
Abstract
Purpose:
The aim of our study was to compare early complication rates between the robot-assisted radical cystectomy (RARC) and open radical cystectomy (ORC) using a standardized reporting system.
Patients and Methods:
From September 2008 to March 2011, 35 and 104 patients underwent ORC and RARC, respectively. Demographics and perioperative and complication data on all patients were reviewed retrospectively and compared between the two groups. All complications were categorized using a modified Clavien reporting system. We also sought to identify independent predictive factors of grade II or greater complications.
Results:
There were no significant differences between the ORC and RARC groups with regard to age, body mass index, American Society of Anesthesiologists score, clinical stage, surgical procedure history, or sex. The RARC group had more cases of ileal neobladder urinary diversion (P<0.001). We did not find any differences in terms of pathologic stage or length of stay. The ORC group had more grade II or greater complications (P=0.001), wound problems (P=0.043), multiple complications (P=0.014), greater estimated blood loss (EBL) (P<0.001), and needed more transfusions (P<0.001). A longer operative time was needed in the RARC group, however. Multivariate logistic regression analysis demonstrated that the ORC (P=0.045, odds ratio [95% confidence interval]=2.44 [1.02–5.85]), EBL (>500 mL, P=0.013, 2.75 [1.24–6.10]), and female sex (P=0.028, 4.06 [1.12–14.11]) were independent predictors of grade II or greater complications.
Conclusions:
Our results showed that the RARC group was comparable to the ORC group with respect to complications using the Clavien reporting system. Further long-term and randomized trials are needed, however, because RARC is still not considered the standard therapy for bladder cancer.
Introduction
Recently, interest in laparoscopy and robot-assisted surgeries has increased with the goal of reducing procedure-related morbidity in the field of urology. Over the last few years, studies of robot-assisted radical cystectomy (RARC) have focused mainly on feasibility and early oncologic and functional results. 7 –9 The early data from these articles demonstrate that RARC is similar to laparoscopy. The leading groups supporting the use of RARC believe that RARC leads to a faster recovery, shorter hospital stay, and more rapid return to daily activities compared with open radical cystectomy (ORC), while offering the same functional and oncologic outcomes. 10 RARC, however, is still regarded as an investigative treatment because there are insufficient data that compare ORC and RARC in terms of oncologic, functional, and perioperative complication outcomes.
A standardized reporting system is mandatory to allow for meaningful interpretation of surgical complications. As such, there are a growing number of studies that have used a standardized reporting system for surgical complications since the modified Clavien system was validated in a large cohort of general surgery patients. 11 The modified Clavien system has also been used to report complications in urologic surgery and to provide a good quality system by which urologic physicians can classify complications. Several studies have analyzed complications associated with ORC and RARC according to the Clavien system, and the current trend supports the increased use of this system. 3,8,12
The goal of the current study was to retrospectively compare early complications between ORC and RARC using the modified Clavien system. Risk factors for perioperative complications in the overall patient sample were identified by logistic regression analysis.
Patients and Methods
This study was approved by the Institutional Review Board at Samsung Medical Center/Sungkyunkwan University School of Medicine.
Patients
Between September 2008 and March 2011, ORC and RARC were performed in 35 and 104 patients, respectively, to manage bladder cancer. We excluded the patients who had undergone radiotherapy before operation or for whom palliative treatment was the primary aim. Clinical and pathologic parameters were collected retrospectively, including age, sex, BMI, American Society of Anesthesiologists (ASA) score, history of pelvic surgery, history of intravesical bacillus Calmette-Guerin (BCG) or chemotherapy, clinical and pathologic stage, operative time (from skin incision to closing), estimated blood loss (EBL), the number of lymph nodes (LNs) removed, length of stay (LOS), and diversion type. Type of preoperative bowel preparation was not different in both groups. Polyethylene glycol-electrolyte solution was routinely given 2 days before surgery, and then patients kept fast.
