
Abstract
Prostatic neuroanatomy is difficult to visualize intraoperatively and can be extremely variable. Damage to these nerves during prostatectomies may lead to postoperative complications such as erectile dysfunction and incontinence. This review aims to discuss the prostatic neuroanatomy, sites of potential nerve damage during a prostatectomy, and nerve-mapping technologies being developed to prevent neural injury. These technologies include stimulation, dyes, and direct visualization. Nerve stimulation works by testing an area and observing a physiologic response but is limited by the long half-life for an erectile response; examples include CaverMap, ProPep, and optical nerve stimulation. Few nerve dyes have been approved by the Food and Drug Administration (FDA) because of the extensive testing required; examples of nerve dyes include compounds from Avelas and General Electric, fluorescent cholera toxin subunit B, indocyanine green, fluorescent inactivated herpes simplex 2, and Fluoro-Gold. Direct visualization techniques have a simpler FDA approval process; examples include optical coherence tomography, multiphoton microscopy, ultrasound, coherent anti-Stokes Raman scattering. Many researchers are developing several novel technologies that can be categorized as stimulation based, dye-based, or direct visualization. As of yet, none has shown clear evidence to improve surgical outcomes and consequently lack wide adoption. Further development of these technologies may lead to improved complication rates after prostatectomies. Clinically, some technologies have demonstrated utility in predicting the development of complications. By using that information, more aggressive rehabilitation programs may lead to improved long-term function. These technologies can also be applied for research to improve our knowledge of the neuroanatomy and physiology of erection and incontinence.
Introduction
From anatomic studies, Walsh identified the neurovascular bundle (NVB) in the posterolateral corner of the prostate. He developed the nerve-sparing radical prostatectomy and despite its wide adoption, erectile dysfunction complication rates remain high and variable. Because of anatomic studies demonstrating a wider anterior distribution of erectile nerves around the prostate, Menon and associates 3 developed the “Veil of Aphrodite” technique. This approach uses a high anterior release with preservation of the prostatic fascia to preserve more nerves and decrease apical traction; it has shown promising results. 3 Recent research, however, suggests that nerve locations are highly variable and nerve-mapping technology may help decrease complication rates. While Walsh's discovery has had a profound impact on the prostatectomy procedure, a lack of information regarding pelvic innervation has hindered further advances in the space. Currently, nerve-mapping technology is in the research phases, and none has yet received wide adoption. In this review, we will discuss the important neuroanatomic structures and the three main nerve-mapping technologies using stimulation, dyes, and direct visualization.
