
Abstract
Background and Purpose:
Although conservative management is indicated in most cases of primary obstructed megaureter (POM), surgery is still indicated when POM is associated with increasing dilation, symptoms, or progressive renal damage. Surgery is associated with a significant rate of complications, however, especially in the case of very large ureter in the first year of life. A valid alternative could be endoscopic high pressure balloon dilation (EHPBD) of the vesicoureteral junction (VUJ). We report the first experience with EHPBD in patients under 1 year of age who were affected by severe POM.
Patients and Methods:
Five patients, aged between 6 and 12 months, were treated with EHPBD. In all patients, preoperative renal ultrasonography showed a distal ureteral dilation ≥15 mm that increased at later evaluations; an obstructive pattern was detected by preoperative diuretic renography. An 8-9,8 F cystoscope, and a 3F balloon catheter (balloon maximum diameter 4 mm) was used. The VUJ was dilated for 5 minutes at 12 to 14 atm. A 4.7F Double-J stent was then positioned and left in place for 6 to 8 weeks. Ultrasonography was performed every 3 months, and renography and voiding cystourethrography the fourth month after the EHPBD.
Results:
No operative complications were observed. All the patients showed an improvement at the ultrasonography postoperative follow-up, and there was no evidence of obstruction/reflux at the postoperative check up.
Conclusions:
Our preliminary results seem to indicate that EHPBD is a feasible, safe, and successful procedure. It could play a role as a minimally invasive alternative to open surgery in cases of POM that necessitate intervention in the first year of life. Longer follow-up is necessary to verify the stability of these results.
Introduction
Primary obstructive megaureter (POM) is from an intrinsic congenital obstruction of the prevesical portion of the ureter. In the majority of cases, there is not really an anatomic narrowing of the vesicoureteral junction (VUJ), but only a functional obstruction, from an aperistaltic segment of the distal end of the ureter.
The management of POM in children below the age of 1 year remains controversial. Conservative management is usually needed for the majority of megaureters. 4 –6 When POM is associated with increasing dilatation, symptoms, or progressive renal damage, however, there is an indication for operative treatment, even in the first year of life. 7,8
Currently, the most common surgical procedure to manage megaureter is the resection of the distal end of the ureter and ureteroneocystostomy, with or without tapering, depending on the diameter of the distal ureter.
Because the reimplantation of a grossly dilated ureter into the small bladder could be technically difficult and potentially dangerous for the normal functional development of the lower urinary tract, some authors have proposed a temporary ureteral derivation, in the first year of age, either external (cutaneous ureterostomy) 9,10 or internal, such as endoscopic or open insertion of a Double-J stent. 11 –14
Even in the less severe cases of POM that can be managed conservatively, the main criterion adopted to direct a patient to operative treatment is the reduction of renal function, but this unfavorable outcome is unpredictable and often irreversible. 8,15,16
Therefore, a minimally invasive alternative that could offer safe and efficient relief from the ureteral obstruction, such as balloon dilation, would be very attractive. In the pediatric age, only two studies have been reported about endoscopic balloon dilation of POM. 17,18
The aim of our study was to analyze the outcome of a selected group of children, under 1 year, with a POM necessitating intervention, treated by endoscopic high pressure balloon dilation (EHPBD) of the distal ureter.
Patients and Methods
Five patients (four boys and one girl), aged between 6 to 12 months (mean, 8 mos), who were affected by unilateral POM were treated from January 2009 to February 2010. All the cases were diagnosed prenatally as having hydronephrosis. Initial investigation involved a renal tract ultrasonographic scan during the first 2 weeks of life. Voiding cystourethrography (VCUG) and diuretic renography were performed between 4 and 8 weeks of life. Diuretic renography was performed according to a well-defined protocol (according to the guidelines of the Society of Nuclear Medicine 19 –21 ): The patients were hydrated orally 30 minutes before the scan, regions of interest (ROIs) were placed around each kidney for calculation of differential function, similar ROIs were placed around both kidney and ureter to calculate the time-activity curve of the diuresis; no evidence of urodynamic obstruction was defined as good drainage out of the ROIs 30 minutes after injection of technetium-99m–labeled mercaptoacetyl triglycine (MAG-3). If poor urinary drainage was seen, furosemide (1 mg/kg) was administered intravenously, and total urinary drainage out of the ROIs, during the 20 minutes after injection of furosemide, was calculated. A diuretic T/2 (the time at which the time-activity curve decreases to half its maximal activity) >20 minutes after furosemide injection was classified as obstruction pattern 20,21 ; moreover, the bladder was kept empty by a catheter during the renography.