Operative technique
The ORC were performed by five surgeons, and two surgeons of those performed RARC. Although all operations have not been performed by the same surgeon, the techniques we used were not different regarding bowel anastomotic technique, ureterointestinal anastomosis. Our surgical technique for RARC and PLND using the da Vinci system has followed what other authors described previously. 13 A six-port transperitoneal approach was used with patients in the extended lithotomy position with a 25- to 30-degree Trendelenburg tilt. After excision of the bladder, the robot undocked, and urinary diversion was performed extracorporeally through a 5 to 7 cm subumbilical midline incision. For the ileal neobladder, the robot was redocked for the urethrovesical anastomosis, and the Studer method was used. In the case of ileal conduit, the distal end of the conduit was fashioned as a stoma at a preoperatively marked site on the abdominal wall.
All patients of both groups have undergone standard PLND. The extent of standard PLND was bifurcation of the common iliac artery proximally, the genitofemoral nerve laterally, the circumflex iliac vein and lymph node of Cloquet distally, and the hypogastric vessels posteriorly, including the obturator fossa. Running suture and reinforcement with interrupted suture on some several places for fascial closure were used in the open group and minilaparotomy site of the robotic group. One or two interrupted sutures were applied for the port site of the robotic group.
Postoperative management
In our center, a nasogastric tube is routinely inserted after completion of anesthesia in the operating room and maintained until confirmation of passing of flatus. Oral fluids were started 5 days after the operation, after which semisolids and solids were provided consecutively as tolerated. Ureteral stents were removed on day 14.
Postoperative complications
We performed a meticulous review of all medical records including admission, catamnesis, test results, and even nursing charts and outpatient clinic records after discharge. We also determined whether patients were readmitted for later-onset complications (90 days after operation). All complications were classified from grade I to V according to the modified Clavien complication classification system.
Statistical analysis
The distribution of continuous variables between the two groups was compared using the Student t tests for independent samples. The distribution of categorical variables in both groups was compared using the Pearson chi-square tests and the Fisher exact tests when the proportion of patients in one or more categories was less than 5%. Logistic regression analysis was used to predict perioperative risk factors for complications categorized as grade II or greater by the Clavien complication classification system. Variables with P<0.20 on univariate analysis were included in multivariate analysis. Total operative time with respect to the number of surgeries performed (ie, learning curve) was measured using the Pearson correlation analysis. Statistical significance was assessed based on a two-sided significance level of P<0.05. Statistical analysis was performed using IBM SPSS Statistics version 19.0 (an IBM company).
Results
Patient characteristics
Patient demographic characteristics are shown in Table 1. The RARC group (mean±standard deviation [SD]: 62.2±10.5 years) was younger than the ORC group (65.9±9.4 years), but the difference of value was marginal (P=0.050). No significant differences were identified in terms of the sex ratio, BMI, ASA classification, history of pelvic surgery, history of intravesical BCG and chemotherapy, or clinical stage between the two groups.
Student t test.
Chi-square test.
Fisher exact test.
RARC=robot-assisted radical cystectomy; ORC=open radical cystectomy; BMI=body mass index; ASA American Society of Anesthesiologists; chemoTx=chemotherapy; Hx=history; CIS=cacinoma in situ; BCG=bacillus Calmette-Guerin.
Perioperative data
Twenty-two (62.9%) patients in the RARC group underwent ileal neobladder formation, compared with only 19 (18.3%, P<0.001, Table 2) patients in the ORC group. The overall mean operative time was 77 minutes longer in the RARC group than in the ORC group (P<0.001). In the subgroup analysis of operative time, there was no difference in the ileal conduit between the two groups, but more operative time was still needed in the RARC group for the formation of the ileal neobladder. The RARC group had a lower mean EBL (P<0.001) and needed fewer transfusions (P<0.001) than the ORC group. The mean number of LNs removed was greater in the RARC group than in the ORC group (P<0.001). The LOS and the pathologic stage distribution were similar in both groups.
Student t test.
Chi-square test.
All of four persons had a single kidney at the time of operation.
RARC=robot-assisted radical cystectomy; ORC=open radical cystectomy; EBL=LN=lymph node; CIS=carcinoma in situ; OP=operative time.
