
Abstract
Purpose:
To compare operative and functional outcomes of minimally invasive partial nephrectomy (MPN) and minimally invasive radical nephrectomy (MRN) for T1b and T2a renal tumors.
Patients and Methods:
All patients who underwent MPN or MRN for a localized, solitary renal mass 4 to 10 cm were included. Perioperative and renal function outcomes were compared. Propensity analysis was used to account for selection bias in type of nephrectomy when evaluating complication rates.
Results:
One hundred and eight patients underwent MRN and 45 underwent MPN between August 2004 and September 2010. Preoperative patient and tumor characteristics were similar between groups. Tumor size was larger in the MRN group (5.3 vs 6.8 cm, P<0.001). Operative times and positive margin rates were similar between the groups (P=0.956 and P=0.207, respectively). Estimated blood loss was higher in the MPN group (401.8 vs 157.1 mL, P<0.001), but transfusion rates were similar (P=0.225). Rates of intraoperative (P=0.724), postoperative (P=0.806), and high Clavien-grade postoperative complications (P=0.966) were similar. Propensity analysis indicated that the likelihood of any complication (odds ratio [OR] 0.810, confidence interval [CI] 0.331–1.982, P=0.645) or of a high-grade complication (OR 0.164, CI 0.011–2.513, P=0.194) was unrelated to type of nephrectomy. With similar preoperative renal function parameters, postoperative development of new stage III to V chronic kidney disease (CKD) was greater in the MRN group (58 vs 31%, P=0.011). Propensity analysis showed that the likelihood of new CKD was 2.8 times higher in the MRN group (P=0.048).
Conclusion:
In selected patients and with appropriate surgical expertise, MPN can result in similar rates of complications but superior renal function outcomes in larger kidney tumors.
Introduction
Although minimally invasive partial nephrectomy (MPN) requires advanced technique, the advantages are appealing to both patients and hospitals. Minimally invasive approaches for radical nephrectomy are widely accepted and preferred to open approaches for large localized tumors because of quality-of-life benefits, including shorter hospital stay, decreased pain, and improved cosmesis. 2
Recently, the use of MPN for larger tumors is on the rise at centers of excellence but has yet to be implemented as standard of care because of the advanced skill required, the potential for surgical complications, and uncertainty of oncologic equivalence. 3 –5 The advantages of NSS likely extend to larger tumors, but data on minimally invasive management of larger kidney tumors are relatively scarce. To further investigate this, we compared surgical and renal function outcomes of MPN with those of minimally invasive radical nephrectomy (MRN) for localized renal tumors 4 to 10 cm (T1b to T2a). These tumors are of particular interest because they present a significant surgical challenge, especially in a laparoscopic or robot-assisted setting. We therefore set out to investigate the perioperative and functional outcomes of minimally invasive kidney surgery in this patient population.
Patients and Methods
From our prospectively collected, Institutional Review Board-approved kidney tumor database, we identified all patients who underwent MPN or MRN from August 2004 to September 2010, for a clinically localized, solitary renal mass of 4 to 10 cm. All tumors were restaged according to the 7th edition of the American Joint Committee on Cancer Cancer Staging Manual 6 such that this size cutoff included all T1b and T2a tumors. Exclusion criteria included metastatic disease at presentation and absence of a normal contralateral kidney (including bilateral disease).
Of the 640 patients in the database, 153 patients met inclusion criteria, 108 and 45 of whom underwent MRN and MPN, respectively. All cases were performed by three surgeons (HK, WU, TS) with the surgical approach and type of nephrectomy being at their discretion. Nephron sparing was generally the primary goal with a minimally invasive operation as a secondary goal.
Clinicopathologic data were recorded, including patient age, sex, race, smoking status, number of previous abdominal surgeries, body mass index (BMI), Charlson Comorbidity Index (CCI), American Society of Anesthesiologists status, and tumor size. Tumor centrality and R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score were retrospectively included with blinding to procedure performed and were thus available for 44 of MPN and 65 of MRN groups (109 total). 7
Surgical outcomes were compared between the two groups, including operative time, estimated blood loss (EBL), transfusion rate, length of stay (LOS), positive surgical margin (PSM), and complications (including conversions). Complications were recorded as any deviation from the normal postoperative course within 30 days of operation (including outpatient data) and are presented according to the 10 criteria outlined by Martin and associates. 8 Complications were categorized according to the Memorial Sloan Kettering system and graded using the Clavien-Dindo grading system. 9,10 Anemia was defined as the need for postoperative blood transfusion, and ileus was defined when delay in bowel function prolonged the hospital stay or necessitated placement of a nasogastric tube.
