
Abstract
One of the most difficult, time-consuming, and at the same time critical steps of laparoscopic pyeloplasty is ureteral spatulation. We describe a reproducible technique that greatly simplifies this surgical step. Using standard laparoscopic scissors, the ureter is partially cut just inferior to the ureteropelvic junction (UPJ) at a point where a normal (nonstenotic) ureter is discerned. This first cut involves only half of the circumference of the ureter. The ureter remains attached to the UPJ. Through the most cephalad port, a 5-mm articulating laparoscopic scissors is inserted in the abdomen. The instrument is fully articulated so that the axis of the jaws is almost in line with the ureteral axis. The jaws are opened, one jaw is inserted in the ureteral lumen, and the ureter is spatulated to the requisite length. At this point, the first apical ureteral stitch is placed outside-in while the ureter is stabilized by its remaining attachment to the UPJ. Subsequently, the ureter is freed completely from the UPJ; the UPJ is excised, and the rest of the procedure is performed in a standard fashion.
Introduction
In our own practice, we have tried multiple modifications to overcome this steep part of the procedure. We have finally developed a reproducible technique that greatly simplifies this surgical step and can easily be adopted, even by inexperienced surgeons performing the procedure.
Technique
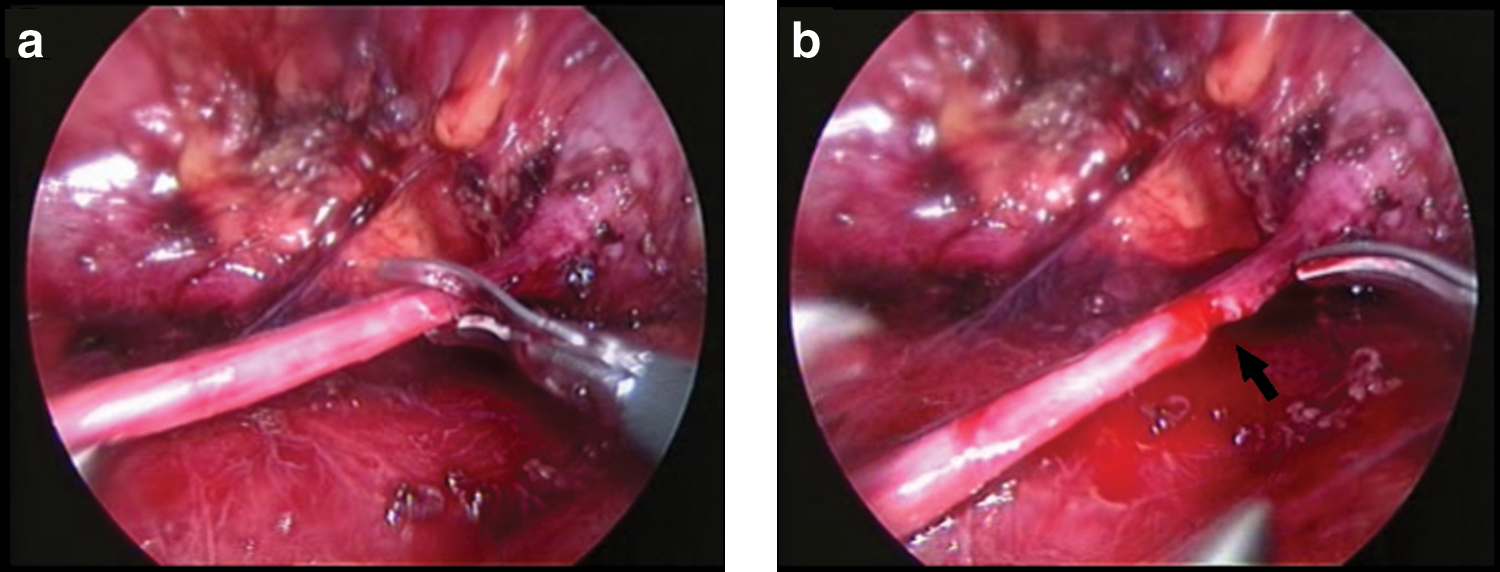
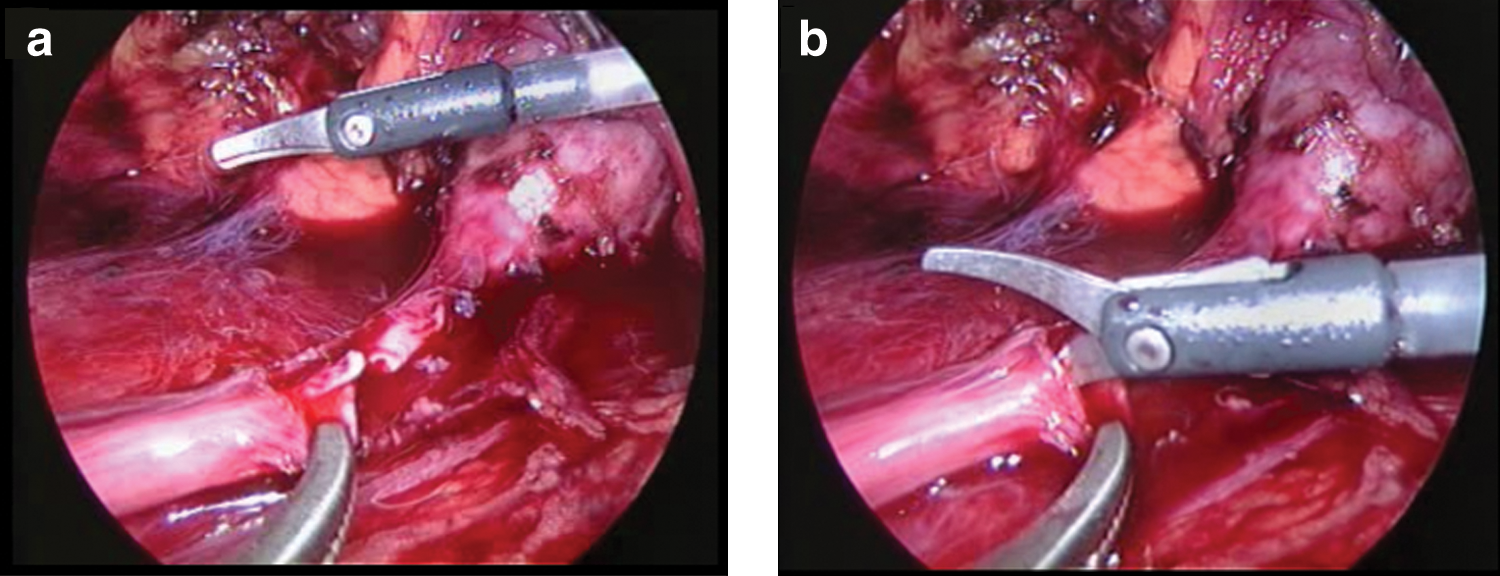
The patient is placed in a 60-degree modified lateral decubitus position with the affected side up. All pressure points are padded, and the table remains flat, without flexion. We use the transperitoneal approach, typically arranging the trocars as shown in Figure 1. The 5-mm trocar in the middle auxiliary line at the level of the umbilicus is placed, if necessary, either for liver retraction on