
Abstract
Background and Purpose:
Gonadal vein angioembolization is a successful means of primary and salvage treatment for symptomatic varicoceles. We aim to investigate angiographic findings during embolization of primary varicoceles vs those with failed surgical ligation.
Patients and Methods:
Between 1992 and 2010, 106 cases referred to our interventional radiologists for primary or salvage varicocelectomy were reviewed. These patients underwent venography and gonadal vein embolization using a combination of embolization coils and vascular plugs. All images were reviewed by an interventional radiologist to determine the anatomic etiology of the varicocele. Primary and salvage embolization cohorts were compared using t test and chi-square analyses for continuous and categorical variables, respectively. Angiographic parameters were analyzed using univariate and multivariable regression models to determine significance in predicting primary vs salvage status.
Results:
Of the 106 patients, 46 patients (57 testicles) underwent primary and 60 patients (62 testicles) underwent salvage embolization. The salvage cohort of patients was younger (P<0.001) and comprised more solely left-sided pathology (P=0.002). An equivalent number of gonadal vein divisions and proportion of patent gonadal veins was found. However, there was a significantly higher proportion (27.8% vs 6.7%) of inguinal collateral vessels and combined presence of inguinal and retroperitoneal collateral veins (8.5% vs 2.1%) identified in the cohort undergoing embolization after failed surgical varicocelectomy. Presence of inguinal collaterals (P=0.008) as well as presence of both inguinal and retroperitoneal collaterals (P=0.038) on multivariable regression analysis revealed both as independent prognosticators of salvage status.
Conclusion:
Recurrence after surgical varicocelectomy is associated with increased inguinal collaterals. The pitfall presented by this anatomic variant to surgical ligation may be successfully managed with selective gonadal vein embolization.
Introduction
Angiography with angioembolization of the affected gonadal vein and associated collateral branches has been reported as a successful means of both primary and salvage treatment for symptomatic varicoceles. 2,3 Percutaneous embolization offers a cost-effective, outpatient option with minimal complications and miniscule risk for postoperative hydrocele formation compared with surgical treatment modalities. 4,5 Furthermore, embolization has been shown to improve semen parameters in subfertile men with varicoceles, in some cases necessitating less invasive forms of artificial reproductive technologies to achieve paternity. 6,7
Persistent or recurrent venous reflux after varicocele repair has been previously attributed to incomplete occlusion of branches of the gonadal vein or various collateral vessels of the retroperitoneum or inguinal region. 3,8,9 We aim to investigate the angiographic findings at the time of embolization to better define the venous anatomy of primary varicoceles vs those with previous failed surgical varicocelectomy to define the cause of persistence or recurrence.
Patients and Methods
A retrospective review was performed of 106 patients who were referred to our interventional radiology department for either primary or salvage varicocelectomy between 1992 and 2010. Institutional Review Board approval was obtained for this study. Patient demographics, history of previous varicocele repair, physical examination and grading of the scrotal varicocele(s), indication for treatment, and periprocedural parameters were recorded in a patient deidentified database. In addition, findings of all available preprocedural physical and ultrasonographic examinations were documented.
All patients underwent transfemoral venography to confirm reflux into the gonadal vein and define the venous anatomy. After the initial venogram, gonadal shielding was performed to limit radiation exposure to the gonads throughout the remainder of the procedure. Subsequently, varicocele embolization was performed using a combination of embolization coils of varying sizes and Amplatzer® vascular plug devices (AGA Medical Corporation, Plymouth, MN). At the culmination of the embolization procedure, venography was performed to ensure cessation of reflux into the scrotal varicocele. All procedures were performed using local anesthetic administered at the site of vascular access and intravenous sedation; all patients were discharged the same day after a period of recovery.
All radiographic images obtained were reviewed by an interventional radiologist, specifically delineating the venous anatomy including collateral branching flow that could serve as etiology of the varicocele. Data from original radiology reports and secondary review of the images were collected with specific attention to the patency of the gonadal vein, number of gonadal vein divisions present, and the presence of any retroperitoneal and inguinal collateral vessels.