Neuroanatomy
Our understanding of erectile neurophysiology is limited. Erection is controlled by the unmyelinated parasympathetic nerves in the cavernous nerve (CN). These unmyelinated nerve fibers have a much slower conduction speed than myelinated fibers. The CN is estimated to be 2 to 6 mm in diameter and generally travels with and posterior to the NVB (Fig. 1). 1 Walsh's classic model is that the NVB arises from the inferior hypogastric plexus and runs posterolateral to the prostate (at 5 and 7 o'clock) until the membranous urethra, where it moves anteriorly until it is directly lateral to the urethra (3 and 9 o'clock). 1 NVB position relative to the clock face is not always consistent and can vary. Anatomic studies have found that only 52% of patients have a clear NVB, while the remainder have a wider fan-like nerve distribution around the prostate and within the multiple fascial layers. 4,5 Histologic studies have reported that 46% to 66% of nerves are located in the classic posterolateral position, while 21% to 29% are located more anteriorly, increasing with age (Fig. 2). 1,5 Electrostimulation of these nerves between 1 and 5 o'clock increases intracavernous pressure (ICP), although the strongest ICP response is at the 5 o'clock position where most of the nerves reside. 6
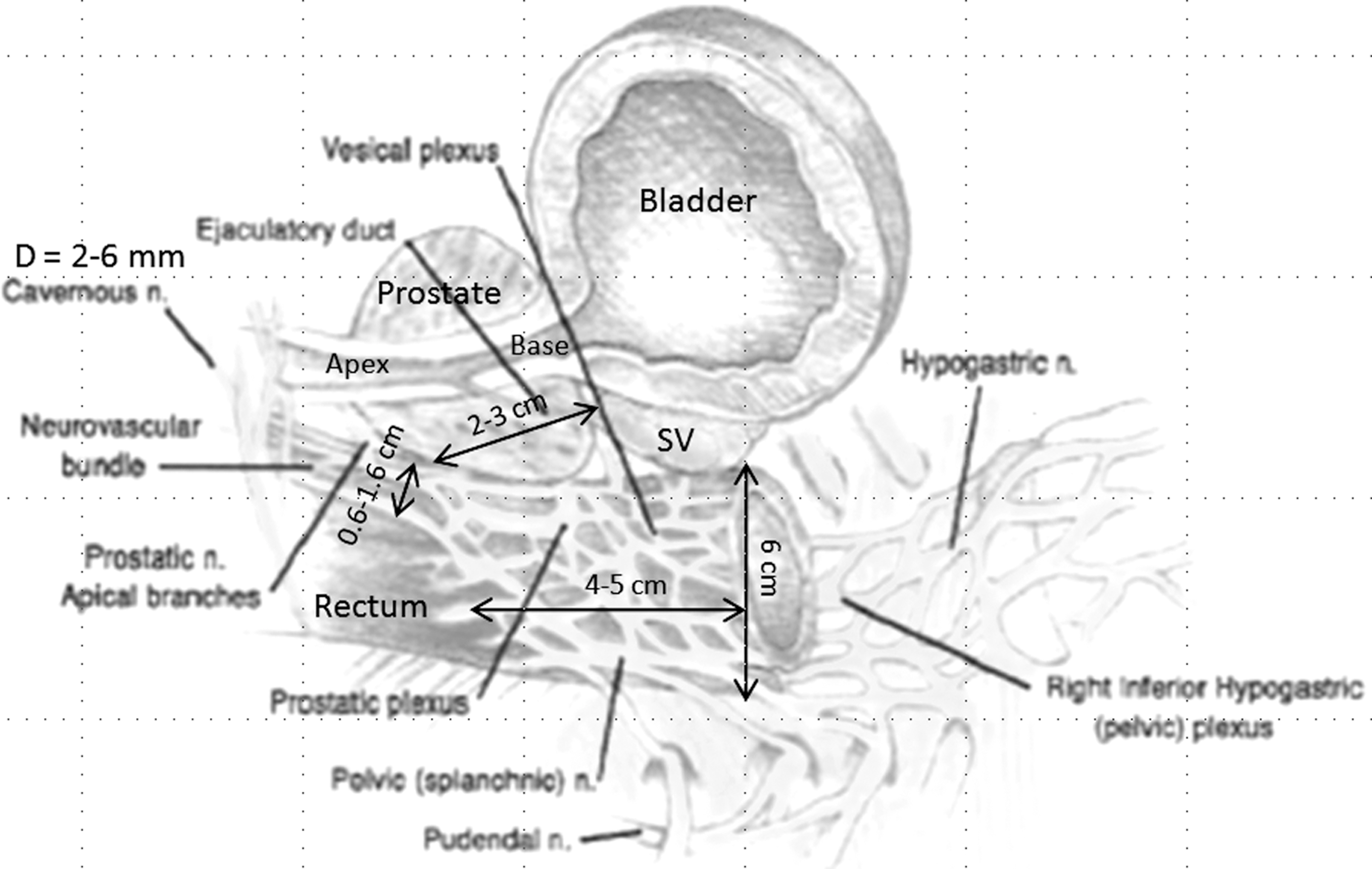
Sagittal cross-section of the prostate, bladder, and rectum with periprostatic nerves labeled and appropriate dimensions marked. SV=seminal vesicle. Adapted with permission from Tewari et al. Eur Urol 2003;43:444–454.

Lateral view of the prostate with mean nerve counts at different areas (mean nerve counts with diameter ≥200 μm/ ≤200 μm). Neurovascular bundle is marked in yellow, and nerves supplementing the posterolateral bundle are marked in blue. Reprinted with permission from Sievert et al. Eur Urol 2008 ;54:1109–1117.
To account for these different nerve distributions, Tewari proposed the Trizonal Neural Hammock model composed of a proximal neurovascular plate (PNP), predominant neurovascular bundle (PNB), and the accessory neural pathways (ANP). The PNP includes the inferior hypogastric plexus and extends to the proximal third of the prostate in 75% of patients. The PNB is equivalent to the previously discussed NVB, while the ANP corresponds to the anterior nerves that have recently gained more significance. 1 Histologic studies found that ganglia are common in the PNP, NVB, pedicles, dorsal aspect of the seminal vesicles (SVs), and circumferentially around the apex.
