
Abstract
Introduction and Objectives:
We report the results of a randomized controlled trial comparing three different lithotriptors using semirigid ureteroscopy (URS) for distal ureteral stones.
Methods:
Between September 2009 and November 2010 69 patients undergoing ureteroscopy were randomized to three groups: LithoClast classic (Group 1), Holmium Laser (Group 2), and StoneBreaker™ (Group 3). A 7.5F semirigid ureteroscope was used in all procedures. The primary outcome was differences in fragmentation time. Secondary outcomes were stone-free rates, intraoperative complications, stone-up migration, hospital stay, analgesic requirement, and need for auxiliary procedures. Patients were followed up at 15 days, 30 days, and 3 months. The stone-free status was defined with noncontrast computed tomography performed at first control. Univariate and multivariate analysis were performed to determine clinical and surgical factors that have direct impact on the success of ureteroscopy. Chi-square test and Analysis of Covariance (ANCOVA) tests were used for statistical comparisons.
Results:
There were no differences between sociodemographic variables. Average stone size was 7.17±2.04 mm in Group 1; 7.89±2.73 mm in Group 2; and 7.79±2.97 mm in Group 3 (p=0.79). Fragmentation time were similar between lithotriptors; 27.12±4.07 minutes in Lithoclast group; 21.78±2.81 minutes in Laser group, and 27.14±4.71 minutes in StoneBreaker group (p=0.74). Stone-free rates were 96%±11.18% (group 1), 96.9%±8% (group 2), and 96.9%±8.4% (group 3) (p=0.1). No difference was observed in stone-up migration, postoperative Double-J stent placement, or auxiliary procedures. Stone size and the placement of a second working wire were associated with shorter fragmentation time (p<0.01).
Conclusions:
The three lithotripsy devices evaluated behaved similarly in terms of the ability to fragment stones, and were equally effective for distal ureteral stones. Adequate fragmentation and fragment removal are mainly dependant on stone size and surgical technique (use of auxiliary wire).
Introduction
The aforementioned methods have some drawbacks in terms of cost, portability, necessity of external electrical power, or access to compressed air pipelines. Current studies in URS show certain degree of superiority of Ho:YAG laser compared with pneumatic lithotripsy in terms of stone clearance and complications in upper ureteric stones. 2,3 The ideal lithotriptor has still not been developed. Recently a novel device demonstrated its utility in management of ureteral calculi, 4,5 the LMA StoneBreaker™ (Cook, Medical) that works as a contact ballistic lithotriptor with a single pulse mode. This device is powered by a cartridge of high pressure carbon dioxide gas providing the necessary energy for stone fragmentation in a single procedure.
To our knowledge no comparison between three different types of lithotriptors has been published. We report a prospective, randomized trial comparing the results in terms of success rates and complications between Lithoclast classic, Ho:YAG laser, and StoneBreaker.
Materials and Methods
All patients older than 18 years who were admitted to the department of urology at Catholic University Hospital and who were scheduled for endoscopic extraction of a distal ureteral stone were considered for enrollment. Exclusion criteria were: abnormal anatomy, known ureteral stricture, presence of renal insufficiency, active kidney infection, and previous failed pneumatic lithotripsy. Upon recruitment each patient provided written informed consent.
Preoperative evaluation included clinical history, physical examination, urinalysis, and radiologic evaluation with noncontrast computed tomography (CT). All procedures were done by the attending urologist or urology resident under direct supervision. For this study patients with mild hydronephrosis only were considered.
Under general anesthesia URS was performed with a 7.5F semirigid ureteroscope (Richard Wolf, Knittligen, Germany). With the patient in the lithotomy position a 0.038 inch guidewire was coiled at the renal pelvis, a second guide was required in case of a difficult negotation of the ureteral orifice. A 350 μm fiber in the group of Ho:YAG Laser was used setting the energy at 0.8–1.5 joules and at frequency of 12 to 20 Hz. One millimeter probe was used in Swiss Lithoclast group using multiple fire technique. For StoneBreaker group a 1 mm probe was selected for the ureteroscopic lithotripsy. No additional devices were used to prevent retropulsion. Fragmentation concluded when stone fragments were sufficiently small to achieve an easy and safe removal.
