
Abstract
Background and Purpose:
Endoscopic lithotripsy is often prolonged secondary to the retrograde migration of calculous fragments. Various balloons, baskets, and other devices have been used to prevent this migration. Our purpose is to analyze the effect of the Accordion® on stone migration and overall efficiency during lithotripsy.
Patients and Methods:
We prospectively evaluated 21 patients with a total of 23 distal ureteral stones. Patients underwent lithotripsy using an endoscopic impact lithotriptor. The Accordion was randomly used in 11 of these 21 patients. Data were collected regarding stone migration, stone size, stone ablation, ureteral clearing, and lengths of time for various stages of each procedure.
Results:
Patients who were treated with the Accordion device experienced significantly less retrograde migration during fragmentation (P=0.0064). When stone volume was taken into account (but not on a per stone basis), ablation and ureteral clearing were also expedited, and fewer lithotripter “hits” and basket “sweeps” were needed.
Conclusion:
The Accordion device is effective in preventing the migration of stone fragments during endoscopic ureteral lithotripsy. Our data suggest that this device may also increase efficiency of the fragmentation and clearance of ureteral calculi.
Introduction
Patients and Methods
We prospectively evaluated and treated 21 patients with a total of 23 distal ureteral stones at the University of Assiut, in Assiut, Egypt, in collaboration with 12 members of the department of urology. The study was designed and accomplished with the approval of the Investigational Review Board of the host institution.
Patients with distal ureteral calculi were eligible for the study. The diagnosis of ureteral calculi was made based on the patient's history and radiographic studies, including plain radiography of the kidneys, ureters, and bladder (KUB), excretory urography, or CT. The patient's medical and surgical history were noted.
All stones were confirmed and measured on the KUB. The width and height of each calculus was recorded for volume calculations. The volume was calculated from the two measurements using a formula for a prolate spheroid. The depth of the stone was assumed to be the same as the medial-lateral measurement.
All non-pregnant patients with distal ureteral calculi were eligible for the study. They were fully informed of the study in their own language by a member of the study team. The patients were randomized to treatment without or with the use of the Accordion by record number.
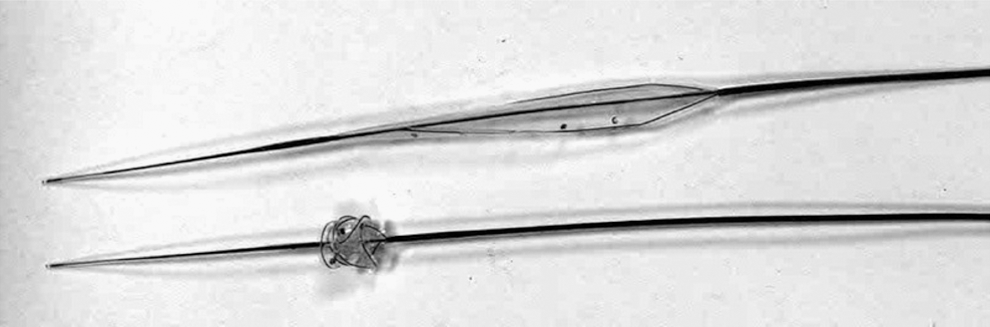
The Accordion device has a central wire shaft within a 3F sheath. There is an occlusive film (7 or 10 mm in diameter) that can be deployed, once in the appropriate position, by moving the central wire within the sheath to shorten the segment at the film to form the Accordion (Figs. 1A, 1B). Basically, the central pull wire can shorten the distance between the proximal and distal extent of the film to form it into the occlusive mass.
The device is placed into the patient's ureter through the working channel of a cystoscope. In this study, a safety wire was used in every patient. Proper placement proximal to the stone to be treated is ensured by fluoroscopic visualization. Radiopaque markers on the edge of the film indicate its position. The device is then deployed to expand its overall configuration to a 7 mm or 1 cm diameter semisolid cylinder (Fig. 2). In patients with widely dilated ureters, the device can be used to sweep the stone to a more distal location where occlusion can take place. In this study, once ureteroscopy was performed, the true occlusion of the ureter by this device could be noted visually.