During a radical prostatectomy, the nerves are at most risk during dissection of the SVs, pedicles, and apex. At the SVs, both the PNP and NVB are 0 to 2 cm posterolateral to the inferior tips of the SVs. 7,8 Depending on the surgeon's preference on anterior or posterior SV approaches, the exposure can vary significantly. At the pedicles, the NVB and distal PNP range from 0 to 1 cm away from the vessels, and in addition, some nerves intermingle with the pedicles. The pedicle structure varies with prostate size and shape, potentially complicating the dissection and increasing the risk of nerve damage. 7,8 The third critical dissection is the apex, where the NVB runs just 3 mm from the prostate capsule and more distally at the membranous urethra only 3 to 4 mm from the urethral lumen. The course of the nerve is most variable here, increasing the difficulty of the dissection. 2,7,8
Nerve Stimulation Techniques
Nerve stimulation was one of the first nerve-mapping approaches used clinically. These technologies apply a probe to stimulate a nerve and then detect a specific physiologic response, such as an action potential or tumescence. The major advantage of this approach is that only nerves responsible for erectile function (or other desired physiologic response) are detected. The disadvantage is that each point needs to be tested individually, potentially slowing the surgical work flow. Because erectile nerves are unmyelinated, their conduction is slow and has long time constants to both observe a response (0 to 2 minutes) and to wait for a subsequent test (45 to 120 seconds) (Tables 1 and 2).
FDA=Food and Drug Administration.
FDA=Food and Drug Administration; H=human; I=in vivo; ICP=intracavernous pressure; A=animal.
These technologies can be assessed by focusing on the means of stimulation (electrical or optical) and measurement outputs (tumescence/detumescence, action potentials, ICP, intraurethral pressure (IUP), or impedance). Each of these stimulation and measurement outputs have their advantages and disadvantages that are discussed with each device below. New technologies may be developed by mixing and matching these stimulation and measurement tools to attempt to overcome the limitations of currently studied devices.
CaverMap
CaverMap (Blue Torch Medical, Rockville, MD) was the first commercial and Food and Drug Administration (FDA) approved nerve mapping technology used clinically for prostatectomies (Fig. 3). It is composed of a probe with 8 electrodes spread over 1.2 cm, and 1, 2, 4, or all 8 electrodes can be activated for different spatial resolution. A single electrode would have a spatial resolution of approximately 1.5 mm. The physiologic response detected is tumescence or detumescence and is measured with a ring placed around the penis. Early studies used a 0.5% change in penile circumference as a positive response, but later studies suggested better specificity is achieved with a threshold of 1.0%. Intraoperatively, a point is stimulated with the probe, and a response would occur in 0 to 120 seconds (median 15 to 20 sec). If the tumescence/detumescence response reaches the threshold, there is a nerve at that point. There is no nerve if threshold is not reached. Before a subsequent site can be tested, another 45 to 60 seconds must elapse to decrease the risk of interference from the previous stimulation. Clinical studies report that the testing increases procedure time by 17 minutes on average.
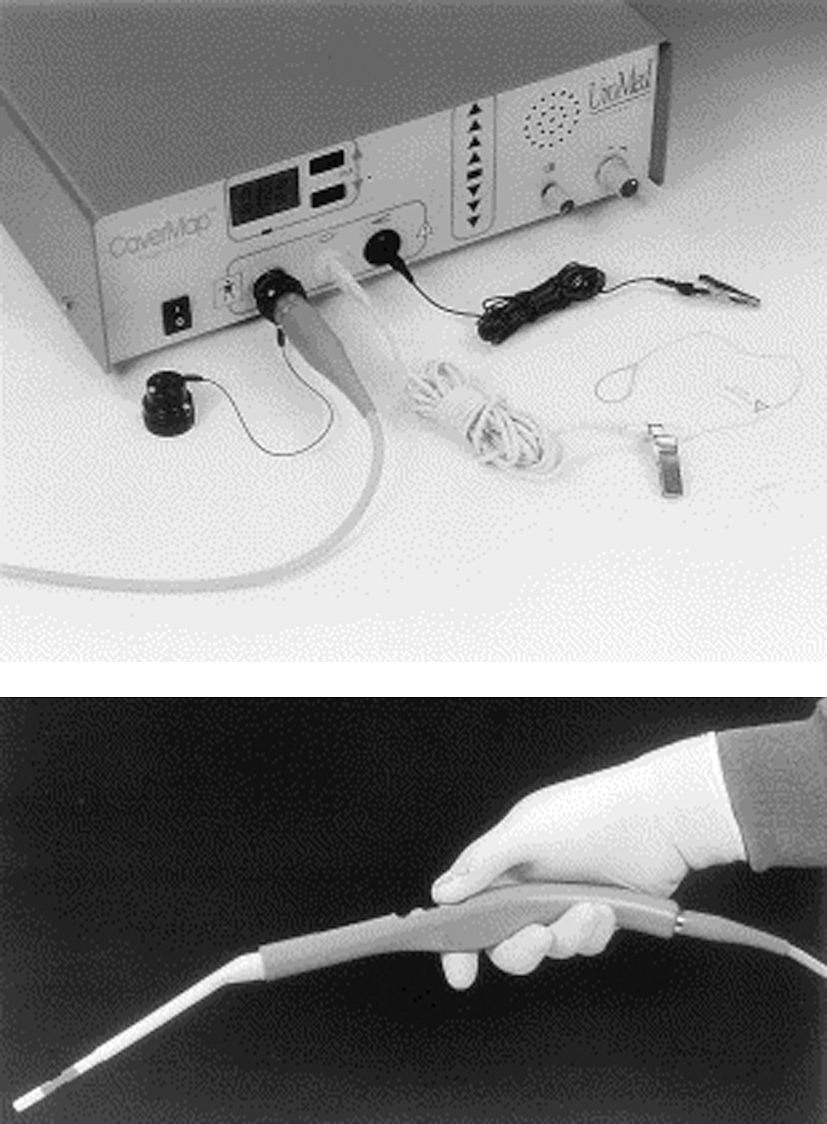
Top is the CaverMap control unit with tumescence sensor, and below is the nerve stimulating probe. Reprinted with permission from Klotz and Herschorn. Urology 1998;52:537–542.
