
Abstract
Purpose:
To evaluate the effectiveness of NTrap in the prevention of stone migration during ureteroscopic lithotripsy for proximal ureteral stones.
Methods:
Eligible studies were identified from electronic databases (PubMed, Embase, the Cochrane Library, ISI - Science Citation Index, and Chinese biomedicine literature database). The database search, quality assessment, and data extraction were independently performed by two reviewers. Our primary outcomes were the stone-free (SF) and incidence of stone migration. Secondary outcomes were operative time and the rate of auxiliary procedures. The outcomes were explored by using Review Manager 5.0. Sensitivity analysis was performed to explore the influence of low-quality studies.
Results:
Two randomized controlled trials and one case-control study including 456 patients met the inclusion criteria. Meta-analysis of extractable data showed that patients who underwent ureteroscopic lithotripsy with the use of the NTrap demonstrated a significant advantage over without the use of the NTrap in terms of the stone-free rate (odds ratio [OR]=3.08, 95% confidence interval [CI] [1.45–6.53], P=0.003); the incidence of stone migration was significantly lower in NTrap treatment than without NTrap (OR=0.23, 95% CI: 0.10–0.53, P=0.0006, while there was no significant difference in operative time between NTrap and control (mean difference=−3.25, 95% CI: −16.11–9.62, P=0.62). Our pooled meta-analysis showed that the incidence of auxiliary shockwave lithotripsy was significantly lower in NTrap treatment than control (OR=0.29, 95% CI: 0.12–0.70, P=0.006).
Conclusion:
The results of this meta-analysis suggested that the NTrap stone occlusion device is efficient at preventing stone retropulsion during ureteroscopic lithotripsy of proximal ureteral calculi. The findings of this review highlight the need for more efficient performance of higher quality, more rigorous, large sample, long-term randomized controlled trials where outcomes are detailed in description.
Introduction
Various devices have been developed to prevent proximal migration of stones during lithotripsy. Most of these devices, however, have some limitations, with only marginal success in achieving this goal. 7 –9 Currently, the most successfully reported occlusion devices are the Stone Cone™ and NTrap.® 10,11 The NTrap device has a 3F shaft consisting of a wire mesh net composed of tightly woven nitinol wires within a 145-cm sheath. The net has central wires <1 mm apart and outer wires <2 mm apart. Advancing the wire mesh net beyond the tip of the carrying sheath deploys the net. The capacity of the net to occlude a maximal ureteral diameter is 7 mm. 12
Several randomized controlled trials (RCTs) and case-control study (CCS) have compared the efficacy and safety of NTrap devices in preventing proximal migration of stones and fragment extraction during ureteroscopic lithotripsy for proximal ureteral calculi, 12 –14 but to date there has been no systematic review and meta-analysis to evaluate the effectiveness of NTrap devices.
Methods
Literature searches were performed to identify RCT or CCS of NTrap in the prevention of stone migration during ureteroscopic lithotripsy for proximal ureteral stones. The following databases were used: Pub–ed (1966–July 2011), Embase (1974–July 2011), the Cochrane Library (2011 issue 5), ISI - Science Citation Index(1955-July 2011), and Chinese biomedicine literature database (1978–July 2011) using the following search terms: NTrap and ureteral stones, ureteroscopic lithotripsy to identify all relevant RCTs and CCS on the subject. We also used search engines such as Google™ to search related references on the Internet and searched the references of included studies to identify additional potentially relevant studies. The search were not restricted by publication year or language.
The search strategy described was used to obtain titles and abstracts of RCTs that were relevant to this review. The titles and abstracts were screened independently by two reviewers, who discarded studies that were not applicable, and two reviewers independently assessed retrieved the titles and abstracts of all identified trials to confirm fulfillment of inclusion criteria. Disagreements were resolved in consultation with Wang Zhiping. Data extraction was performed independently by the same authors using standard data extraction forms. For trials with multiple publications, we only included the most complete report for each outcome.
Our primary outcomes were the stone-free rate (SFR) and incidence of stone migration. Secondary outcomes were operative time and the rate of auxiliary procedures. The relevant data were extracted by two reviewers. The quality of RCT studies was assessed by the Cochrane Collaboration's tool, 15 which included assessment of sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting of outcomes, and other possible sources of bias. The non-RCT studies were assessed with a modification of the Newcastle-Ottawa Scale. 16 Scores 5 to 9 were defined as high quality, and a score <5 as low quality.