Primary and salvage embolization cohorts were compared using t test and chi-square analyses for continuous and categorical variables, respectively. A predetermined P value threshold of 0.05 was used to define statistical significance. Univariate and multivariable linear regression models were performed to assess the posthoc predictive nature of any angiographic findings in classifying varicocele embolizations performed as either primary vs salvage procedures. All statistical analyses were performed using Microsoft® Excel 2003 and SPSS® for Windows® version 16.0.
Results
Between 1992 and 2010, 106 patients underwent selective gonadal vein angiography and retrograde embolization by interventional radiologists at our institution. These 106 patients consisted of 46 primary and 60 salvage varicocele embolizations that were performed on 57 and 62 testicular units, respectively. Patient demographics and varicocele grade are shown in Table 1. The salvage varicocele embolization cohort of patients was significantly younger (P<0.001) and comprised a higher proportion of solely left-sided pathology compared with the primary treatment cohort that had 24% presenting for bilateral varicocele embolization (P=0.002). No patients in either cohort presented for retrograde embolization of an isolated right-sided varicocele.
There was no significant difference in varicocele grade when primary vs recurrent varicocele cohorts were compared. Subset analysis by side was not feasible because of the limited number of patients presenting for salvage treatment of bilateral varicoceles. Combining both treatment cohorts, however, there was a notable difference in varicocele grade favoring more significant varicocele dilation in left-sided pathology (P<0.001).
Analysis of angiographic findings are demonstrated in Table 1. The data revealed an equivalent number of gonadal vein divisions (Figs. 1A, B) comparing the primary and salvage cohorts in addition to a statistically equivalent proportion of patent or reconstituted gonadal veins (Figs. 1C, D). Similarly, the proportion of isolated retroperitoneal collaterals was comparable (Figs. 2A, B). The proportion of inguinal collateral veins identified (Fig. 2C) in the cohort undergoing salvage embolization after failed surgical varicocelectomy (27.8%), however, was a significantly higher than those undergoing primary varicocele embolization (6.7%), P=0.007. Furthermore, the combined presence of both retroperitoneal and inguinal collateral veins (Figs. 2D, E) was more commonly found in salvage varicocele cases (P=0.044) (Table 1).
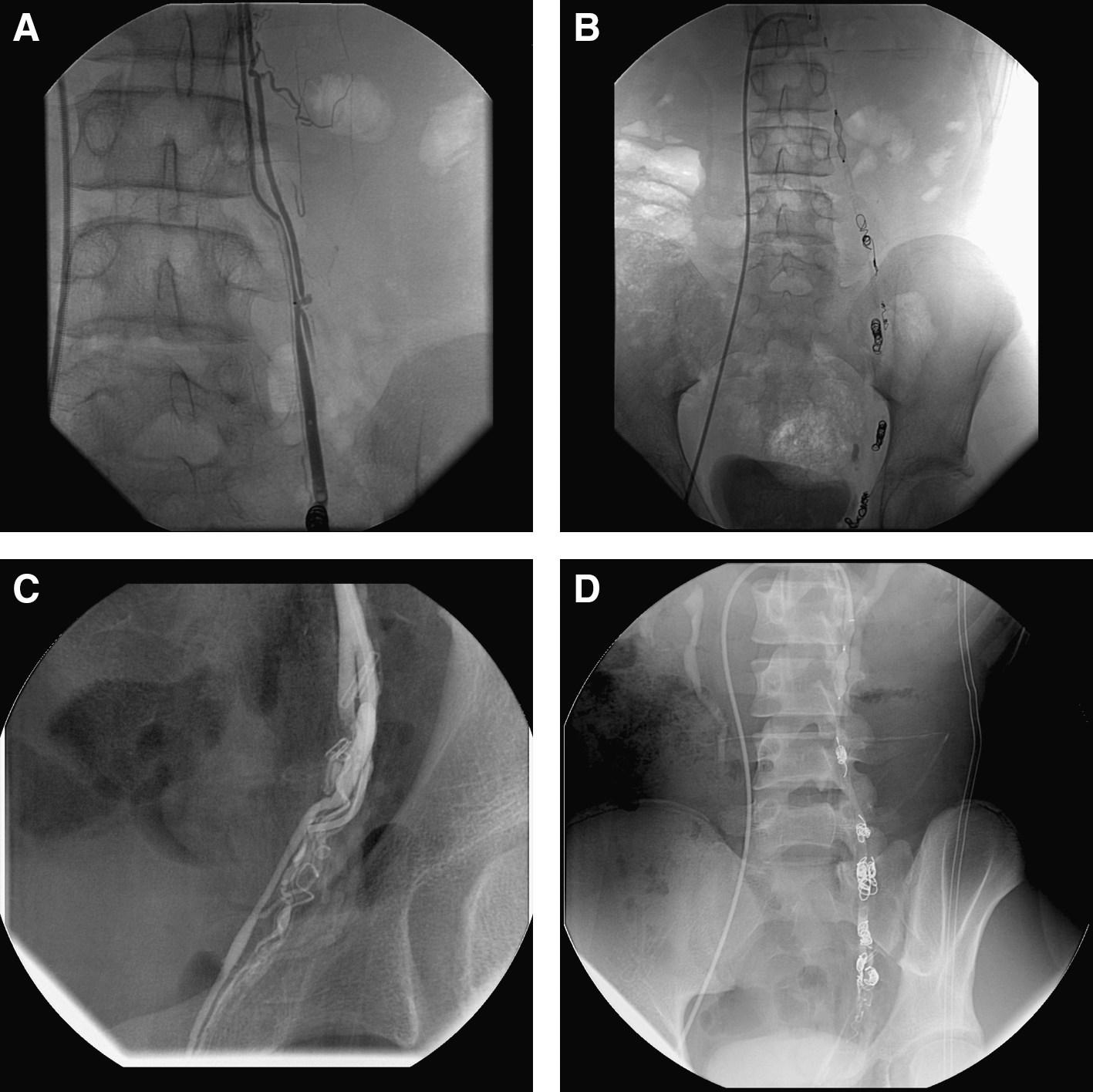
Gonadal vein angiogram demonstrates
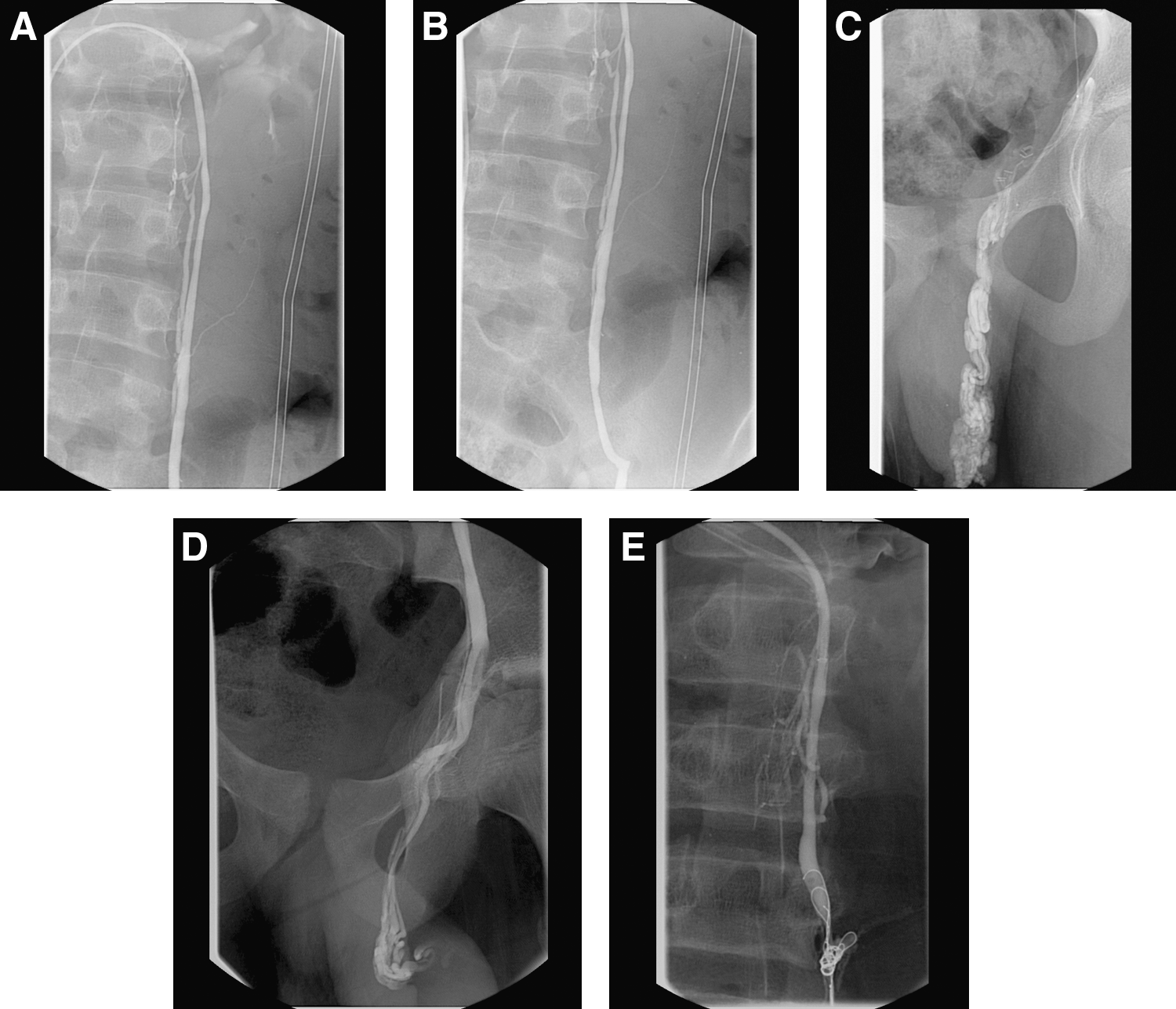
Venogram demonstrates
Analysis of the angiographic parameters as posthoc predictive criteria was performed using univariate and multivariable linear regression models, which demonstrated isolated inguinal collateral vasculature to be an independent criterion predictive of the treatment cohort the patient belonged to (P=0.008). The presence of both inguinal and retroperitoneal collaterals was also an independent prognosticator of salvage status (P=0.038). Other parameters investigated in the model were not significant on univariate or multivariable models (Table 2).
Discussion
Treatment of symptomatic varicoceles either for subfertility, significant testicular asymmetry, pain, or swelling has been controversial, given the wide array of available treatment options. Surgical ligation methods include subinguinal micro- or macroscopic, inguinal macroscopic (Ivanissevich), and the open or laparoscopic retroperitoneal (Palomo) approaches. Each surgical ligation technique has varying reported rates of treatment failure, resulting in either persistence or recurrence of the scrotal varicocele on the treated side. 10 –13 In addition, a percentage of patients undergoing each ligation approach are at risk for hydrocele formation, of whom some become symptomatic and need a secondary operation to address the hydrocele.