Much of the clinical research using CaverMap was conducted in the late 1990s and early 2000s, with early results promising improved outcomes. Later studies, however, showed inconsistent results. For a more detailed analysis of the clinical results, see the review by Klotz. 9 The current consensus is that the system can be useful to test NVB integrity after removal of the prostate but is not specific for predicting long-term potency. The key limitation of this technology is the unreliability of tumescence/detumescence as measured by penile circumference. The long time constant to detect a response severely slows surgical work flow and decreases the frequency at which multiple spots can be tested. Of the technologies discussed during this review, CaverMap has had the most clinical trials and, because of its unreliability, the system has had a very limited adoption in the urology community.
ProPep
ProPep (ProPep Surgical, Austin, TX) is a more recent electrical stimulation technology that delivers stimulation through robotic Maryland bipolar forceps (Intuitive Surgical, Sunnyvale, CA). Two needle electrodes are inserted via a patent-pending delivery system and positioned in both levator ani muscles. With nerve stimulation, levator ani action potentials can be detected quickly and frequently without interference from previous stimulations. Visual confirmation of levator ani contractions corroborates the electrode readings. This approach can be useful for identifying the somatic perineal branch of the pudendal nerve. Initial clinical studies reported that ProPep can predict recovery of continence, but its ability to improve outcomes is unknown. 10 Because the somatic nerves provide fast and reliable muscle action potentials in the levator ani, there are no concerns for waiting between stimulations or having frequent testings. In theory, this approach may be able to help surgeons improve continence complication rates.
Unpublished studies suggest the needle electrode can be placed distally in the NVB adjacent to the membranous urethra to detect stimulation through the CN, although whether the benefit of NVB detection would outweigh potential physical damage resulting from electrode insertion is unresolved. The autonomic action potentials are slower and lack the characteristic action potential waveform seen in muscle. These slow action potentials with incompletely characterized waveforms face the same limitations that hindered CaverMap with the time to detect a response and inability to frequently test multiple spots. Measuring tumescence/detumescence and nerve action potentials may not be the most reliable or easiest to integrate into a clinical setting. Nonetheless, more clinical trials are needed to determine ProPep's ability to preserve continence and potency. The company has recently submitted an application for FDA approval.
Fixed bipolar electrode
Kurokawa and colleagues 11,12 at Gunma University School of Medicine developed a bipolar stimulating electrode with a fixed 7-mm separation distance and used it to measure increases in ICP with a needle placed in the corpus cavernosum. The testing protocol involved stimulation at a point and tracking of ICP response for 10 to 60 seconds. If ICP increased above threshold, that counted as a positive response. For a point to be classified as negative, three subthreshold ICP responses are needed. Between each test, there is a wait time of 1 to 2 minutes for ICP to stabilize. A unilateral response (at a threshold ICP of 4 cm H20) with assessment of erectile function by interview was found to have a sensitivity of 69.2% and specificity of 100%. The authors suggest that their device could be used to predict postoperative potency, but did not report if it could be used to improve surgical outcomes. 12 The use of ICP as a measurement tool has faster response times than with tumescence/detumescence and is reported to have a higher specificity. Consequently, using ICP with the previously discussed nerve stimulation technologies may lead to more reliable results and possibly improved surgical outcomes. Although having a faster response, the response time is still slow enough to hinder surgical work flow.