the right side or for insertion of an additional grasper. The colon is mobilized medially by incising the line of Toldt. The proximal ureter is identified and is carefully dissected up to the renal pelvis. After complete mobilization of the UPJ, the following surgical steps are used: 1. Using standard laparoscopic scissors, the ureter is partially cut just inferior to the UPJ at a point where the normal (nonstenotic) ureter is discerned. This first cut involves only half of the circumference of the ureter. The ureter is still attached to the UPJ (Fig. 2). 2. Through the most cephalad port, a 5-mm articulating laparoscopic scissors (Covidien, Norwalk, CT) (Fig. 3) is inserted in the abdomen. The instrument is fully articulated (approximately 80 degrees) so that the axis of the jaws is in line with the ureteral axis. The jaws are opened; one jaw is inserted in the ureteral lumen, and the ureter is spatulated at its lateral aspect to an adequate length (Fig. 4). 3. At this point, the first apical ureteral stitch is placed outside-in. The needle holder is inserted through the most inferior trocar. The spatulated ureter is stabilized by its remaining attachment to the UPJ, which greatly facilitates this step. A 4-0 polyglactin suture on the RB1 needle is used (Fig. 5). 4. The remaining ureteral attachment is cut, freeing the ureter completely. The UPJ is excised, cutting the renal pelvis in an oblique fashion from superior medial to inferior lateral. If deemed appropriate, the renal pelvis can be reduced at this point. 5. The posterior wall of the anastomosis is done first using free-needle suturing. We prefer interrupted sutures. One can run the initially placed stitch to complete the posterior anastomosis, however. After completion of the posterior wall, a pigtail stent is placed in an antegrade fashion. Subsequently, the anterior wall is addressed, which completes the procedure.