Complications
The overall complication rate did not differ between the two groups (P=0.206). The total number of complications in the ORC and RARC groups was 27 and 124, respectively (Table 3). The details of each complication are shown in Table 4. There were more patients who experienced grade II or greater complications in the ORC group than in the RARC group (P=0.002). With regard to multiple complications, there were fewer in the RARC group (P=0.014). The distribution of the highest grade complication tended to be lower in the RARC group (P=0.014). More wound problems such as dehiscence and infection occurred in the ORC group (P=0.043). There was a higher rate of urinary tract infection (UTI) in the RARC group, but the difference was not statistically significant (P=0.058). The mortality of the two groups was similar, and detailed causes of death are described in Table 5. The readmission rate was not different between the two groups. There were one and three cases of urine leakage at the anastomosis site in the ORC and RARC groups, respectively (P=0.049); in these cases, the leakage occurred in the urethroneovesical anastomosis site in the RARC group and the ureteroileal anastomosis site in the ORC group.
Chi-square test.
Fisher exact test.
RARC=robot-assisted radical cystectomy; ORC=open radical cystectomy.
Fisher exact test.
Chi-square test.
RARC=robot-assisted radical cystectomy; ORC=open radical cystectomy; UTI=urinary tract infection; CVA=cardiovascular accident.
The patient presented with severe hematochezia and hypovolemic shock.
RARC=robot-assisted radical cystectomy; POD=postoperative day; ORC=open radical cystectomy; UTI=urinary tract infection.
Predictors of grade II or greater complications
The type of operation (ORC group), sex (female), and EBL (>500 mL) were significant parameters on univariate analysis for factors associated with grade II or greater complications. These factors were still independent predictive factors on multivariate analysis (Table 6).
Variables at P<0.20 on univariate analysis were selected for multivariate analysis.
OR=odds ratio; CI=confidence interval; RARC=robot-assisted radical cystectomy; ORC=open radical cystectomy; BMI=body mass index; ASA=American Society of Anesthesiologists; OP=operative; Hx=history; BCG=bacillus Calmette-Guerin; EBL=estimated blood loss; LN=lymph node.
Learning curve for RARC
The total operative time decreased dramatically with increasing number of surgeries performed (Pearson correlation coefficient r=−0.599, P<0.001, Fig. 1). The operative times for the last five cases were not different between the two groups (ORC: 415.0±89.6 min vs RARC: 439±63.7 min; P=0.639).
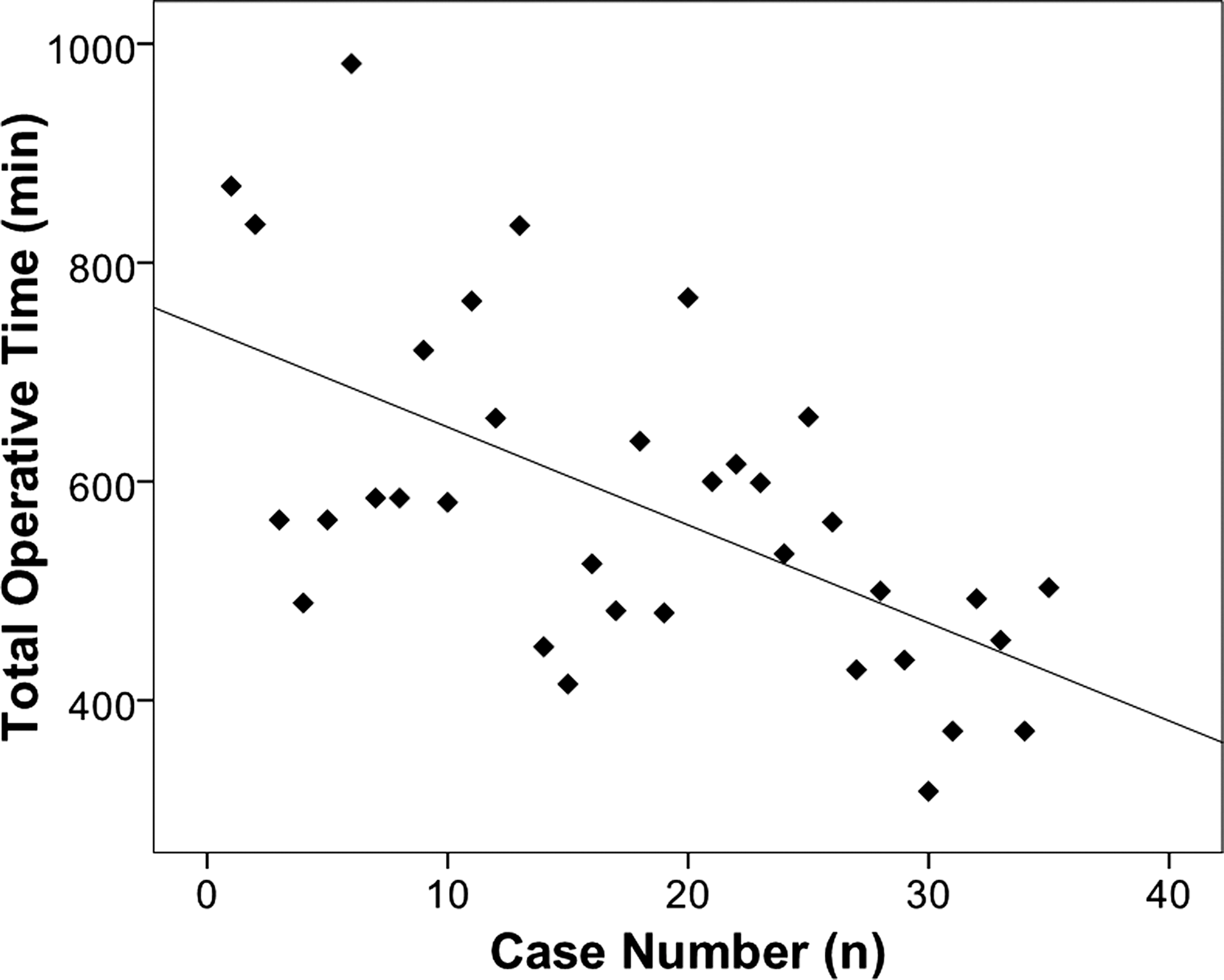
Operative time vs case number; Pearson correlation coefficient: r=−0.599, P<0.001.
Discussion