Renal function outcomes were also compared, including postoperative decrease in the estimated glomerular filtration rate (eGFR), as calculated using the CKD Epidemiology Collaboration formula, 11 and development of new stage 3 to 5 CKD according to the National Kidney Foundation Practice Guidelines. 12 Postoperative decline in eGFR was calculated using creatinine level measured at the most recent postoperative visit beyond 30 days after surgery.
Continuous variables were compared using the Student t test or Wilcoxon rank-sum (for non-normally distributed variables), and categorical variables were compared using either chi-square analysis or the Fisher exact test where appropriate. A P value<0.05 was considered statistically significant. All analyses were performed using Stata statistical software, version 11.0 (StataCorp, College Station, TX).
To account for selection bias inherent in this non-randomized population, propensity analysis was undertaken. 13 Probability of undergoing MRN was calculated using multivariable logistic regression including those preoperatively available variables that could influence selection for type of nephrectomy (age, sex, race, smoking status, BMI, CCI, tumor size, and preoperative creatinine level). Patients were then assigned a propensity score based on quintile of the probability of undergoing MRN. Odds ratios for any complication, high-grade complications, and development of new postoperative stage 3 to 5 CKD by type of nephrectomy were recalculated using logistic regression, adjusting for the propensity score.
Results
Of the153 patients meeting inclusion criteria, 45 (29%) underwent MPN and 108 (71%) underwent MRN. MRN was completed laparoscopically in 104 (96%) patients and with robot assistance in 4 (4%) patients. MPN was completed laparoscopically in 25 (56%) patients and with robot assistance in 20 (44%) patients. Demographics were similar between the groups (Table 1). Tumor size was larger in the MRN group vs the MPN group (6.8±1.7 cm vs 5.3±1.3 cm, P<0.001). There was a higher rate of central tumors in the MRN group (97% vs 84%, P=0.029), but mean R.E.N.A.L. scores were similar (9.3 vs 9.7 in the MPN vs MRN groups, P=0.159). Operative times and LOS were similar between the groups (P=0.956 and P=0.151, respectively). Focally positive margins were found in two patients and one patient in the MPN vs MRN groups, respectively (P=0.207). Mean EBL was higher in the MPN group (401.8 vs 157.1 mL, P<0.001). Intraoperative (P=0.136) and postoperative (P=0.225) transfusion rates, however, were similar between the two groups.
Total number of previous abdominal and pelvic surgeries.
Central tumor defined as abutting the central sinus fat or collecting system on preoperative CT scan.
MPN=minimally invasive partial nephrectomy; MRN=minimally invasive radical nephrectomy; SD=standard deviation; BMI=body mass index; ASA=American Society of Anesthesiologists; R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location.
A total of 39 patients experienced 45 postoperative complications. Rates of complications were similar between the MPN and MRN groups (Table 2), including intraoperative (4.4% vs 7.4%, P=0.724) and total postoperative complications (26.7% vs 24.8%, P=0.806). Of those patients, 11 and 23 experienced a single postoperative complication, 1 and 3 experienced two postoperative complications, and 0 and 1 experienced three postoperative complications in the MPN and MRN groups, respectively (P=0.950). High Clavien grade (III and IV) complications were seen in two and four patients in the MPN and MRN groups, respectively (P=0.966). There were no Clavien grade V complications. The systems involved in the postoperative complications are included in Table 3 (P=0.740).
MPN=minimally invasive partial nephrectomy; MRN=minimally invasive radical nephrectomy; SD=standard deviation; WIT=warm ischemia time; EBL=estimated blood loss; PSM=positive surgical margin; Cxs=complications; POC=postoperative complication; LOS=length of stay.
MPN=minimally invasive partial nephrectomy; MRN=minimally invasive radical nephrectomy.
In the MPN group, one patient each experienced urine leak and arteriovenous fistula (which necessitated interventional embolization). Mean warm ischemia time (WIT) in the MPN group was 23.6±9 minutes (three MPN performed unclamped were excluded from the mean). There were two conversions from partial to radical nephrectomy for oncologic reasons, one of which was also converted to open while the other was completed robotically. One additional MPN was converted to open partial nephrectomy because of difficulty accessing the tumor and bleeding from an unclamped accessory renal artery. Of the MRNs, one patient's procedure was converted to hand-assist because of difficulty with liver retraction, and one patient's operation was converted to open radical because of bleeding from the renal vein stump from stapler malfunction.