Patients were followed up as outpatients at 15 days, 30 days, and 3 months The stone-free status was defined with noncontrast CT performed at first control (Postoperative day 15).
The primary outcome was differences in fragmentation time during the procedure. Secondary outcomes were stone-free rates, stone up migration, intraoperative complications (including damage to the mucosa, ureteral perforation, and prolonged hematuria), necessity of Double-J stent placement, differences in hospitalization, and need for pain analgesia. In case of direct visualization of retropulsion of fragments, a flexible URS was performed.
Statistical methods
This study was designed to detect a 5 minutes difference between each device, with a power at 0.9 and a type I error at 5%, and 13 patients were required for a group. We planned to enroll 23 patients per arm to prevent the potential loss of follow-up. Allocation into groups was done by random allotment of chits.
Analysis was done with SPSS® version 17. Proportions comparisons were done with chi-square test or Fisher test as appropiate. Univariate and multivariate analysis were performed to determine clinical and surgical factors that have direct impact on the success of URS.
Results
Between September 2009 and November 2010 89 patients met inclusion criteria for enrollment. Twenty patients did not require the fragmentation of the stone; consequently they were excluded for the analysis. Four patients were not available for follow-up. Finally, the analysis included 22 patients for Lithoclast group, 23 for Holmium Laser, and 20 for StoneBreaker group. (Fig. 1).
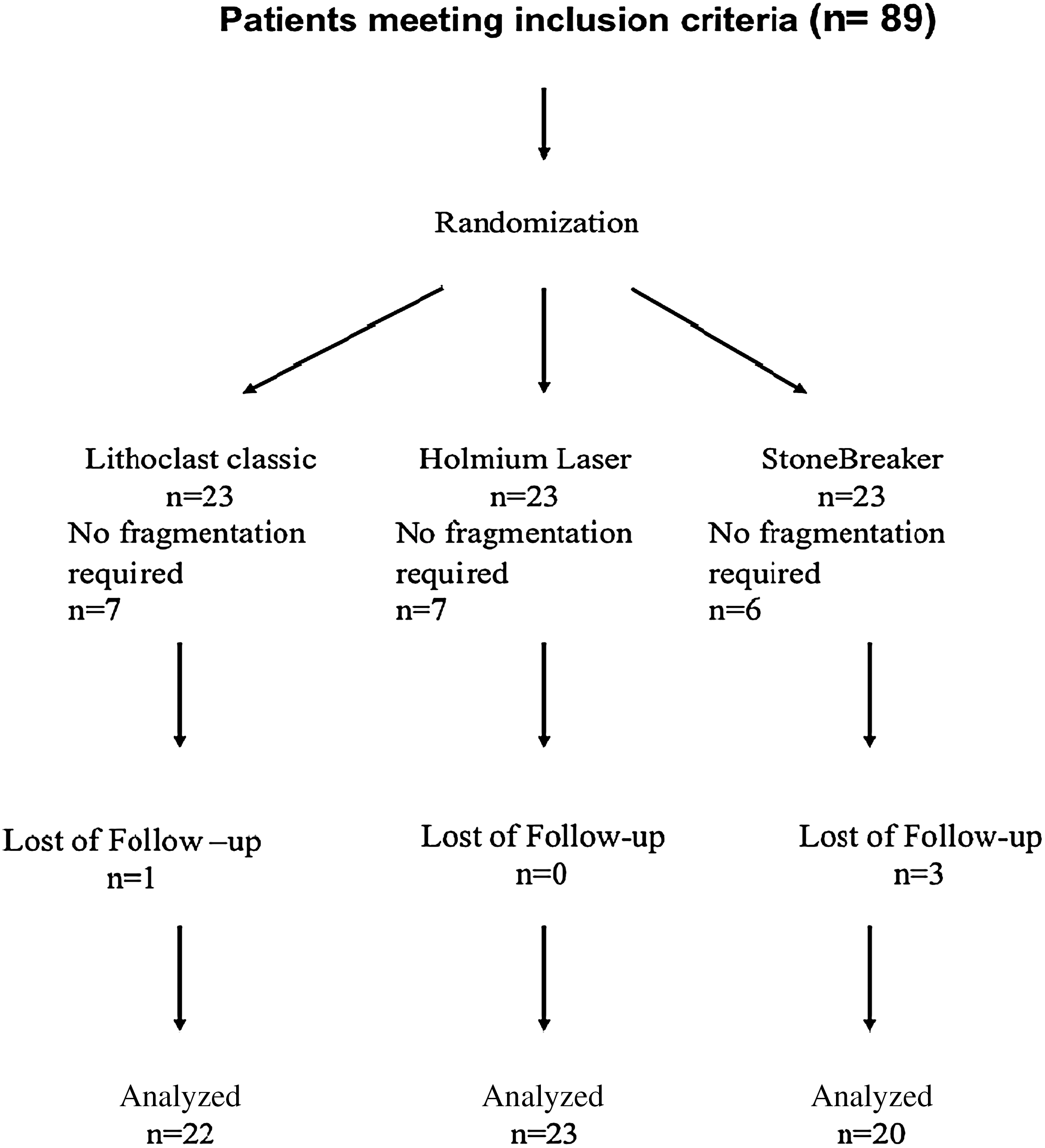
Patient flow during study.
Demographics parameters between each arm were not significantly different. Average stone size was comparable between groups. (Table 1).