Shabsigh and associates 3 showed that the complication rate was 64% using the modified Clavien system, and Kauffman and colleagues 8 reported a rate of minor complications as high as 79%, both of which are relatively high in comparison with results from other studies. They attributed the high rate of complications to differences in the methodologies used to collect and report data as well as differences in surgeon experience, technique, and type of institution. In our institution, the complication rates of RARC and ORC were 62.8% and 74.0%, respectively, and these are not much different from rates reported by other studies using the standardized reporting form.
Our findings showed that undergoing ORC was an independent predictor of more complications on multivariate analysis, even though perioperative data were somewhat different between groups. Additional predictors included sex (female) and EBL (greater than 500 mL). We assessed grade II or greater complications because we felt that a comparison of these types of complications between ORC and RARC would be more meaningful in the clinical setting. Grade I complications in the modified Clavien classification are defined as any deviation from the normal clinical course, such as simple use of antiemetics and antipyretics. In other words, because of the structure of the standardized Clavien system report form, we would have had to include trivial problems in our analysis if we chose to assess grade I complications, and this would likely have affected our results. In addition, the fact that patients experiencing no complications or only grade I complications needed a shorter hospital stay supports our method of data analysis (data not shown). There were also fewer severe complications (grade III or greater) in the robotic group, but the difference was not significant. These results may be because of the limited sample size.
A number of previous studies have shown that EBL and the subsequent transfusion requirements are associated with complications. 14,15 Casey and coworkers 12 suggested that the cause of the lower complication rate in robot-assisted cystectomy may be related to the lower EBL. In their study, the robotic cohort had less blood loss (460 vs 1172 mL), and RARC was highly correlated with lower EBL (Spearman rank test ρ=0.65). They explained that the higher EBL may itself be deleterious in a patient who has several comorbidities and could result in a greater degree of surgical difficulty and more extensive disease. In the present study, multivariate analysis revealed that EBL greater than 500 mL was an independent predictor of complications, and was correlated with the need for transfusion and grade II or greater complications (ρ=0.579 and 0.424, respectively, both P<0.001; data not shown in the Results section). Because transfusion itself was considered a grade II complication in the Clavien system, if more EBL occurred, more complications would be recorded.