Although the literature supports “catch-up” testicular growth, improved semen analysis parameters, and increased Leydig cell function after each treatment approach, there are limited data that varicocele ligation significantly improves pregnancy rates. 14,15 Nevertheless, there is no consensus as to the best method of surgical ligation for the treatment of varicoceles. By using a wide variety of embolization techniques, retrograde gonadal vein angioembolization has been performed for more than three decades and now serves as a viable minimally invasive option for the management of both primary and recurrent varicoceles.
Patients who present to an interventional radiologist for varicocele embolization are commonly referred by urologists for consultation, which inherently subjects this patient population to a selection bias. Urologists counseling patients to consider embolization and referring to their interventional radiology colleagues depends solely on the practice protocol, either preferring embolization over surgical ligation for the treatment of primary varicoceles or more commonly referring for embolization in cases of persistence or recurrence after surgical treatment. This practice-based referral pattern may explain the age differential found comparing our two patient cohorts whereby patients in the salvage treatment group were significantly younger, whereas many of the primary varicoceles were directly referred for embolization by general urologists whose practice did not specialize in male infertility. Similarly, the disparate proportion of solely left-sided pathology in the salvage treatment cohort is confounded by the younger age of that patient population. The majority of patients in the pediatric and adolescent population who undergo surgical treatment of varicoceles do so for testicular asymmetry, more commonly treating unilateral left-sided pathology. 16
Our investigation focused primarily on the differential venous anatomy as demonstrated on selective gonadal vein angiography during the treatment of primary compared with salvage varicoceles after various forms of surgical ligation. A better understanding of the venous anatomy and pathophysiology in both primary and recurrent varicocele populations would allow for improved patient counseling and clinical decision-making among the plethora of treatment options available.