The initial inclusion criteria for this study were dilatation of the distal ureter ≥15 mm at the first ultrasonography, age at diagnosis 1 to 6 months, and an obstructive pattern at the MAG-3 diuretic renography. All five patients showed a progressive increasing dilatation of the distal ureter at the successive ultrasonographies. The group represents about 10% of the primary obstructed megaureters seen in the same period, presenting with different characteristics. The progressive increasing ureteral dilatation, associated with an obstruction pattern at MAG-3 diuretic renography, was considered an indication for operative treatment, but instead of open surgery, the megaureter was managed by EHPBD.
EHPBD was performed under general anesthesia. Antibiotic prophylaxis was administered perioperatively. An 8-9,8 F cystoscope with a 5F working channel was used. A 0.032-inch guidewire was inserted, and the VUJ was dilated with a 3F balloon catheter for 5 minutes. The balloon length was 4 cm, and the balloon diameter was 4 mm when filled with contrast at 12 to 14 atm (Fig. 1).
Balloon catheter and inflation device; balloon inflated with contrast medium
In four (of five) cases, we could identify a definite stenotic ring, which disappeared at the end of the dilation. In one case, we could not see any ring, because the stenotic tract was longer. Retrograde urography was then performed to check the disappearance of the stenotic ring and to place a 4.7F Double-J stent. The Double-J placement was always difficult because of the kinking of the ureter. The stent was removed 6 to 8 weeks after the procedure, and antibiotic prophylaxis was maintained during this period.
Follow-up consisted of an ultrasonographic scan every 3 months (the first ultrasonography 1 month after Double-J stent removal) and MAG-3 renography with VCUG the fourth month after the EHPBD. Urinalysis was performed every month.
Results
There were no operative complications from the endoscopic procedure, and none of the five patients had urinary infection or any other postoperative problem. The patients were discharged within 24 hours of the procedure.
The mean follow-up was 23.8 months (range 16—30 mos). All patients showed an improvement on the ultrasonographic scan during the postoperative follow-up, and all the kidneys had a preserved function after the EHPBD (Table 1). No evidence of obstruction or vesicoureteral reflux in all the patients during the MAG-3 renography and VCUG performed at 4 months postoperatively was seen (Figs. 2, 3).
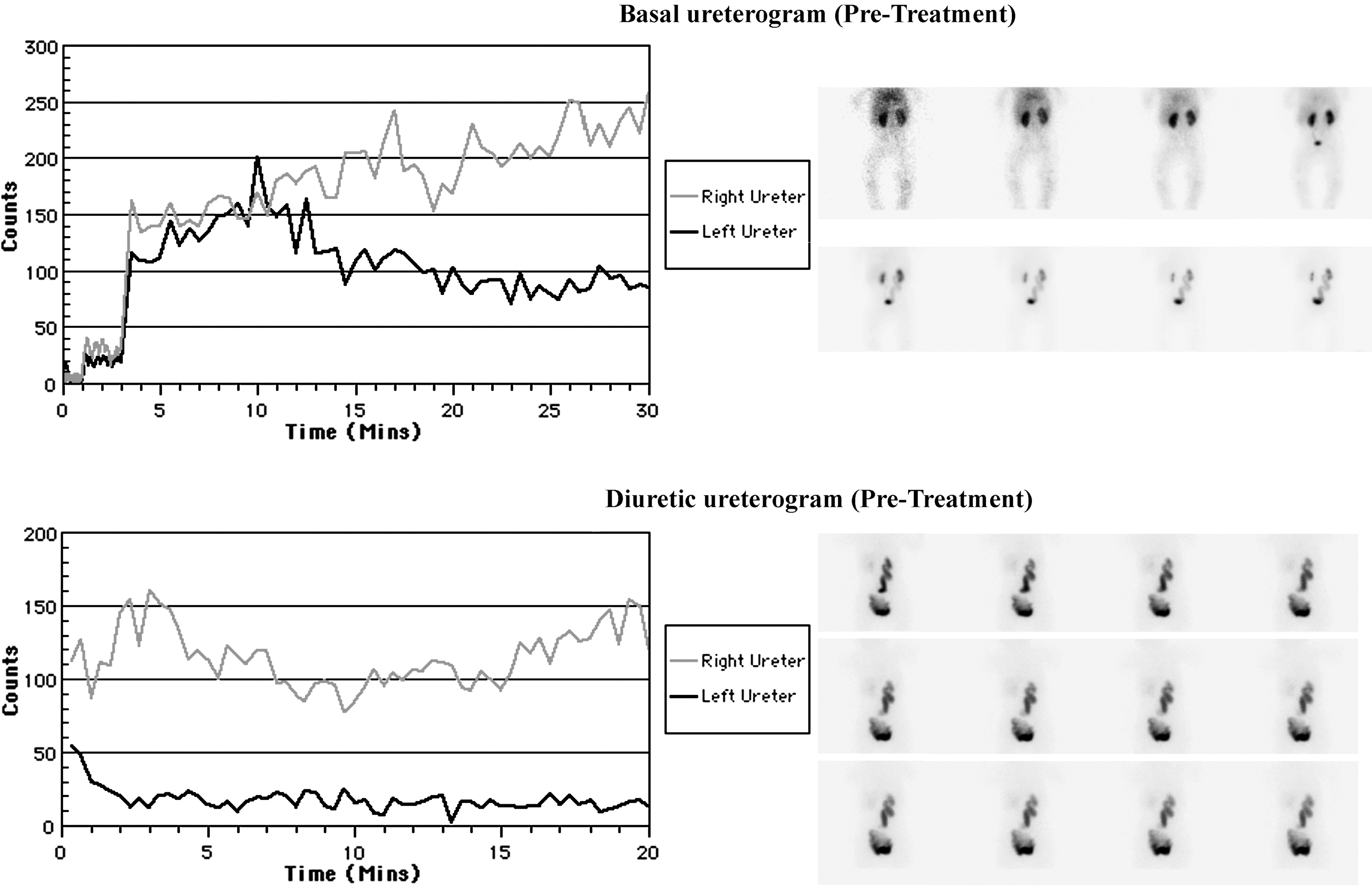
Mercaptoacetyl triglycine-3 renography shows an obstruction pattern of the right ureter before endoscopic high pressure balloon dilation.