Follow-up research with this bipolar stimulating electrode reported on the use of IUP measurements (measured with an intraurethral balloon) in conjunction with ICP. 13 The authors found that IUP had a quick increase with stimulation and quick decrease with the end of stimulation, whereas ICP had a longer time course, as was discussed previously. In the patients studied, the CN position as determined by ICP measurements was variable and did not always correlate with the NVB. On the other hand, the urinary continence nerves tended to consistently run within the NVB. 13 IUP is controlled by somatic nerves as discussed previously, and as a result has a much more reliable measurement output than ICP, which is controlled by autonomic nerves. This study also brings the use of ICP for detecting potency nerves into more question. The combined measurement of both continence and potency could be integrated into future devices and lead to a combined nerve stimulation device that could lead to improved complications rates for both.
Needle array probe
Researchers at the University of British Columbia developed a needle array probe that uses sequential electrical stimulation (with a 5 mA sinusoidal current) through each electrode with concurrent impedance measurements to determine nerve locations. This system is capable of real-time intraoperative electrical impedance tomography and to date has been validated in vitro and in vivo using rat sciatic nerves. 14 Although successful in finding the somatic sciatic nerve, which is a well-defined bundle, it remains to be seen whether it can work in the periprostatic area where numerous nerves of varying dimensions run both in bundles and independently. In addition, this technology is not correlated with a physiologic outcome as are the other nerve stimulation technologies. It remains to be seen whether it can be translated to an intraoperative setting.
Optical nerve stimulation
Fried and colleagues 15 developed an optical means of activating nerves using infrared lasers with a 1-mm diameter beam. The beam is at a wavelength of 1870 nm, providing a penetration depth of 400 μm. This technology offers high resolution targeting of nerves and a noncontact means to activate them. They studied the use of lasers in a rat model and measured ICP as their physiologic output. When laser stimulation was compared with electrode stimulation, it generally had a 10-second delay in ICP response in addition to an overall lower peak ICP. 15
Lasers are theorized to activate nerves by heating them to a stimulation threshold of 42°C to 45°C, and this heating time was found to be 10 seconds and corresponded with the onset of ICP response. Stronger lasers can heat nerves faster, but would place them at greater risk of damage because the injury threshold is 47°C. 16 Other researchers found that a subthreshold electrical stimulus combined with optical stimulation can provide a wider thermal safety window. The ratio of laser exposures for damage to stimulation with pure infrared stimulation is 2:1, while with subthreshold electrical stimulus the ratio increases to 6:1. 17
Tozburun and coworkers 18 created a laparoscopic laser probe that can stimulate a target 20 mm away with a 1-mm beam, and it was successfully used for in-vivo rat experiments. This technology uses ICP as the physiologic output measured as did the fixed bipolar and has the advantages and disadvantages of that measurement system. The laser has the added risk of having a narrow safety window that does not affect direct electrical stimulation. Because the theorized mechanism of activation is by heating, the efficacy of nerve activation would be more variable based on the amount of tissue, blood, or fluid surrounding the nerve of interest. Using a laser may provide a noncontact means of stimulation; it pays for it with a slower response time than electrical stimulation and with a high risk for damage. Thus, direct electrical stimulation may be a more reliable, faster, and safer means to stimulate nerves.
Dye-Based Visualization Techniques
Nerves can also be visually identified with dye labeling. This technique allows nerves to be found without repeated testing as is needed with stimulation. The labeled nerves, however, may not be responsible for erectile function, because labeling is not tied to physiologic response. Commercialization challenges include years of toxicity and efficacy testing necessary for FDA approval. Currently, the only FDA-approved dyes that have been studied in prostatectomies are indocyanine green (ICG) and fluorescein.
Some of the important characteristics in evaluating a dye are its method of delivery, nerve specificity, time for staining, and resolution. Dyes are generally delivered by either local delivery into the base of the penis with retrograde transport along the erectile and other nerves innervating the penis or systemic delivery with labeling of all nerves. They have different nerve specificities, depending on their target. Some dyes target myelin, in which case they would not be expected to label the unmyelinated CN. The optimal staining time plays a role in determining the preoperative preparation, because staining can occur anywhere from minutes to months after administration, depending on the method of delivery. Lastly, the dye's resolution is critical for insuring nerves of appropriate size can be identified (Tables 1 and 3).
