
Abstract
Duplicated renal collecting systems are a common congenital anomaly, with patients usually presenting in childhood, rarely in adult life. To our knowledge, only one case of robot-assisted heminephrectomy in adults has been described. We reviewed the medical records of four adult patients with symptomatic unilateral duplicated collecting systems and nonfunctioning upper pole renal units (NFUPRU) who underwent robot-assisted laparoscopic heminephrectomy at our institutions. Heminephrectomy for NFUPRU should be approached differently than partial nephrectomy, because of complex vascular anatomy. Patients who are undergoing this procedure have brief hospital stays, minimal morbidity, preservation of renal function, and resolution of symptoms. Robot-assisted laparoscopy is well suited for this procedure because it allows improved visualization during dissection of the unique vascular anatomy as well as scaling of surgeon movements and improved ergonomics.
Introduction
Patients and Methods
This study was performed in a retrospective fashion. After Institutional Review Board approval, we reviewed the patient records of all known adult patients at our institutions (University of Virginia, Children's Hospital Boston) who had undergone robot-assisted laparoscopic resection of NFUPRU between November 2004 and April 2010. All patients had a preoperative CT scan or MRI showing a dilated upper pole renal unit and ureter in the setting of a duplicated collecting system. Functional assessment of the upper pole unit was achieved by either CT or MR urography or radionuclide renal scan with mercaptoacetyltriglycine or dimercaptosuccinic acid. The parenchyma of the upper pole was thin and demonstrated minimal function in all patients. Patients 1, 2, and 4 had ectopic ureters with associated obstruction, whereas patient 3 had a ureterocele identified on preoperative imaging. Three of the four patients had serum creatinine measurement before and after NFUPRU removal.
Surgical technique was similar to previously described conventional laparoscopic technique. 8 Patients 1 to 3 underwent cystoscopy with retrograde ureteropyelography of the lower pole collecting system, followed by placement of a 5F or 6F open-ended ureteral catheter into the lower pole, secured to a Foley catheter. Patient 3 had a transurethral incision of the ureterocele with a Colling knife. Patients were then repositioned in the 45-degree modified flank position. Because of surgeon preference, all procedures were performed via the transperitoneal approach. Verress needle placement at the umbilicus was used to achieve peritoneal insufflation.
A 12-mm laparoscopic camera port was placed at the umbilicus (supraumbilical in patients 1–3, infraumbilical in patient 4) under direct visualization using a 0-degree laparoscope. Two 8-mm ports were placed at positions 10 cm cephalad to the camera port and 10 cm lateral to the camera port (in the direction of the affected kidney), for use with robotic arms. An assistant port was placed approximately 5 cm at the diagonal caudally and contralateral to the affected kidney, as an assistant port. In the case of a right-sided NFUPRU, a 5-mm port was placed in the subxiphoid area for passage of a liver retractor (Fig. 1).