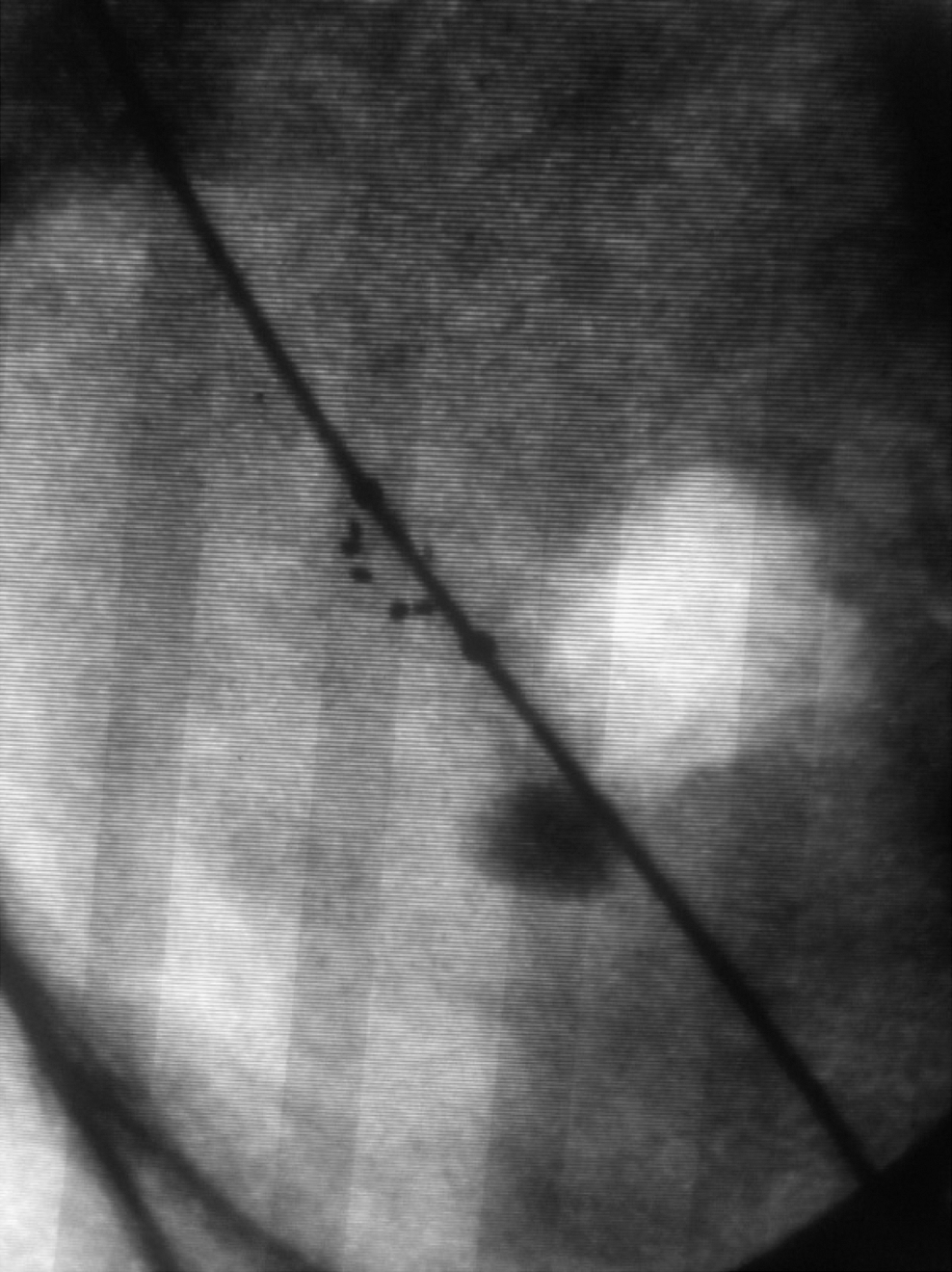
Markers on the Accordion® are visible fluoroscopically and demonstrate its position proximal to the large distal ureteral calculus.
All calculi remained in situ for treatment. None was displaced during the initial manipulation with a wire or Accordion. The semirigid ureteroscope was used to access all stones. The calculi were fragmented with a pneumatic impact lithotriptor (Stone Breaker,™ Cook Urological, Spencer, IN) until all remaining pieces were <1 mm in diameter, or were easily basketed with a 3.0 or 4.0F Nitinol basket, either a Dormia or Dimension (CR Bard, Covington, GA) style. In patients in whom the Accordion was used, attempts to “sweep” fragments of calculi from the ureter were made before basketing was initiated. Fluoroscopy was used to locate the calculus and anatomic landmarks before and after lithotripsy and before basketing and/or sweeping was attempted. The distance between the initial and final locations of the stone on fluoroscopy or radiography was measured with calipers.