Duration of symptoms were similar between groups, with 10 days for Lithoclast, 15 days for Holmium laser, and 15 days for StoneBreaker (p=0.79). In terms of technique 28 (40.6%) patient required the use of a second guidewire to secure the access.
A trend toward a higher number of complications in Lithoclast group was observed, including the unique case of ureteral perforation in this series, but there were no statistically significant differences among groups (p=0.47). Likewise, rate of fragment up migration and fragmentation time were similar between groups. (Table 2).
Only one patient by group required more than 24 hours hospital stay. Criteria for Double-J stent placement was determined by the surgeon, mainly when an important mucosal injury was evident at the end of the URS (p=0.3). All patients showed 100% stone-free rate at 3 months, as evidenced by noncontrast CT. Nonauxiliary procedures were required.
Finally, multivariate analysis shows only two factors related with increased fragmentation time, stone size (odds ratio [OR]: 2.09, confidence interval [CI] 95%: 1.47, 3.47) and the negotation of the ureteral orifice without the use of an auxiliary guide (OR: 20.39, CI 95%: 6.72, 34.07).
Discussion
Endoscopic lithotripsy has progressively become the gold standard in management of ureteral calculi. Several factors have influenced this trend. Gerber 6 published an electronic survey in 2010 demonstrating a possible explanation for this choice of treatment, particularly for patients with distal ureteral stones, to the wider availability of the Holmium laser, improvements in endoscopes, and a growing dissatisfaction with the overall results achieved with shock wave lithotripsy.