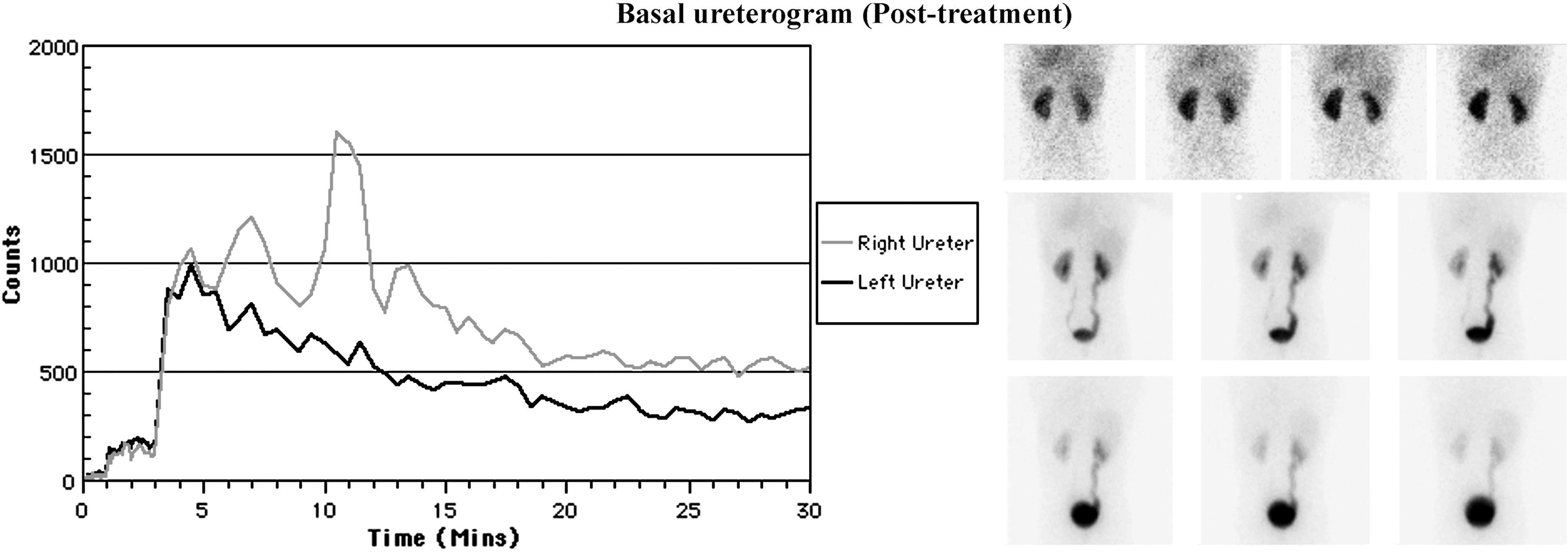
Mercaptoacetyl triglycine-3 renography indicates the absence of obstruction 4 months after endoscopic high pressure balloon dilation.
Obstruction=T/2>20 minutes after diuretic during renography; no obstruction=good urinary drainage out of the regions of interest at 30 minutes after injection of the MAG-3 without diuretic test).
VCUG=voiding cystourethrography; MAG-3=mercaptoacetyl triglycine-3; DUD=distal ureteral diameter.
Although the dilatation had not been completely resolved after the EHPBD, the very satisfactory result of the renography and ultrasonographies in the postoperative period indicated that the procedure was technically successful in all cases.