A previous report by Feneley and colleagues 3 demonstrated the cause of persistence or recurrence of a varicocele after surgical ligation was incomplete obliteration of collateral vessels as found on angiography. In their series, a subset of 18 patients presented for attempted salvage varicocele embolizations, of whom 14 were successfully treated. Of those receiving embolization, five had free flowing reflux through the gonadal vein despite previous surgical ligation, suggesting gonadal vein divisions that were not addressed by their report. Three of the four patients in whom attempted a salvage varicocele procedure was attempted had complex venous collateralization as the reason for recurrence, preventing successful embolization.
A study specifically investigating postsurgical varicocele recurrences with venography has been performed by Punekar and associates. 17 They evaluated a homogenous surgical population of men who had all undergone an inguinal (Ivanissevich) varicocele ligation with subsequent recurrences treated by venography and coil embolization. Description of angiographic findings in their population of 33 patients revealed 82% with parallel collateral channels as a cause of recurrence. Similarly, Sze and coworkers 9 demonstrated that the majority of salvage varicocele angiography and embolizations performed by their group were explained by gonadal vein branchings and parallel drainage mechanisms.
In the current investigation, we identify and classify the venous collateralization as possible routes of outflow and reflux for both cohorts of primary and salvage varicoceles. Although the number of gonadal vein divisions was equal in both treatment cohorts, it was surprising to find a nearly equal proportion of patent gonadal veins despite previous surgical ligation. This suggests reconstitution of the gonadal vein or one of its divisions with retroperitoneal or inguinal level collateral veins.
Interestingly, the proportion of patients with retroperitoneal or inguinal collateral veins was higher in the salvage varicocele patient cohort. Only the presence of isolated inguinal collateral veins, however, was statistically significantly increased in that group. The combination of both retroperitoneal and inguinal collateral veins was also significantly increased in the salvage varicocele cases. This was further supported by the multivariable regression model, which demonstrated that the presence of inguinal collaterals as well as the combined presence of inguinal and retroperitoneal collaterals are each independently predictive of the recurrent nature of the varicocele being investigated. These findings support that inguinal and possibly retroperitoneal venous collaterals are the cause of surgical treatment failures based on this comparison with primary varicoceles where no treatment had yet been used.
The presence of collaterals in patients with primary varicoceles demonstrates that these collaterals are a true anatomic variant that may serve as an occult pitfall to surgical ligation as the primary treatment for symptomatic varicoceles. Nabi and colleagues 7 identified 26.7% of patients undergoing retrograde varicocele angioembolization as having anomalous venous collaterals. The patient population in their study was not specifically noted to include salvage varicocele embolizations. This would be analogous to our patient population of primary varicocele angioembolizations, where 40.8% of patients in that treatment cohort had either retroperitoneal collaterals, inguinal collaterals, or both.
The salvage varicocele embolization cohort in the current study is not adequately powered to substratify by primary surgical approach used. Possibly a multi-institutional effort could better delineate the postoperative anatomic variability, if present, classified by the level of gonadal vein ligation performed. Other limitations of our study include the retrospective nature and the aforementioned selection bias present by the different referral patterns in the urology groups in our clinical practice region. Currently, the efficacy and cost-effectiveness of retrograde selective gonadal vein embolization for treatment of primary varicoceles is suggested by retrospective and a few small prospective studies. A larger randomized study with follow-up is necessary to ultimately determine the durability of angioembolization as a primary treatment option in overcoming the described venous anatomic pitfalls rendering surgery inadequate in some patients.
Conclusion
The angiographic findings at the time of retrograde varicocele embolization reveal salvage varicocele cases to be associated with an increased presence of inguinal venous collaterals, possibly the cause of varicocele persistence or recurrence after surgical ligation. This anatomic variability may be successfully managed with selective retrograde gonadal vein angioembolization.
Footnotes
Disclosure Statement
No competing financial interests exist.