In addition to calculus migration and size, data were collected regarding the number of lithotripter hits needed for fragmentation, the total number of basket and Accordion sweeps, the total amount of time spent fragmenting calculi, time spent clearing the ureter of fragments, and total operative time (cystoscopy to stent placement).
The associates in the department of urology, Assiut University, were the primary endoscopists, with a member of the study team always in attendance. Therefore, a relatively inexperienced endourologist who was familiar with neither the lithotriptor nor the Accordion was always the operator. We noted that most of the movement observed resulted from pushing the stone with the scope and the probe of the lithotriptor, not from the lithotriptor itself.
Results
A total of 21 patients included 14 males and 7 females. The average age was 41.8 years. There were 17 patients with single ureteral calculi and 4 with multiple calculi in the same ureter. Ipsilateral surgical history included six patients with previous ureteroscopy, two with previous stents, two with previous shockwave lithotripsy, three with previous percutaneous nephrolithotomy, and six patients with previous open lithotomy.
Before fragmentation, 14 patients needed ureteral dilation secondary to ureteral strictures. Open-ended catheters were used in 8 patients, dual lumen catheters in 11, and 5 patients underwent balloon dilation (to 5 to 6 mm in diameter) with pressures ranging from 6 to 24 bars. These narrowings may have occurred with a long duration of stone impactions or even from a history of schistosomiasis.
Although a total of 21 patients were treated initially; 20 patients with 21 distal ureteral calculi were included in our final calculations. One patient was not included because a basket was used to hold two calculi in place during fragmentation.
Stones in the Accordion group were larger than in the control group (Table 1). There were an average greater number of lithotripter hits (86.6 vs 65.5) and basket sweeps (6 vs 5.2) needed on patients in whom the Accordion was used. When volume is taken into consideration, however, fewer hits and fewer basket sweeps per mm3 of stone were needed (Table 2). Similarly, the average time for lithotripsy (9.7 vs 6.7 min) and basketing and sweeping (6.7 vs 6.3 min) was higher in the Accordion arm. When volume was taken into consideration, however, fewer minutes were needed for both ablation and ureteral clearing (Table 3). The average operating room time was 56 minutes in the Accordion group, and 50.4 minutes in the control group.
Avg=average.
Avg.=average.
Volume is in mm3 and time in minutes unless otherwise specified.
P value determined using a one tailed t-test comparison of means.
Avg=average.
The average stone migration with the Accordion device was 0.68 mm, compared with 35.5 mm in the control group (P value of 0.0064). No stones migrated beyond the reach of the rigid ureteroscope. If this had occurred, the times would have been widely altered. In the control group, a basket or grasper was used to reposition stones as they migrated too far proximally.
In one patient, the Accordion device was able to sweep all ureteral fragments sufficiently without the need for a basket.
Discussion
Ureteroscopy has assumed a major role in the treatment of ureteral calculi. Stones that are too large to be removed intact must be fragmented first. During endoscopic lithotripsy, there is often proximal migration of the calculus. 4 –6 During the initial experience with ultrasonic lithotripsy, it was necessary to secure the stone with a basket. 1 Other lithotripsy devices, including impact and lasers, have also caused proximal migration of the calculus. This has proven to be more of a problem when only rigid ureteroscopes are available and it is impossible to proceed to follow the calculus into the renal pelvis and intrarenal collecting system with a flexible endoscope. Proximal migration may be more problematic in managing stones that are located in the mid or proximal ureter where it is more likely that the stone can move into the intrarenal collecting system. Various devices and techniques have been used previously to prevent migration. In the present study, we have used the Accordion device with rigid ureteroscopy and impact lithotripsy.
The Accordion prevented the migration of calculi and fragments during the treatment of those patients with the impact device. Average stone migration was changed from 35.5 mm to only 0.68 mm with use of the Accordion (Table 2). Most movement appeared to result from the urologist touching the stone with the lithotripter probe. There was little movement from the impact of the device itself. The Accordion prevented proximal migration from either mechanism. Studies in vitro have shown that the Accordion effectively prevents stone migration during pneumatic or laser lithotripsy. 7,8 Migration was altered from 3.7 to 7.5 cm to <2 mm with use of the Accordion. A similar effect preventing stone migration with pneumatic lithotripsy has been demonstrated in vivo. 7
In this study, we chose to use an impact lithotriptor because of the wide availability of these devices throughout the world. These lithotriptors are essentially limited to rigid endoscopes because there are no satisfactory and functional flexible probes available to be used in a flexible ureteroscope. There is less movement of stones with holmium laser lithotripsy, yet movement is always seen. We have noted both in this series and in training courses with the holmium laser that much of the stone movement observed occurs when the probe or laser fiber touches the stone and moves it. It does not occur solely from the lithotripsy procedure. We expect that the Accordion can similarly prevent proximal migration of stones fragmented with any device and have used it successfully clinically with the holmium laser outside this study.