Trocar configuration for right-side transperitoneal laparoscopic pyeloplasty. The same configuration in the mirror image is used for a left-side reconstruction. (●) camera port; (▴) 10-mm port; (♦) 5-mm port; (▪) optional 5-mm port.
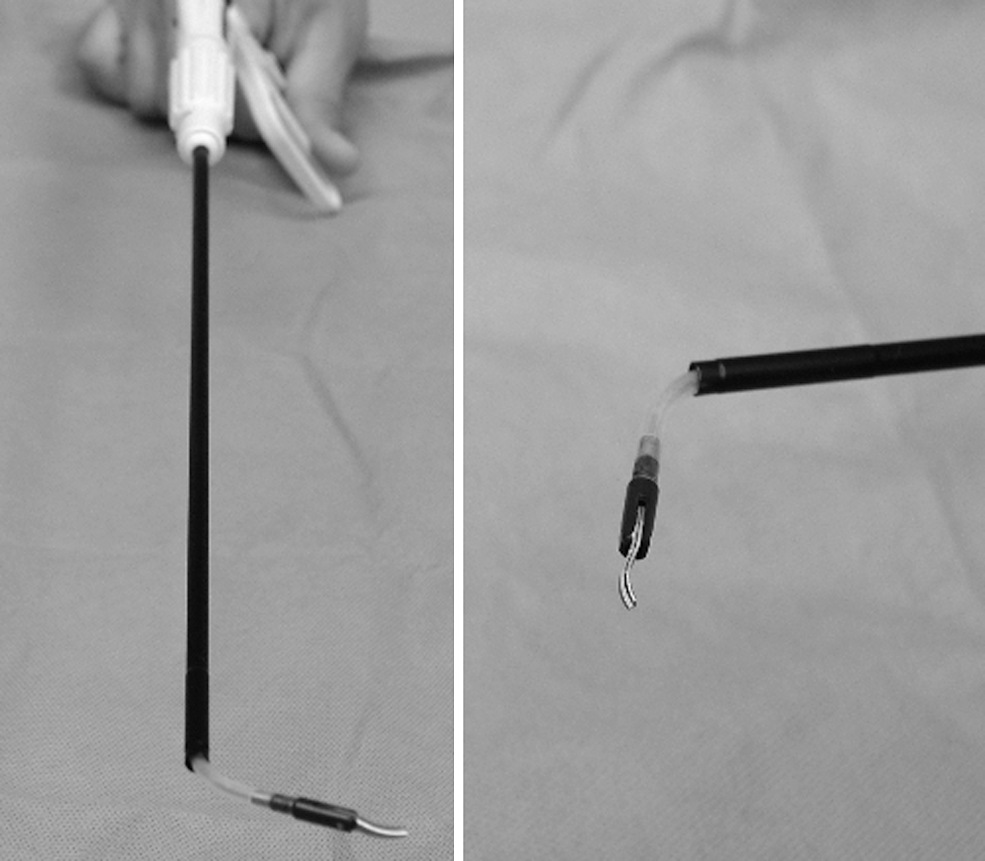
A 5-mm articulating laparoscopic scissors. The instrument is shown with its tip at maximum articulation (approximately 80 degrees).