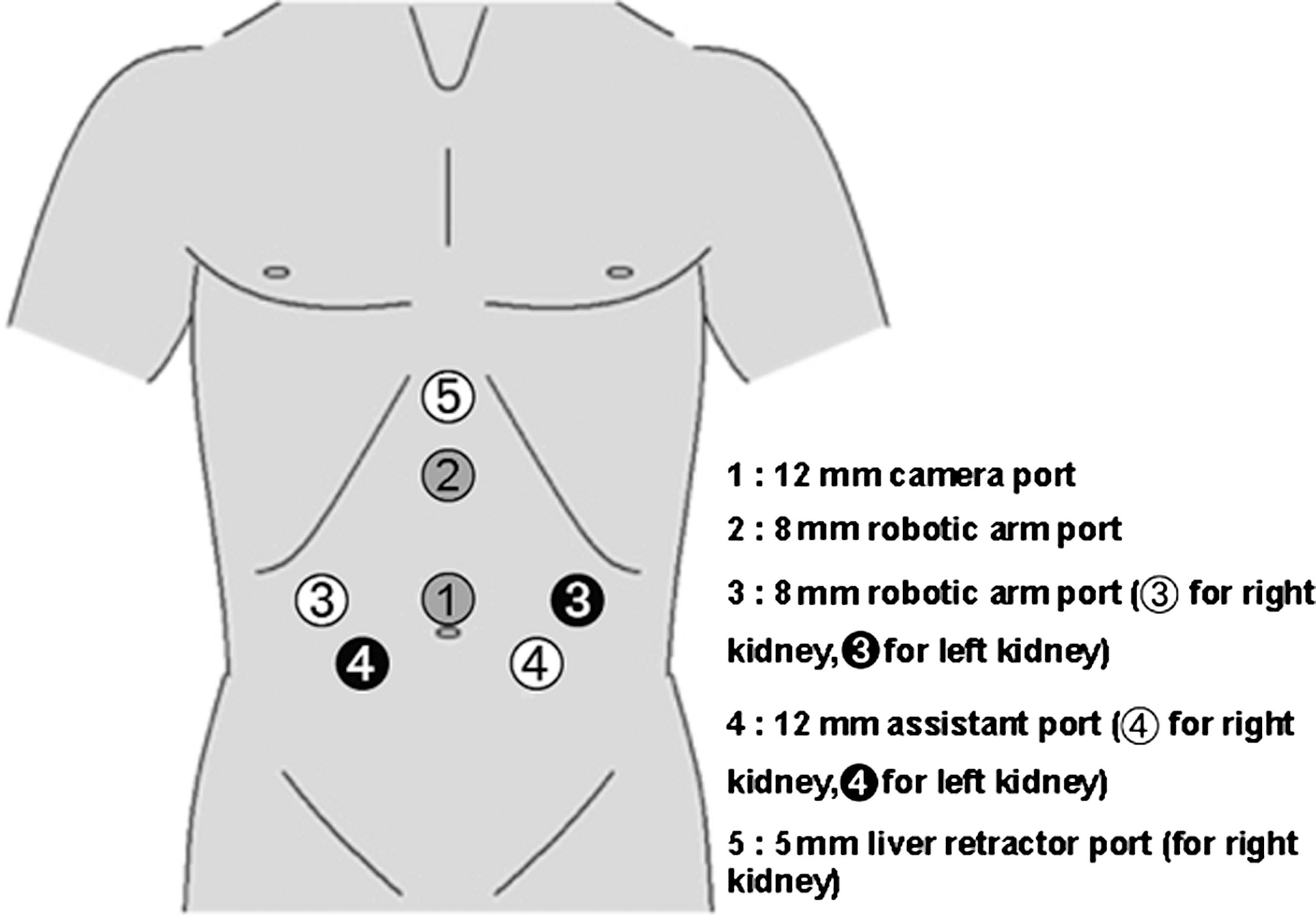
Schematic of typical laparoscopic port placement.
After docking the robot, the colon was reflected medially, and both ureters of the duplicated system were identified medial to the lower pole of the kidney. The lower pole ureter was identifiable because of the previously placed ureteral catheter. Using robot assistance, the upper pole ureter was dissected cephalad toward the upper pole renal hilum, taking care not to injure the lower pole vasculature as it crossed anterior to the upper pole ureter. No clamping of the hilum was performed—only selective vascular dissection. The upper pole vasculature was ligated using locking vascular clips.
The NFUPRU was then removed by dividing along the atrophic cleavage plane using harmonic scalpel or electrocautery, based on surgeon preference. Harmonic scalpel was used in situations where less spread of energy to surrounding tissues was desired and was applied via conventional laparoscopic instrument through an assistant port. The upper pole ureter was then dissected caudally to within 1 cm of the bladder and ligated using locking vascular clips. Methylene blue injection of the lower pole ureteral catheter was performed to evaluate for collecting system injury. Hemostasis was achieved via bipolar electrocautery and oxidized cellulose polymer. A 15F round Jackson-Pratt (JP) drain to bulb suction was placed within the surgical bed. The ureteral catheter was removed immediately postoperatively. Foley catheters were removed on postoperative day 1, and JP drains were removed on postoperative day 2 if no urine leak was present.