Between disintegration devices, the Ho:YAG laser has been defined as the gold standard for intracorporeal ureteral lithotripsy due to its capacity to fragment regardless of the hardness and size of the stone, achieving the smallest fragment compared with other intracorporeal lithotriptors. 7 Luminous energy released by the Holmium laser is transformed to thermal energy which results in photothermal chemical decomposition of the stone. 8 Holmium laser lithotripsy is also associated with a low incidence of proximal stone migration, however the cost of the Holmium laser assisted URS is higher than that for using pneumatic lithotripsy. Pneumatic lithotripsy provides excellent fragmentation rates with the advantage in terms of cost-effectiveness compared with Holmium laser, although migration of the stone toward the renal pelvis might be a limiting factor. The Swiss Lithoclast®, introduced in the early 1990s, was the first ballistic lithotrite. Clean, pressurized air acts as an energy source to fire the projectile onto a metal rod that is in contact with the stone, 9 achieving complete fragmentation of all stones irrespective of their composition 10 and no significant long-term tissue effects. 11 The StoneBreaker is a contact, pneumatic, and portable intracorporeal lithotriptor; a compressed carbon dioxide cartridge provides the energy for stone fragmentation. Rané et al 4 first reported their experience with this device in 42 cases of ureteral stone requiring a mean of nine shocks for fragmentation and subsequent successful clearance. In terms of safety, Nerli et al, 5 described no complications or evidence of tissue trauma in 110 patients with ureteral calculi fragmented with the StoneBreaker. In our study, the three lithotripsy devices achieved a similar stone clearance rate at the end of the procedure, 96% for Lithoclast group, 97% Holmium laser group, and 96.9% for StoneBreaker group (p=0.97), which is comparable to international published data. 3,4,5,10,12,13
Proximal stone-up migration accounts for significant endoscopic failures. Pneumatic lithotriptors has been traditionally associated to this complication because of its jack hammer mechanism. However, laser endoscopic lithotripsy is not free from this issue, as Lee and coworkers 14 reported in their model of retropulsion during Ho:YAG lithotripsy and determined that retropulsion increases as the laser energy and the fiber diameter increases. In fact, in our report the lower rate of fragment up migration was associated to Lithoclast group followed by Holmium laser group, although no statistical difference was found. This could be explained by selection, in our protocol, of patients with mild hydronephrosis, which could generate a bias in favor of pneumatic lithotriptors.
In terms of fragmentation time, Manohar et al 15 demonstrated comparable results between Swiss Lithoclast 2® and Ho:YAG laser in upper ureteral stones. The present study shows a trend toward shorter operatives times with Holmium laser compared with the other devices (p=0.74), but not enough to reach significant differences, although our protocol considered only distal stones. A similar comparison has been made in the setting of percutaneous nephrolithotomy, Zhu et al 13 reported a difference of only 4 minutes faster using Lithoclast compared to Holmium laser, which did not reach a statistically significant difference.
Potential complications in URS could be separated in two different aspects: Early and late complications. Geavlete and associates 16 found a rate of 10.64% for perioperative complications, most of them corresponded to mucosal abrasion. In the same article late complications were described only in 0.2% of cases, which included three cases of ureteral stenosis and two cases of persistent vesicoureteral reflux. In our experience perioperative complications reached 11.6% (5 cases): persistent hematuria (one case), lesion of the ureteral mucosa (three cases), and perforation (one case). The case of ureteral perforation was recognized at the end of the URS, this was viewed as a single hole, about 3 mm in diameter and with net margins. As described above, we decided to leave a Double-J stent, which was removed 1 month later. During the follow-up period of our report, no case of ureteral stenosis was discovered. Since StoneBreaker and Lithoclast are pneumatic lithotriptors, there is no risk of thermal injury in the ureteral mucosa. However potential ureteral damage can occur by pressure generated with pneumatic devices. In an animal study, pneumatic pressure generated by Lithoclast demonstrated minimal focal hemorrhage and edema occurring on tissue contact, but after acute injury, no extravasation was noted on retrograde pyeloureterography. 11
According to the multivariate analysis, the use of a second guide during the URS was associated to a faster procedure. We believe that this is related with a more successful advance of the endoscope which is related with a faster extraction of fragments.
Conclusion
The three lithotripsy devices evaluated at our institution behaved similarly in terms of the ability to fragment stones, and were equally effective for distal ureteral stones. Adequate fragmentation and fragment removal are mainly dependant on stone size and surgical technique (use of auxiliary wire). We believe that unique endourologic treatment modality for distal ureteral stones is not justified.
Footnotes
Disclosure Statement
No competing financial interest exists.