for the enhancement. Delaying the first postoperative imaging may reduce the incidence of these “incidental” enhancements as well as costs and radiation exposure. We therefore recommend an initial routine follow-up imaging to be performed at least 6 months after cryoablation.
Of 30 cases with postablation enhancement, 7 underwent salvage treatments (6 repeated PCA) for an overall re-treatment rate of 4.1%, which favorably compares with the current literature. These cryoablation failures were managed with a nephron-sparing approach and in a minimally invasive manner in the present series, indicating the feasibility of repeated cyoablation. In the absence of large-scale consensus on the definition of residual/recurrent disease after cryoablation or its management (specifically there is no indication for the role of biopsy in this setting), the decision to treat was based on the current knowledge, and physician and patient preferences.
The gap between 17.4% of postablation enhancement and 4.1% re-treatment rate is bridged by two categories of enhancing lesions: The ones that resolved on follow-up imaging and the ones that remain stable without imaging evidence of evolution (increased degree of enhancement or enlargement). These postoperative findings are of most interest because little is known about their evolution over time and their management is controversial. Our results show that more than one-half of enhancing lesions spontaneously resolve on subsequent imaging. Similar findings were reported by Beemster and coworkers 8 whereby most initial enhancements resolved on subsequent imaging. We found that lesions enhancing >35 HU and enhancing lesions that appeared after a negative imaging follow-up are unlikely to resolve. These lesions would benefit from an intensified imaging follow-up and prompt re-treatment if imaging evolution (increased enhancement, increase in size) is noted.
The second category (stable enhancing lesions) remains of uncertain nature. At our institution these lesions are currently being carefully followed; we will be able to report their clinical course once follow-up matures. We did not find an association between the type or morphology of the enhancement and its tendency to spontaneously resolve. Diffuse as well as focal (both nodular and rim) enhancing lesions appear to have comparable rates of resolution. We did note that none of the rim enhancements needed re-treatment, and this category needes further investigation
Based on our results, we suggest customizing the early imaging follow-up protocol after renal cryoablation (Fig. 2). Specifically, we propose that patients with no evidence of enhancement on the first imaging study (at 3–6 months) embark on a longer interval between imaging approximating the schedules adopted for partial nephrectomy patients. This would obviate the need for frequent contrast-enhanced CT scans in the first year, reducing radiation exposure to the patient as well as healthcare cost, without reducing the efficacy of surveillance.

The proposed algorithm outline for imaging surveillance after renal cryoablation. NSS=nephron-sparing surgery.
On the other hand, monitoring of indeterminate enhancing lesions (that are not clearly missed tumors) should be frequent to promptly detect signs of evolution (increase in enhancement, enlargement, and/or changes in the morphology of the lesions). We propose repeated imaging in 3 to 6 months to monitor the evolution of the enhancing site. A biopsy of the enhancing area could be added to the algorithm when deemed necessary for evolving lesions whereby its results could impact the treatment of the patient.
An aggressive approach to re-treat any enhancing area after cryoablation, except for indisputably missed tumor, seems to be inappropriate because more than 50% of these will spontaneously resolve. Further investigation is needed to reach a consensus on the most appropriate individualized follow-up regimen and uniform reporting of the outcomes of renal cryoablation.
The results of our study should be interpreted in light of limitations inherent to the retrospective, single center design. Moreover, we lack pathologic data in the percutaneous cohort and therefore cannot elucidate the relations between imaging findings and the biology of the renal mass. This makes it impossible to us to discern true cancer recurrences from imaging evidence of persistent/recurrent benign pathology. Moreover, the limited sample size resulted in reduced statistical power of the multivariable analyses. Finally, longer follow-up is needed to address the course of stable enhancing lesions correlating to primary pathologic data.
Conclusions
In this series, contrast enhancement on CT at the cryoablation site was not infrequent and was evident in many cases on the first follow-up imaging study. More than 50% of these spontaneously resolve on subsequent imaging studies, however, and only one of four ultimately need salvage treatment. Delayed appearance of enhancement after negative follow-up imaging as well as highly enhancing lesions (>35 HU) are unlikely to resolve spontaneously and therefore should be considered suspicious for local recurrence or incomplete ablation. Rim enhancement appears to have a benign evolution because none of those were re-treated in this series. Further investigation is warranted to reach a consensus on a radiographic definition of local recurrence after renal cryoablation.
Footnotes
Acknowledgment
Presented in part at the 2010 World Congress of Endourology and SWL, Chicago, IL.
Disclosure Statement
No competing financial interests exist.