Results
Patient characteristics are summarized in Table 1. Patient age ranged from 32 to 56 years. The most common presenting complaint was episodic flank pain. Urine cultures from all patients showed no infection. Patient 3 presented with progressively worsening lower urinary tract symptoms (LUTS) and was found to have an associated cecoureterocele obstructing the bladder neck and proximal urethra. The other three patients did not have identification of an upper pole ureteral orifice. Patient 3 had thin parenchyma with a small amount of contrast uptake by the upper pole renal unit on preoperative CT urography, whereas all other patients had no contrast or radionuclide uptake on preoperative urography or renal scan. Preoperative imaging demonstrated the typical anatomy of lower pole renal vasculature crossing anterior to the upper pole ureter (Fig. 2).

CT urography demonstrating lower pole artery (arrow) crossing dilated upper pole ureter.
BMI=body mass index; NFUPRU=nonfunctioning upper pole renal unit.
Patient outcomes are summarized in Table 2. No intraoperative complications were encountered. The dissection of the unique vascular anatomic arrangement was achieved easily with robot-assisted dissection (Fig. 3). Parenchymal thinning and hydronephrosis of the NFUPRU was discernible from the normal-appearing lower pole moiety. Mean operative time was 310 minutes (range 240–400 min). Mean estimated blood loss was 310 mL (range 80–1200 mL). In patient 3, the demarcation between the NFUPRU and lower pole was not readily apparent, and the lower pole parenchyma was entered, accounting for increased blood loss. Mean length of hospital stay was 2.3 days (range 2–3 days). Mean postoperative estimated GFR (92 mL/min) was not significantly different from the preoperative value (91 mL/min). No postoperative complications were encountered, including urine leak, in any patient. Mean follow-up was 13 months (range 9–19 months). Patient 1 had resolution of her flank pain and improvement but not complete resolution of her urge incontinence. All other patients had complete resolution of their presenting symptoms.
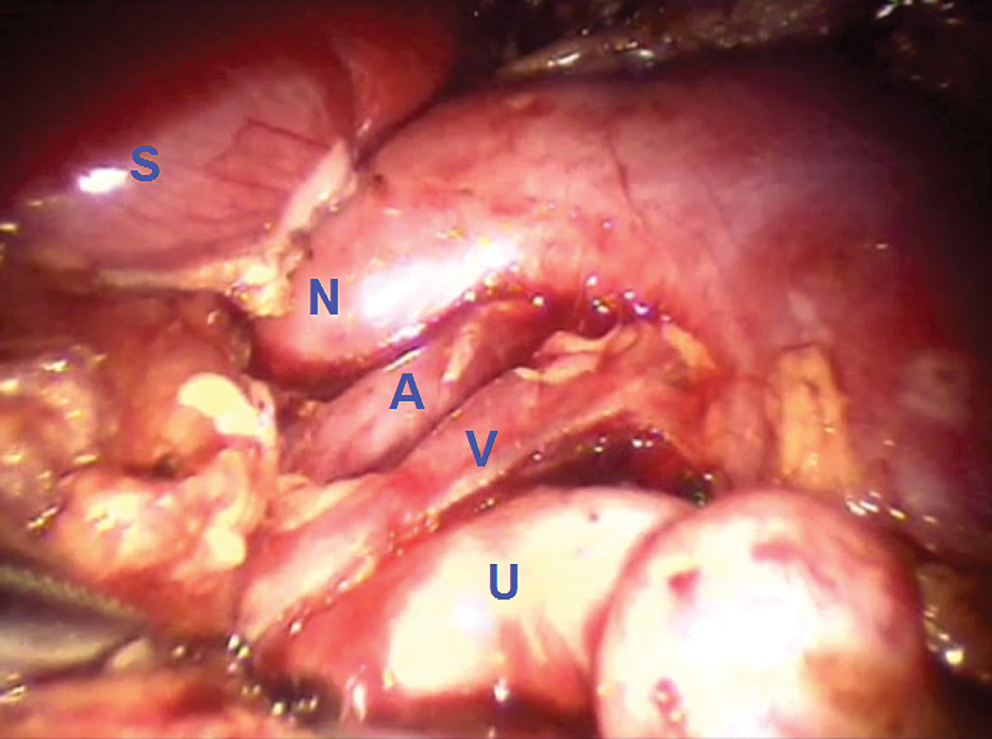
Spleen
EBL=estimated blood loss; GFR=glomerular filtration rate; preop=preoperative; postop=postoperative.