Discussion
The management of POM in children less than age 1 remains a subject of discussion.
In 1989 Peters and colleagues 7 reported that 89% of children with POM needed open surgery before 8 months of age. Although the overall results were good, the complication rate was rather high, with a reoperation rate of 12%. On the other hand, Keating and coworkers 4 reported good results in the same year with conservative management. Another argument against open surgery in the first year of life is the onset of bladder dysfunction at follow-up, reported by some authors. 22 –24 Moreover, several studies showed that a ureteral diameter >10 mm and slow drainage on renal scan were predictors of poor outcome, even though these findings do not absolutely indicate the need for surgery. 25
As a result of these studies, the trend in the management of POM has been in favor of a conservative approach, at least in the first year of life. When POM is associated with progressive increasing dilatation, symptoms, or progressive renal damage, however, there is a clear indication for operative treatment. 8,9,14,16
Because the reimplantation of a grossly dilated ureter into a small bladder (such as the bladder in the first year of life) is technically difficult as well as associated with a higher complication rate, some authors have proposed a temporary ureteral diversion, such as cutaneous ureterostomy, to preserve renal function and allow the reduction of the megaureter diameter, making ureteral tapering unnecessary at definitive surgery. 9,10
As an alternative to cutaneous ureterostomy, Ransley and associates 11 proposed the temporary insertion of a Double-J stent in the megaureter to bypass the obstruction. This procedure is sometimes difficult to perform endoscopically in a child (<1 year old); therefore, a small open cystostomy was performed in half of the cases. 12 The stent placement of POM is not a definitive treatment (half of POMs need surgery after stent removal), but it is valuable to temporize surgery after 1 year of age; moreover, this procedure is associated with a high rate (30% to 70%) of complications (infection, stent migration, stone formation, or knotting of the stent). 12,14 In our series, the balloon catheter was always inserted endoscopically. It is likely that our successful outcomes depended on the use of particular instruments. The small operative cystoscope (8-9, 8F) reduced the need for open insertion in patients with a small caliber urethra. Moreover, the use of a 3F semirigid balloon catheter allowed easier stent placement in the ureter.
A minimally invasive technique for the definitive treatment of POM would be a very attractive option. Both antegrade and retrograde ballon dilation have been reported as treatment for ureteral strictures 26,27 and primary ureteropelvic obstruction in adults. 28 In the pediatric age, few studies have been reported on balloon dilation of ureteropelvic junction obstruction. 29,30 Endoscopic dilation of obstructive megaureter was first described in children by Angulo and coworkers in 1998. 17 They treated a group of 11 patients with primary and secondary obstructive megaureter, aged 4 months to 11 years. In 2007, Angerri and colleagues 18 presented a study on their initial experience with endoscopic balloon dilation, specifically in seven children who were affected by POM.
In the literature, our report is the first to include patients only below 1 year of age who were affected by severe POM and treated with endoscopic balloon dilation. In our patients, there were clear indications for operative treatment, on the basis of increasing distal ureteral dilatation and an obstructive pattern at MAG-3 diuretic renography. Conservative management, with a potential risk of permanent renal damage, did not seem to be an acceptable approach. Open surgery in patients younger than 1 year, however, is associated with a higher rate of complications than in older children, even long after the procedure, such as the onset of bladder dysfunction. 22 –24
In four of our five cases, we observed a stenotic ring as the cause of obstruction, in agreement with the findings of Angerri and colleagues. 18 The evidence of a stenotic ring and its disappearance after endoscopic dilation is in contrast with the general view that the cause of POM is the aperistaltic distal ureter. Actually, the ring would appear to be very tough, because the filling pressure of the balloon needed to achieve its disappearance has to exceed 10 atm under endoscopic and fluoroscopic control. This finding cannot be explained by the current knowledge of the possible causes of POM, which are usually focused on segmental changes of muscle cells. 31 –33 At least in four cases of our series and in the seven cases of Angerri and asociates, 18 a real stenosis of the distal ureter seems to have been demonstrated.
Conclusions
In the management of POM in patients under 1 year of age, EHPBD seems to be feasible and, in the short/medium term, also safe and effective.
In cases of POM that necessitate intervention below the first year of life, EHPBD could be also a less invasive alternative to temporary cutaneous ureterostomy or later reimplantation. Moreover, the EHPBD appears to be more efficient and associated with less morbidity than simple stent placement with a Double-J catheter.
Longer follow-up is necessary to verify the stability of these results.
Footnotes
Acknowledgments
Many thanks to Prof. Kyriacos Kyriacou (MA), a native English speaker who teaches the English language at the Sapienza University of Rome. He performed the English review of this article.
Disclosure Statement
No competing financial interests exist.