We analyzed the data using Review Manager (version 5.0) and extracted and pooled data for summary estimates. For meta-analysis, we combined data on dichotomous outcomes using the Mantel-Haenszel odds ratio (OR). For continuous outcomes, we used the inverse variance mean difference (MD) method and 95% confidence intervals (95%CI). We used the chi-square statistic and I2 test to assess heterogeneity between trials and the I2 statistic to assess the extent of inconsistency. I2 values of 25%, 50%, and 75% correspond to low, medium, and high levels of heterogeneity. When I2 values were less than 50%, we performed meta-analysis by fixed-effect model. When data are available and sufficient, subgroup analysis was performed by grouping the trials on RCT group and CCS group to explore possible heterogeneity. Sensitivity analysis was performed to explore the influence of low-quality studies.
Results
Nineteen studies were identified from the electronic database and hand search. After study assessment, we identified three trials 12 –14 — two RCTs and one CCS—that met our inclusion criteria (Table 1).
I/C=intervention/control; RCT=randomized controlled trial; CCS=case-control study.
There were 456 patients involved in the three trials: 199 receiving ureteroscopic lithotripsy with NTrap treatment and 192 only receiving ureteroscopic lithotripsy treatment. Table 1 showed the study characteristics of the three studies included in the meta-analysis. Baseline information was comparable between intervention groups and control groups. Quality assessment showed that two RCTs were deemed as moderate quality and one CCS was low quality.
Meta-analysis results
The rate of stone free
Three available studies' data including 374 patients reported the rate of stone free for NTrap vs control. At the follow-up end points, patients who underwent ureteroscopic lithotripsy with the use of the NTrap demonstrated a significant advantage over without the use of the NTrap in terms of the SFR (OR=3.08, 95% CI [1.45–6.53], P=0.003). After deleting the data of CCS, sensitivity analysis demonstrated that there was still statistical significance between NTrap and control (OR=−2.46, 95%CI: 1.08–5.60, P=0.03). The result of the SFR is depicted in Figure 1.
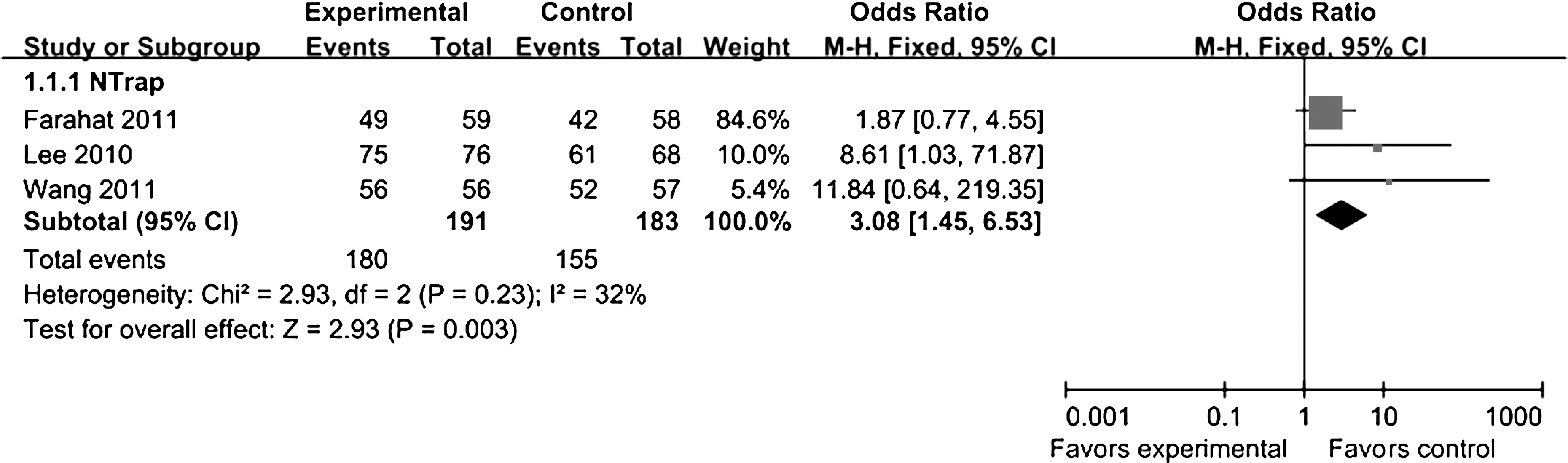
Pooled results of the incidence of stone-free rate between NTrap and without NTrap. CI=confidence interval.