FDA=Food and Drug Administration; IV=intravenous; A=animal; I=in vivo; H=human; E=explant.
Avelas
Avelas is a start-up company spun from Dr. Roger Tsien's University of California, San Diego, laboratory that is commercializing fluorescent peptides. They use phage display to select peptides targeting either purified myelin basic protein or peripheral nerve. This dye is delivered intravenously (IV) and can clearly label peripheral nerves in 2 hours for mice. In an in vivo mouse model looking at myelinated somatic nerves, Whitney and associates 19 reported that they had a resolution of 50 μm and could view nerves at a depth greater than could be seen under white light, but the depth was not quantified (Fig. 4). The researchers found no obvious toxicity as noted by no apparent behavior or activity changes after treatment. Greater study is warranted to progress with human trials.

Mouse sciatic nerve under white light (above) and fluorescence (below) 2 hours after intravenous injection of Avelas' dye candidate. This dye offers nerve visualization at depths greater than possible with white light. Reprinted with permission from Nat Biotechnol. 19
Recurrent laryngeal nerve explants from patients were treated with the peptide and found to have similar staining as the mouse with the greatest concentration in the nerve's connective tissue, such as the epineurium, perineurium, and endoneurium. 19 If used during prostatectomies, one concern is whether the peptides would target the unmyelinated CN. Assuming it labels the CN and receives FDA approval, this technology is promising because of its high resolution and fast staining time.
General Electric
General Electric has filed multiple patents on fluorescent compounds designed to target myelin basic protein. They report testing the dyes in mice models by intraperitoneally or IV delivery, and they were able to label somatic nerves in vivo 4 hours after delivery. 20 –23 It remains to be seen whether this dye will target the unmyelinated CN, and whether it will be safe to use in humans.
Cholera toxin subunit B-AlexaFluor 488
Researchers at the University of Virginia created a dye by conjugating AlexaFluor 488 with cholera toxin subunit B. This dye is retrogradely transported up the axon after local injection into the corpus cavernosum. From in-vivo rat studies, the dye took 9 days for optimal CN staining. It is theorized that human staining would take 38 to 45 days, because the dye is transported at a fixed speed and the nerves are four to five times longer in humans. The dye was visualized using the CellVizio (Mauna Kea Technologies, Newton, PA) fluorescent confocal microscope with a resolution of 40 μm, depth of 15 μm, a viewing window of 0.6 mm by 0.5 mm, and a frame rate of 12 frames per second. Potential toxicity was assessed by histologic staining for apoptosis and comparison of maximal ICP pressure responses with and without staining. No differences were found between the stained and unstained groups, suggesting no toxicity as noted by these measures. 24 Further testing of toxicity will be needed for FDA approval, and additional research will be needed to identify optimal human dosing because of the predicted month long staining. Unless the time for optimal staining can be improved, this technology may be difficult to integrate into clinical use.
OptiScan
OptiScan Pty. Ltd. (Victoria, Australia) has a confocal microscope that has been investigated for use in prostatectomies in an early stage clinical trial (NCT00792961). A few hours before surgery, nonspecific fluorescein dye is delivered systemically for contrast. The system is reported to have a resolution of 500 μm and can view a depth of 2 μm. Unpublished results found that the utility of the system was severely limited by its bulkiness and necessity to be placed perpendicular to the tissue of interest. The narrow confines of the pelvis and irregular surfaces severely limited the tissues that could be examined. Newer versions have a more streamlined design. An additional issue is the limited penetration depth of 2 μm that can be easily obstructed by small quantities of blood.
When using a fluorescein dye, an experienced operator would be needed to identify tissues based on imaging. Unpublished studies have found that this could be circumvented by using nerve-specific stains such as cresyl violet. The narrow viewing window of the probe, however, puts this system at a disadvantage relative to the other dye-based visualization techniques. Based on the clinical trial to date, this technology does not have much promise for clinical use in its current form because of the limited viewing window and penetration depth.
Novadaq
Novadaq Technologies Inc. (Bonita Springs, FL) is a company that sells intraoperative fluorescent imaging systems and has two dyes that can be used for nerve mapping: FDA approved ICG and non-FDA approved ICG conjugated with inactivated herpes simplex virus 2 (HSV2). Golijanin and colleagues 25 had reported in early studies that local injection of ICG into rat crura led to retrograde transport with optimal intraoperative staining at 18 to 24 hours. They correlated the results with histology and reported that fluorescence was localized to nerves. Later experiments could not replicate these results.