Discussion
Duplicated renal collecting systems are a common urologic abnormality. Patients with upper pole renal units with associated obstruction usually present in childhood with prenatal detection or with infection and flank pain. Rarely do obstructed upper pole units go unnoticed until adult life, at that point presenting as NFUPRU with a variety of symptoms including hematuria, flank pain, and LUTS. In our series, no patients presented with infection, although this is reported in the literature as one of the most common presentations. 1 Conventional treatment for symptomatic NFUPRU is heminephrectomy. Laparoscopic heminephrectomy has previously been described in the literature for both pediatric 2 –7 and adult patients. 8
We performed robot-assisted heminephrectomy and near-total ureterectomy for NFUPRU in four adult patients. This was performed in a manner similar to the conventional laparoscopic technique described by Abouassaly and associates, 8 with modification to include near-total ureterectomy in all patients, and use of the robot for hilar dissection. Because of the complex vascular anatomy, heminephrectomy for NFUPRU should be approached differently than partial nephrectomy for tumor. Robot-assisted laparoscopy is well suited for this procedure because it allows for excellent visualization and meticulous dissection of duplicated renal vasculature. Figure 4 shows a schematic of the typical anatomy. Vascular patterns can be highly variable and may include multiple branches from the main lower pole vessels.
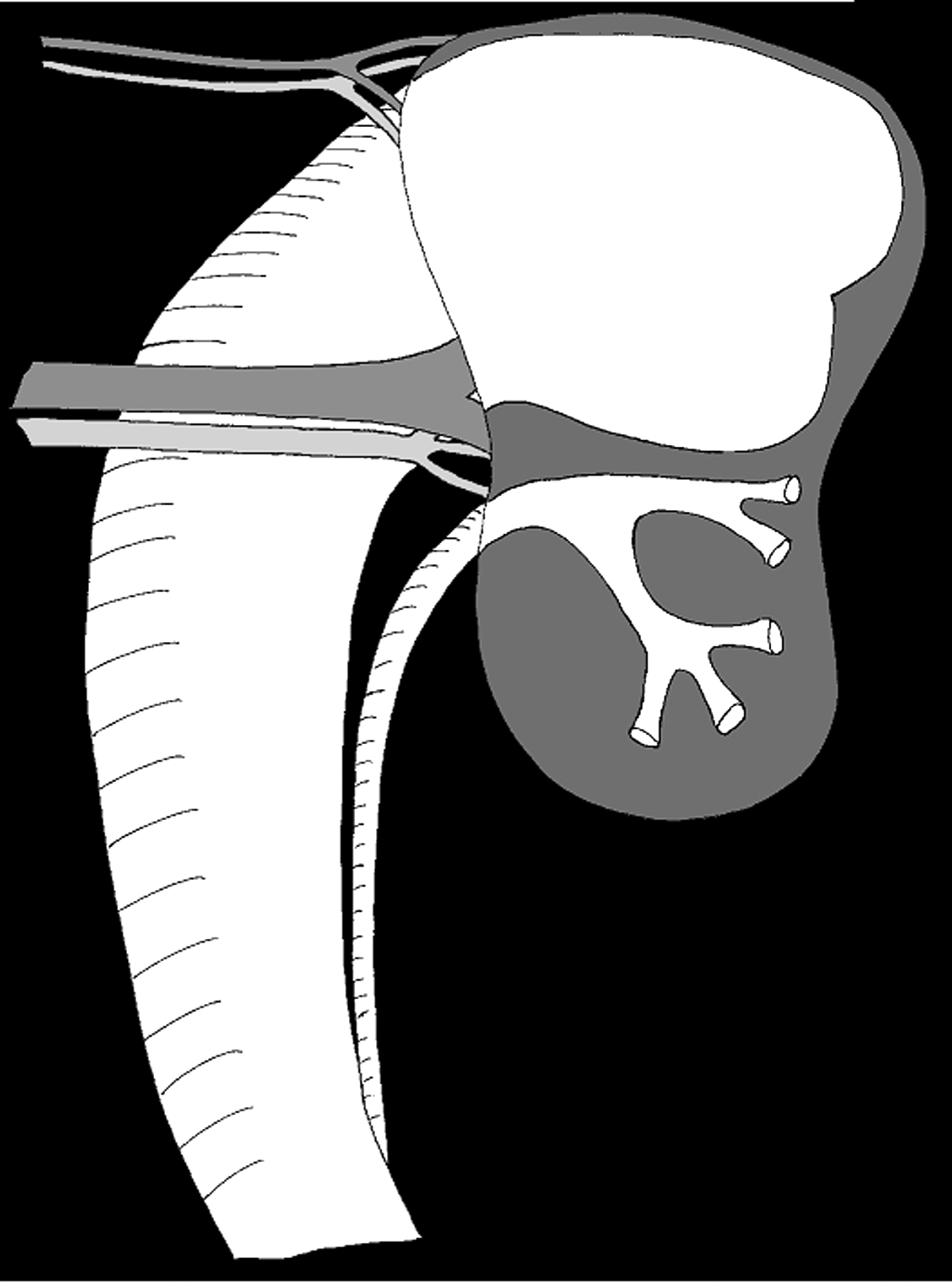
Schematic of typical vascular and ureteral anatomy.
We chose a transperitoneal approach to this surgery, because of surgeon preference. The literature has described benefits of both the transperitoneal and retroperitoneal approach. After a study of adults undergoing partial nephrectomy for tumor, Ng and colleagues 10 stated their preference for the transperitoneal approach because of the larger working space and improved instrument angles. In children undergoing partial nephrectomy for NFUPRU, the transperitoneal approach has been attributed with larger working space and more familiar anatomy for most surgeons, whereas the retroperitoneal approach allows a shorter working distance to the kidney and a theoretical reduction in formation of intra-abdominal adhesions. 11