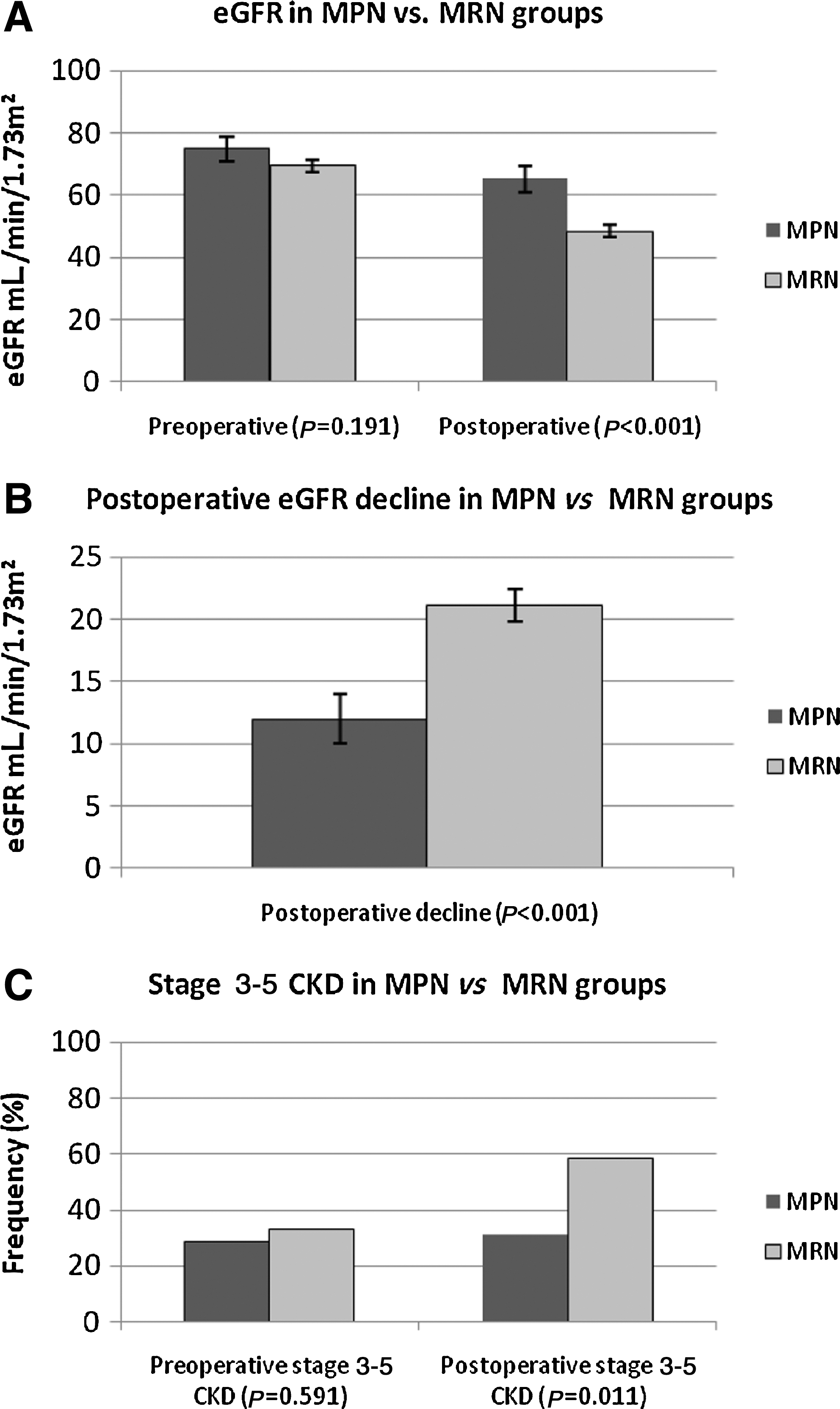
Preoperative eGFR was similar in the MPN vs MRN groups (74.9 vs 69.5 mL/min/1.73m2, P=0.191) with stage 3 to 5 CKD seen in 13 (29%) vs 36 (33%) patients, P=0.591. Postoperative decline in eGFR was significantly greater in the MRN group compared with the MPN group (21.1±12.9 vs 12.0±13.2 mL/min/1.73m2, P<0.001), resulting in a greater rate of new stage 3 to 5 CKD at 58% vs 31%, respectively (P=0.011), as shown in Figures 1A–C.
Propensity analysis indicated that likelihood of any complication or of a high-grade complication was not related to type of nephrectomy (MRN odds ratio [OR] 0.810, confidence interval [CI] 0.331–1.982, P=0.645 and OR 0.164, CI 0.011–2.513, P=0.194, respectively). Likelihood of development of new stage 3 to 5 CKD, however, was 2.8 times higher in the MRN group (P=0.048).