ICG is a nonspecific dye, and it is thought that the lymphatic system was marked. It is very unlikely that plain ICG will be used clinically for identification of nerves. Thus, Novadaq applied for a patent for ICG conjugated with HSV2 and reported that somatic nerves in mouse models could be labeled in 2 hours while rabbits were labeled in 4.5 hours. 26 It is unknown whether this dye would label the autonomic CN, and significant toxicity and safety testing will be necessary before FDA approval. The stigma of conjugating ICG to HSV2 may severely hinder the ability to perform the necessary toxicity and safety testing to receive FDA approval and from there move on to clinical utility studies.
Fluoro-Gold
Davila and coworkers 27 examined the use of various dyes (Fluoro-Gold, Fast-Blue, Fluoro-Ruby, and green fluorescent pseudorabies virus) delivered via intracavernosal injections for identifying the CN nerve. They explanted the NVB and examined the samples under fluorescent microscopy and found that Fluoro-Gold produced the best staining at the 2- and 3-day explant time points. Fluoro-Gold is a retrograde dye that is sold by Fluorochrome, LLC for research purposes. 27 Further studies in intraoperative imaging and for toxicity/safety will be needed before human use. This dye is not being developed for intraoperative use and is only being used for pathology staining, and it will likely not make it to clinical use.
Direct Visualization Techniques
Direct visualization includes methods that do not use dyes. These technologies have a significantly simpler FDA approval process compared with the dye-based techniques. They also face the problem of labeling nerves without physiologic correlation and having limited viewing windows (Tables 1 and 4).
FDA=Food and Drug Administration; H=human; I=in vivo; E=explant.
Optical coherence tomography
Optical coherence tomography (OCT) uses near-infrared radiation in a manner similar to B-mode ultrasound (US) to produce images with a resolution from 1 to 15 μm, depth of 1.6 mm, and a viewing window of 200 by 200 pixels. The OCT probe can be used in both contact and noncontact means. Imalux Corporation sells the FDA-approved Niris OCT system that includes a laparoscopic probe.
Studies in rats have found that the OCT images correlate with histology findings (Fig. 5), and that the CN could be accurately identified by OCT as confirmed by electrical stimulation and ICP measurements. 28,29 When looking at human explants, the image landmarks were not as clear, because humans have a thicker capsule, denser stroma, and more periprostatic fat through which blood vessels and the CN run. 28 Intraoperative (laparoscopic and robotic) human studies with the OCT probe could find the NVB, and images correlated with the surgeon's impression and histology. 30
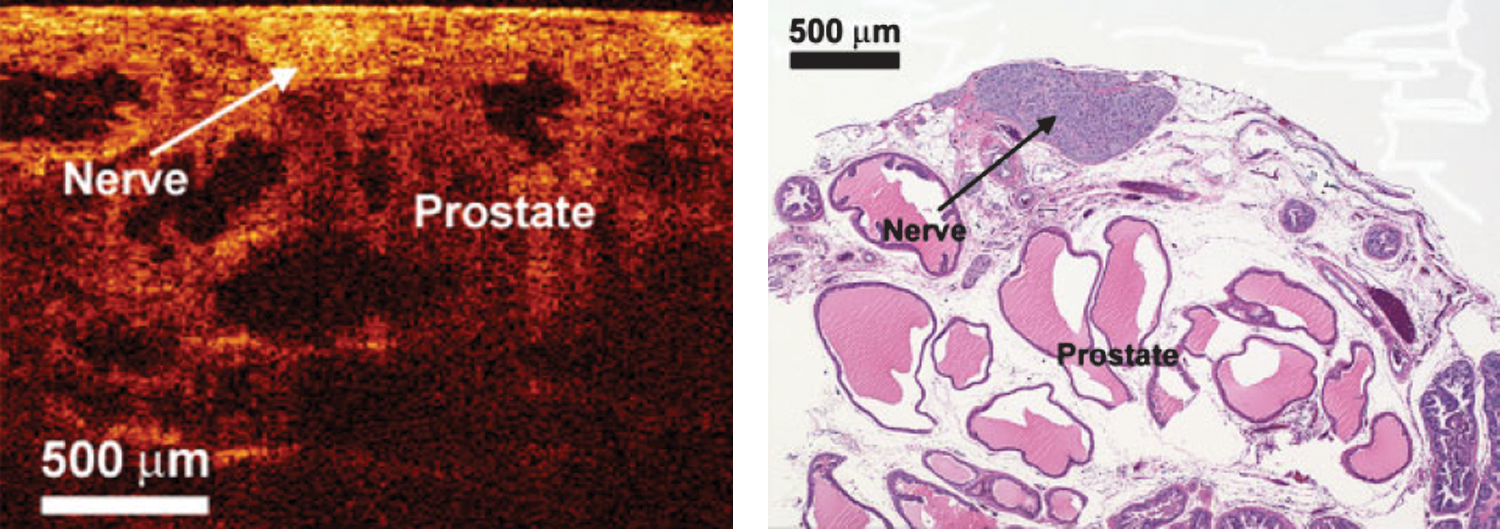
Optical coherence tomography (left) and histologic (right) cross-sectional images of the rat cavernous nerve. Re-printed with permission from Lasers Surg Med. 29
Widespread adoption of this technology is limited by the need for surgeon training to interpret OCT images. This technology has been used in some preliminary studies and has the necessary FDA approval, but the key efficacy studies have not been published. If a study can demonstrate decreased complications with OCT, then wide adoption would be easier than other technologies.