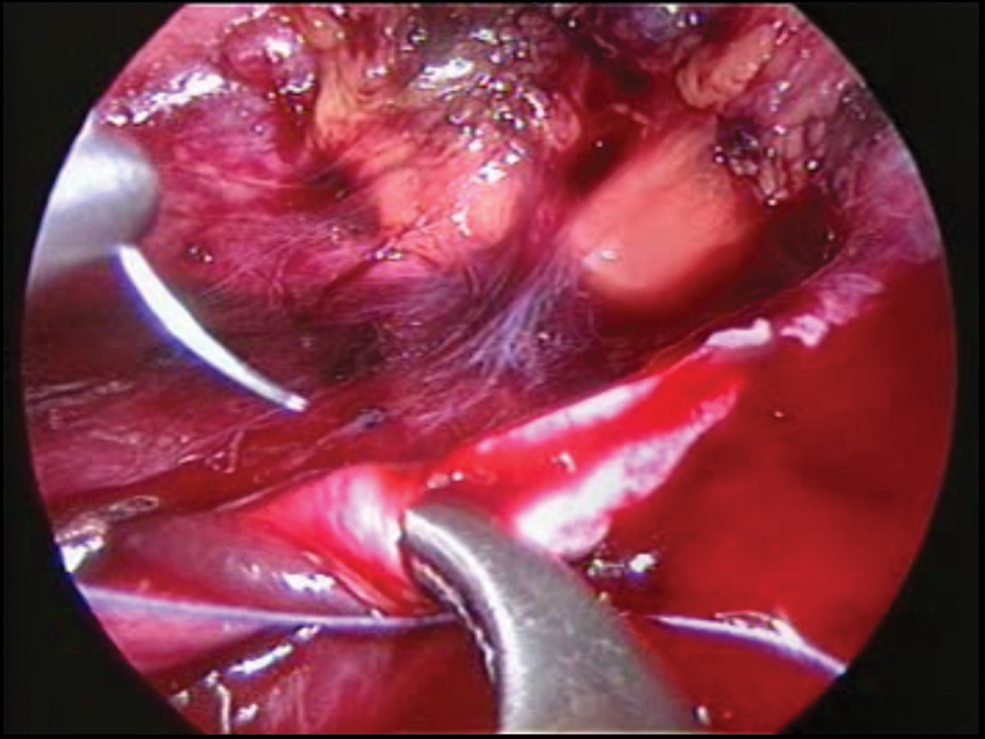
The first apical ureteral suture is placed outside-in before cutting the remaining ureteral wall. The needle holder is inserted through the most inferior trocar. The spatulated ureter is stabilized by its remaining attachment to the ureteropelvic junction.
Discussion
The key point of our technique is the use of the articulating scissors. The main advantages include an incision created with the jaws of the scissors in line with the ureteral axis while the ureter is still attached to its original anatomic position. Therefore, the ureter cannot be twisted; the incision is performed precisely and easily because the ureter is stabilized, avoiding spiraling of the cut. Technically, if the angles allow, lateral spatulation of the ureter can be performed after completing the anterior pyelotomy using standard laparoscopic scissors. 1 Unfortunately, in our experience, this is not the case in a significant number of patients. In these cases where optimal angles cannot be reached, ureteral spatulation can be quite difficult or even impossible with standard laparoscopic scissors, unless dismemberment has already been completed. Freeing the ureter completely, however, makes the subsequent steps of spatulation and apical stitch placement significantly more difficult and cumbersome.
With the technique we describe, favorable angles can always be produced by appropriate articulation of the instrument tip, obviating the need for early dismemberment. Therefore, the ureter is not freed from the UPJ until the first apical suture has been placed, again with the ureter stabilized and lying at its normal anatomic position. Both spatulation and apical suture placement are performed with minimal ureteral grasping and manipulation, thus minimizing ureteral trauma.
It is also noteworthy that these time-consuming steps of laparoscopic pyeloplasty can be achieved within a few minutes by the surgeon alone, without any help from the assistant. There is no need for stay sutures in the ureter, and we have never used stay sutures for the pelvis, although the latter can be used, if necessary. Practically, use of the articulating scissors for this step of the procedure mimics the robotic arm during robot-assisted pyeloplasty, yielding additional degrees of freedom for ureteral spatulation.
There are two main drawbacks to this technique. The first is that the stent should not already be in place; otherwise, it may be inadvertently sectioned during the initial cut of the ureteral wall. The stent should be placed later either in an antegrade fashion, as we usually do, or in a retrograde fashion using a variety of techniques. 3 The second drawback is that because the initial partial cut is made inferior to the UPJ, the surgeon must pay special attention not to cut too far distally; otherwise, tension may be encountered during the subsequent reconstruction. In this case, further mobilization of the ureter and the pelvis will solve the problem.
One can also avoid tension in the anastomosis by minimal reduction of the renal pelvic wall. We had no problem in performing a tension-free ureteropelvic anastomosis, despite the fact that we routinely discard the dysfunctional ureteral segment of the UPJ. The same technique can also be used for ureteral spatulation through the UPJ, maintaining the entire ureteral length and incorporating it in the subsequent reconstruction.
Footnotes
Disclosure Statement
No competing financial interests exist.