The incidence of stone migration
Three available studies' data including 374 patients reported the incidence of stone migration for NTrap vs control. The results of pooled meta-analysis showed that the incidence of stone migration was significantly lower in NTrap treatment than control (OR=0.23, 95% CI: 0.10–0.53, P=0.0006) (Fig. 2). After deleting the data of CCS, sensitivity analysis demonstrated that there was still statistical significance between NTrap and control (OR=0.29, 95% CI: 0.12–0.71, P=0.007).
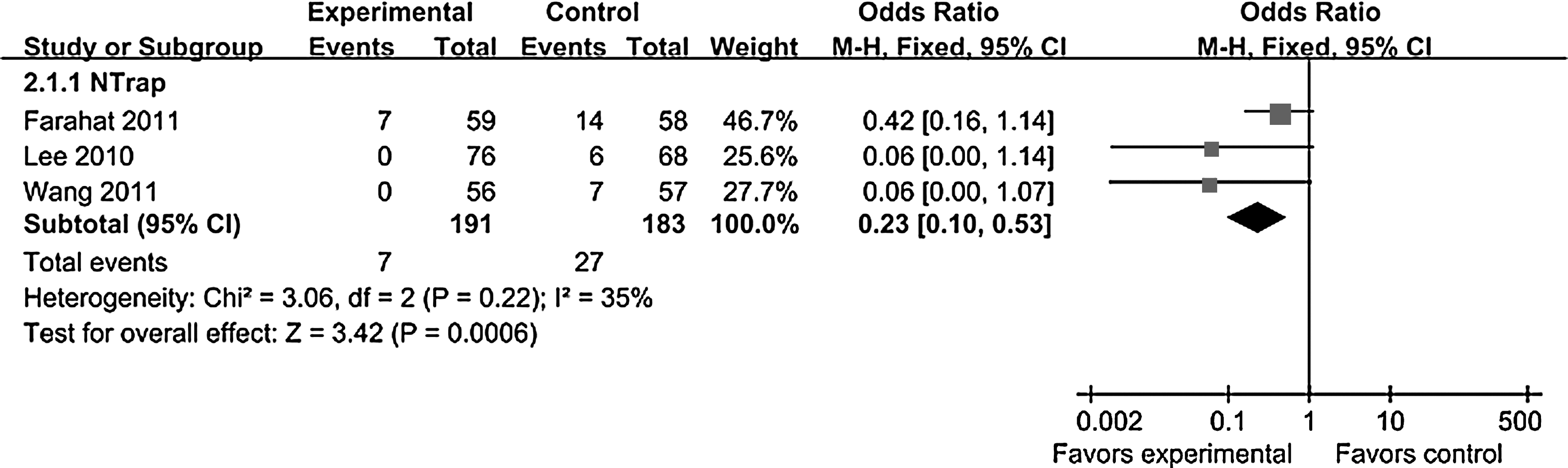
Pooled results of the incidence of stone migration between NTrap and without NTrap.
Operative time
Three available studies' data including 374 patients reported the operative time for NTrap vs control. Heterogeneity were observed in pooled analysis (P<0.00001, I2=98%). We performed meta-analysis by the random-effect model. The results of pooled meta-analysis showed that there was no significant difference between NTrap and control (MD=−3.25, 95% CI: −16.11–9.62, P=0.62) (Fig. 3). After deleting the data of CCS, sensitivity analysis demonstrated that there was still no statistical significance between NTrap and control (MD=−2.75, 95% CI: −21.24–15.75, P=0.77).

Pooled results of the operative time between NTrap and without NTrap.
Auxiliary procedures
Three available studies' data including 374 patients reported the incidence of auxiliary shock wave lithotripsy (SWL) for NTrap vs control. The results of pooled meta-analysis showed that the incidence of auxiliary SWL was significantly lower in NTrap treatment than control (OR=0.29, 95% CI: 0.12–0.70, P=0.006) (Fig. 4). After deleting the data of CCS, sensitivity analysis demonstrated that there were still statistical significance between NTrap and control (OR=0.33, 95% CI: 0.12–0.88, P=0.03).

Pooled results of the auxiliary shockwave lithotripsy between NTrap and without NTrap.