The skills necessary to perform this surgery are likely possessed by most surgeons who regularly perform robotic renal procedures, such as pyeloplasty or partial nephrectomy for tumor. We think that the procedure we describe uses the same surgical skill set, and it is likely to be a smooth transition to this procedure for surgeons with robotic renal surgical experience.
Table 3 compares the results of our study with a conventional laparoscopic surgical series in adult patients. Our series shows similar efficacy and safety of the robot-assisted laparoscopic approach. There is increased operative time associated with the robotic procedure, because of additional equipment, docking and undocking of the robot, and changing instruments.
EBL=estimated blood loss.
Cost of robotic surgery is significant, with mean hospital billing amount in our series of $43,980 (total operating theater and anesthesia cost accounting for $40,157 with the remainder attributed to hospital stay). Robot-assisted laparoscopy, however, allows for better visualization (with regard to depth perception and magnification), scaling of surgeon movements, and improved ergonomics. 12 Overall, we think the benefit of the robotic approach for this procedure is equal to that of conventional laparoscopy and is a valid alternative for surgeons more comfortable with robotic surgery.
Conclusions
Heminephrectomy for NFUPRU should be approached differently from partial nephrectomy for tumor, because of the complex vascular anatomy. Patients who are undergoing this procedure enjoy brief hospital stays, minimal morbidity, preservation of renal function, and resolution of symptoms. Robot-assisted laparoscopy is well suited for this procedure because it allows improved visualization during dissection of the upper pole collecting system and ureter as it crosses posterior to the lower pole vasculature, as well as scaling of surgeon movements and improved ergonomics.
Footnotes
Disclosure Statement
No competing financial interests exist.