Other devices have also been used to prevent the retropulsion of calculi during lithotripsy. The Stone Cone™ (Boston Scientific, Natick, MA) is a device that consists of an inner wire and outer radiopaque catheter. The cone portion is formed by an internal stainless steel wire wound with a strand of nitinol molded to produce a spiral form. It is straight while located within the catheter but can be advanced to assume its spiral form. It has been reasonably successful in reported series to prevent retropulsion of calculi. 9,10 Urologists have anecdotally commented on the difficulty in opening the device to its active position effectively.
The NTrap® (Cook Urological, Spencer, IN) device has a 2.6F shaft with a 7-mm deployable backstop composed of 24 interwoven nitinol wires to be placed proximal to the site of ureteral endoscopic lithotripsy. It has also been reported to have success in preventing retrograde movement of calculi. 11
Balloons such as a Fogarty have been used in an attempt to obstruct the ureter and prevent proximal migration. Experience with balloons during the initial studies with endoscopic ultrasonic lithotripsy proved that they were not effective. 1 The round, elastic design of the balloon allowed even large stones to pass around it.
Others have attempted to obstruct the ureter proximal to the stone with materials that can be washed out subsequently. Lidocaine jelly has been used. 12 More recently, a thermosensitive gel that is affected by temperature to become more or less soluble has become available. 13
It has been suggested that the Accordion can be used to “sweep” stone fragments from the ureter. In our series, it was helpful to reposition stone fragments—specifically, to reposition stones in a dilated ureter or to bring fragments into closer proximity to the distal ureter for lithotripsy. In this way, it was helpful in all patients. In only 1 of 10 patients who were treated with the Accordion, however, could the fragments be fully swept without the need for a basket. We did note that fragments could be moved easily until they reached a narrowing in the ureter. If the stone had caused a ring of edema or if there were strictures, then stone fragments would not pass beyond that. It was also more difficult to sweep the fragment through the intramural ureter.
During manipulation with the device, both in sweeping and engaging stones, we did not note any urothelial damage. In a previous study using an in-vitro model, the Accordion device produced less maximal force than the Stone Cone when pulled past a stricture with an impacted stone (0.67 vs 1.13 newtons). 14 In the same study, the NTrap was unable to release or to pass by the impacted calculus. The elasticity of the Accordion device may make it a safer stone “sweeper.” Other studies have also noted a difference in the stiffness of the tip, the radial dilation, and axial extraction force. Those were minor differences of unknown clinical significance. 15
Because the holmium laser is frequently used for endoscopic lithotripsy, its effect on various occlusion devices has been studied. Vejdani and associates 16 demonstrated a marked difference in the number of laser firings tolerated by the devices before failure. It took only 2 pulses to break the NTrap to prevent its closure while it took 28.6 for the Stone Co. The Accordion remained operable after 100 laser firings. The outer catheters were relatively more resistant, necessitating several seconds of laser activity at 8W to break the shaft. 16
Another benefit observed during the use of the Accordion is that with the proper irrigation, stone fragments are flushed out of the ureter during lithotripsy. Proximal migration is obstructed by the device, and with irrigation fragments may “rebound” off the device, creating a suspension of stone fragments and a flush of fragments into the distal ureter or bladder. This may explain why fewer basket sweeps per volume of stone were needed in our series of patients treated with the Accordion. Similarly, this flushing effect may also improve visibility, rendering lithotripsy more accurate and efficient.
This series demonstrates the ability of the Accordion to obstruct the ureter and prevent retrograde migration of calculi during impact lithotripsy. When considered on the basis of the stone volume, those treated with the Accordion were removed with fewer passes of a basket and in a shorter time. Because the stones in the Accordion group were actually larger than those in the control group, there might be a greater possibility of fragment migration. Thus, even with a bias against the study group, the Accordion prevented proximal migration. Although this study is somewhat complicated because it was not a single surgeon with a single technique, there was some standardization with the participation of the authors in each case. It also demonstrates the efficacy of the device when used by relatively inexperienced urologists.
Conclusion
The Accordion device effectively occludes the ureter and prevents the retrograde migration of stone fragments during endoscopic impulse lithotripsy in the distal ureter. The device may also increase the efficiency of stone ablation and fragment clearance.
Footnotes
Disclosure Statement
No competing financial interests exist.