Discussion
To our knowledge, this study is the first systematic review with meta-analysis including RCT and CCS that compares NTrap with not NTrap during ureteroscopic lithotripsy for proximal ureteral stones. In our systematic review and meta-analysis, we had a precise search strategy, executed it with a librarian, and strengthened our meta-analysis with sensitivity analysis. By doing so, we expected to include all of the studies related to prevention of stone migration during ureteroscopic lithotripsy for proximal ureteral stones in a comparison between NTrap and without NTrap, hoping to reduce the confounding, limit the bias, and draw a scientific and statistically robust conclusion. A major concern with the current topic, however, is that only two RCTs were obtained. RCTs are considered the gold standard trial design for evaluating and comparing intervention by reducing bias to a minimum. To expand the number of included trials, we included the other case-control study. 14
The American Urological Association/European Association of Urology published the 2007 guidelines and recommended that for stones >10 mm, ureteroscopic management yields significantly greater SFRs for the majority of stone stratifications. 17 Some limitations remain, however, when using the lithotripsy device during ureteroscopic stone fragmentation. These include incomplete fragmentation, lack of stone retrieval, and possible proximal migration of the stones and stone fragments. The reported migration rate varies from 2% to 60%. 18 –20 Knispel and colleagues 21 reported 40% ureteral calculus migration from the proximal ureter and 5% from the distal ureter. Robert and associates 22 reported 48% calculus migration from the proximal ureter when pneumatic intracorporeal lithotripsy was performed. Recently, Chow and coworkers 23 noted that despite the use of modern techniques, such as laser lithotripsy and flexible ureteroscopy, a 25% failure rate was associated with ureteroscopy for proximal ureteral calculi.
Several strategies and devices have been recommended specifically to prevent retrograde stone migration and assist with fragment extraction. Currently, NTrap is one of the most successfully reported occlusion devices. Our pooled analysis and sensitivity analysis showed that the SFR was significantly higher (94.2% vs 84.5%) and the incidence of stone migration was significantly lower in NTrap treatment than without NTrap (3.7% vs 14.8%). Migrating stones and residual fragments usually need additional procedures that involve SWL. Our pooled meta-analysis results showed that the incidence of auxiliary SWL was also significantly lower in NTrap treatment than without NTrap (3.7% vs 11.5%).
Wang and associates 13 reported that the operative time of the NTrap group was significantly longer than that in the without NTrap group, while Farahat and coworkers 12 reported that operative time was significantly shorter in the NTrap group than in the without NTrap group. Moreover, Lee and colleagues 14 also indicated that operative time was shorter in the NTrap group than in the without NTrap group, although there was no significant difference. In our study, both the meta-analysis of RCTs and RCTs combined with case-control study showed that there was no statistical significance between the NTrap and without NTrap group, which may be related to surgeons with different operating proficiency.
Only one RCT reported Stone Cone 12 and BackStop 24 in the prevention of stone migration during ureteroscopic lithotripsy for proximal ureteral stones, respectively, so we could not use meta-analysis to evaluate the effectiveness of Stone Cone and BackStop. In the future, more Stone Cone and BackStop RCTs are needed to confirm effectiveness in the prevention of stone migration during ureteroscopic lithotripsy for proximal ureteral stones.
Han and colleagues 25 reported that the NTrap can save time and cost by lowering the rate of stone retropulsion, which involves unnecessary procedures such as prolonged operative times, rigid-flexible ureteroscope alteration, and additional operations. Economic efficiency also indicated that it was feasible to choose the NTrap in patients with proximal ureteral stones.
Our meta-analysis has several limitations. The number of included studies is relatively small. Only two RCTs reported the oucome of NTrap in prevention of stone migration during ureteroscopic lithotripsy for proximal ureteral stones. The small number of participants and included studies, as well as the moderate or low quality of most studies in this study, might not allow for a reliable conclusion. Second, we only included the data of published studies, and unpublished reports tend to show less positive results, 26 so the exclusion of these abstracts might have introduced bias in favor of the interventions. Because of the small sample and limited methodologic quality of the included studies, more efficient performance of higher quality, more rigorous, large sample, long-term randomized controlled trials in which outcomes are detailed in description are needed to confirm the above results.
Conclusion
The results of this meta-analysis suggested that the NTrap stone occlusion device is efficient at preventing stone retropulsion during ureteroscopic lithotripsy of proximal ureteral calculi. The findings of this review highlight the need for more efficient performance of higher quality, more rigorous, large sample, long-term randomized controlled trials where outcomes are detailed in description.
Footnotes
Disclosure Statement
No competing financial interests exist.