Multiphoton microscopy
Multiphoton microscopy is a novel technology that uses near-infrared radiation to elicit autofluorescence in a cell's reduced nicotinamide adenine dinucleotide and flavin adenine dinucleotide. This technique can provide real-time noncontact images and provide different resolutions based on the objective lens. With a 4x objective, the resolution is 6 μm/pixel, depth of 400 μm, and viewing window of 3 mm2, whereas, the 20x objective has a resolution of 1.2 μm/pixel, depth of 250 μm, and viewing window of 614 μm2. Studies to date have demonstrated that the images correlate with histology in both rat and human explants. 31,32 It remains to be seen how to convert the system for intraoperative use and if it will be effective. Assuming the nerves can be easily identified on the image, integration of this system into a robotic console shows promise.
US
Transrectal US with and without Doppler has been explored for potential intraoperative use during radical prostatectomies. To date it has shown promise in improving oncology margins. 33 Its use to identify the CN, however, is severely limited by inadequate system resolution. Generally, the CN is expected to be lateral to the blood vessels, which are found by Doppler. US elastography is a newer approach that can differentiate tissues based on their density and stiffness during tissue deformation. Fleming and colleagues 34 were able to identify the nerves around the prostate in a rat model using elastography and found that they were noncompressible relative to the surrounding tissue. The resolution of currently available US is not sufficient to detect the very small CN and its branches. Without major strides in US capabilities, it does not show much promise for use in nerve mapping.
Coherent anti-Stokes Raman scattering
Coherent anti-Stokes Raman scattering (CARS) uses nonlinear excitation of chemical bonds and detects the vibrational transitions of these bonds to differentiate tissues. Gao and associates 35 built a custom CARS system with a resolution of 0.4 μm and frame rate of 3.93 fps. They examined human explants cut into pieces measuring 5 mm on each axis. The viewing window of the system was 200 μm by 200 μm, and images were acquired every 1 μm through a z-stack of 30 μm. Each sample needed less than 5 minutes for imaging and analysis. They reported that they could distinguish normal from cancerous glands and were able to identify the CN. Signals from lipid rich myelin sheaths were thought to play the largest component. 35 It remains to be seen whether CARS can identify the unmyelinated CN. Additional work to miniaturize and test the system is needed to verify that it can work in an intraoperative setting. Adapting this system for intraoperative use and the ability to detect unmyelinated nerves will be the key obstacles that this device faces for clinical adoption.
Conclusion
Many researchers are developing several novel technologies that can be categorized as stimulation based, dye-based, or direct visualization. They all have their own advantages and disadvantages and as of yet, none has shown clear evidence to improve surgical outcomes. Because of lack of clinical efficacy for all and limited FDA approval for some, none has been adopted into regular clinical use. Further development of these technologies is necessary to overcome their limitations so that they have the chance to improve complication rates after prostatectomies. Clinically, some technologies have demonstrated utility in predicting the development of complications. By using that information, more aggressive rehabilitation programs may lead to improved long-term function. These technologies could also be applied for research to improve our knowledge of the neuroanatomy and physiology of erection and incontinence and lead to better nerve-mapping devices that can improve surgical outcomes.
Footnotes
Disclosure Statement
Drs. Sorger and Mohr are employees of Intuitive Surgical, Inc. For Dr. Ponnusamy, no competing financial interests exist.