The use of RARC has definitive merits in terms of wound problems. Just one case of wound dehiscence necessitating additional suturing occurred at the site of minilaparotomy for ileal neobladder formation in the RARC group, while the ORC group had 17 (16.3%) cases of wound problems. In a direct sense, robot-assisted laparoscopic surgery has advantages in terms of wound care because a smaller incision is needed to perform the operation. It is generally accepted, however, that RARC needs a longer operative time. 12,16 In this study, it also took more time to perform RARC than ORC. In the subgroup analysis according to type of diversion, however, there was no difference in ileal conduit formation between the two groups, and the difference in neobladder type between the two groups increased. The gap according to type of diversion might be because RARC requires that the robotic arm dock and redock for the manipulation of the ileal neobladder and urethroneovesical anastomosis. Taking into account the fact that our data were collected from our first experiences with RARC and the RARC group underwent ileal neobladder formation more frequently, the total operative time of the RARC group was comparable to that of the ORC group. Moreover, the total operative time still decreased.
There were three cases of urinary leakage in the RARC group, all of which occurred in the urethroneovesical anastomosis site of the neobladder. There was only one case in the ORC group, and it occurred in the ileal conduit of the ORC group. Additional urethral catheterization was needed in all three cases. Interestingly, we thought that it was somewhat more difficult to perform vesicoileal anastomosis with RARC than with ORC. In fact, the robot system was developed and spotlighted because of its ease of manipulation and reconstruction in the pelvic cavity, such as for radical prostatectomy and its urethrovesical anastomosis. This perceived difficulty could be because we had to take the neovesical segment “up” to the urethral stump against gravity because of the steep Trendelenburg position. Currently, a level or low degree of Trendelenburg position has been adopted for vesicoileal anastomosis in our center.
More UTIs occurred in the RARC group in our study. There was, however, no difference in the subgroup analysis according to the type of diversion. The ileal neobladder generally tends to be associated with more complications such as metabolic problems and UTI. 17 Indeed, 71.4% (5/7) of UTIs in the RARC group arose from the neobladder, but this was not different from the percentage of UTIs that occurred in the ORC group (62.5% (5/8), P=0.714).
We expected that the RARC group would experience less ileus; however, there was no difference between the two groups. This disappointing result could be attributed to our extracorporeal bowel manipulation. There are limited data documenting the intracorporeal type of urinary diversion performed with RARC. Research into the correlation between ileus and the type of diversion is needed.
There are several limitations to this study. First, this was a nonrandomized and retrospective comparison study, and therefore has some selection bias. ORC, however, was still an independent predictor of more complications on multivariate logistic regression analysis. Second, discrepancy in the rate of patients undergoing orthotopic neobladdder between both groups may have introduced a confounding bias to the results. Selection of healthier patients, as suggested by higher neobladder rate, may account for the lower rate of complications in the RARC group. There was no difference in terms of comorbidity, however, including renal insufficiency. Third, there were differences in the degree of experience among the surgeons. Our team had performed dozens of open radical cystectomies a year before the introduction of robot-assisted surgery, while we included data from the initial cases in which RARC was performed. Nonetheless, the RARC group had fewer complications. We expect that more RARC procedures need to be performed to achieve proficiency, and complications from RARC will consequently decrease. Last, the modified Clavien system is limited because it only reports for up to 90 days, and readmission is not counted in the score. We scored complications at the time of readmission, but the readmission itself was not regarded as a complication.
Conclusions
The results of this retrospective, nonrandomized study demonstrated that RARC results in fewer grade II or greater complications than ORC. Wound problems, EBL, and transfusion requirements were also lower in the RARC group, while a longer operative time was needed. Overall, RARC appears to be comparable to ORC in terms of early complications classified according to the modified Clavien system. Larger, randomized studies with long-term follow-up periods are still needed to confirm the feasibility and oncologic outcomes of RARC.
Footnotes
Disclosure Statement
No competing financial interests exist.