Discussion
NSS for tumors ≤4 cm is the standard of care as recommended by current AUA guidelines, because it results in a decreased risk of renal insufficiency and subsequent decreased risk of cardiac morbidity, hospitalization, and death related to CKD. 14 –17 Because of the potential survival advantage, indications for NSS are expanding. 17,18 Minimally invasive surgical techniques have much appeal, but require extensive surgical skill and may be associated with more complications. 19 MPN may be more difficult with tumors >4 cm because of difficulty in obtaining adequate access, less working space, more vessel involvement, and distortion of normal anatomy.
We investigated tumors up to T2a, because larger tumors are very difficult to manage using minimally invasive technique simply from size constraints. Therefore, tumors ≥T2b are usually managed with open approaches at our institution and were not included in this analysis. It is important to critically examine perioperative outcomes of MPN compared with the reference standard MRN, however. Our study supports the safety and efficacy of MPN in larger kidney tumors, including stages T1b and T2a.
Accounting for selection bias through a propensity analysis, we have demonstrated that the rates of any complication or high-grade complications were similar between MRN and MPN. Simmons and colleagues 4 compared laparoscopic partial nephrectomy (LPN) in smaller and larger tumors and found a rate of 24% total postoperative complications in tumors >4 cm, which is comparable to the 26.7% rate found here. This rate as well as rates of intraoperative complications were shown to be similar to those with tumors ≤2 cm and 2 to 4 cm. 4 Our standardized comprehensive report of complications of the two minimally invasive procedures further supports the safety of MPN for tumors 4 to 10 cm with similar rates of intraoperative complications, rates of multiple postoperative complications, and systems involved with postoperative complications.
Although EBL was higher in the MPN group, intraoperative and postoperative transfusion rates were similar, calling into question the significance of this finding. Patard and coworkers 20 depicted in a retrospective, multicenter study that there was a higher risk of hemorrhage, blood transfusion, and urinary fistulas in partial nephrectomies in tumors >4 cm, but these results did not show significantly higher rates of medical and surgical complications.
Open partial nephrectomy has been used for tumors >4 cm in appropriately selected candidates. 14 Minimally invasive approaches are more attractive to both patients and healthcare facilities, and there is a growing effort to use these techniques. Literature is scarce on use of MPN for larger tumors, however. Some data exist suggesting similar preservation of renal function outcomes in smaller and larger tumors with NSS and worse renal function outcomes with radical surgery in larger tumors, in terms of rates of new onset CKD and postoperative eGFR decline. 4 Simmons and associates 5 demonstrated that laparoscopic radical nephrectomy (LRN) resulted in a decrease in postoperative GFR of 24 vs 13 mL/min and more one-stage and two-stage CKD progression compared with LPN in tumors >4 cm.
We found a similar significantly larger decrease in eGFR and a >20% difference in new onset stage 3 to 5 CKD in the radical group, thus substantiating these findings. The propensity analysis further supports the superior preservation of postoperative renal function with partial vs radical excision. This is likely because even in larger tumors, MPN can be performed with a low WIT. The mean WIT in this series compares favorably with most published series. 4,5,14,18,19
Given the retrospective nature of this analysis, selection bias was inherent in which patients were chosen for MPN. The propensity analysis, however, would account for most variables thought to influence selection for type of nephrectomy. Other unrecognized or unavailable variables not included in propensity analysis may have also had effect. The sample size of the MPN cohort is small, but other series have had similarly low numbers of patients undergoing MPN for tumors >4 cm, thus demonstrating the difficulty of this procedure and importance of proper patient selection with larger tumors. 4,5 In addition, limited follow-up precluded a meaningful analysis of oncologic outcomes. Intermediate-term oncologic outcomes in LPN and LRN for tumors >4 cm have been shown to be similar in the past. The PSM for this series is comparable to previous reports, which may be an indicator for oncologic outcomes. 5
Future studies should focus on oncologic equivalence with long-term follow-up before MPN in larger tumors can be universally adopted. Our results represent outcomes at a tertiary referral center and may not be applicable to a general urology practice. Nonetheless, we believe that our results further support the safety of MPN for larger renal masses and the superiority in preservation of kidney function over radical surgery with proper patient selection.
Conclusion
MPN has a role in the management of larger renal masses. In selected patients and with appropriate surgical expertise, MPN can result in similar rates of complications but superior renal function outcomes in tumors between 4 and 10 cm.
Footnotes
Disclosure Statement
No competing financial interests exist.