
Abstract
During cryotherapy of the prostate, identification of probe tips that are misplaced into the bladder is often not readily apparent via transrectal ultrasonography. Ultimately, cystoscopy is needed to ensure this has not occurred before initiating a freeze. We describe the innovative use of continuous flexible cystoscopy in retroflexion for visualization of the bladder neck during insertion and manipulation of cryoprobes. Using this technique, it is possible to identify probes errantly placed into the bladder lumen in real time, thereby facilitating safe and accurate placement and eliminating an unnecessary step in the cryotherapy procedure. Instead of placing a Foley catheter at the beginning of the cryotherapy procedure, a flexible cystoscope is advanced into the bladder lumen and retroflexed at the onset of the procedure. The cystoscope is maintained in this position during cryoprobe placement. This real-time observation of the bladder neck allows for immediate withdrawal and repositioning of cryoprobes inadvertently advanced into the bladder. This technique also obviates the need for Foley catheter placement at the beginning of the procedure and subsequent removal after cryoprobe insertion to allow for cystoscopic evaluation for inadvertent cryoprobe insertion into the bladder or urethral lumen.
Introduction
Despite these advances, care must still be taken to avoid probe placement into the urethra or bladder to avoid thermal injury to these areas and subsequent urethral sloughing or ureteral injury, respectively. The standard technique, as described by Cohen 1 and Onik 2 has been to distend the urinary bladder with sterile water via a Foley catheter and place all cryoprobes and thermocouples stereotactically using a placement grid with simultaneous transrectal ultrasonography. After all probes are in place, the Foley catheter is then removed, and flexible cystourethroscopy is used to confirm that no probes have penetrated the urethra or bladder neck. If probes are visualized in an improper position, they are then repositioned under cystoscopic guidance. With the use of an increasing numbers of probes, however, it can be difficult to determine which of the inserted probes is misplaced. Thus, manipulation and repositioning of multiple probes is often necessary in pursuit of the one that is malpositioned. In the interest of simplifying this process, we propose the use of continuous retroflexion video cystoscopy during the initial placement of all cryoprobes and thermocouples.
Technique
After induction of general anesthesia, the patient is placed in the dorsal lithotomy position and sterilely prepped and draped. A flexible video cystoscope is then advanced into the bladder, the bladder is distended with sterile water, and the cystoscope is retroflexed to provide a view of the bladder neck. The cystoscope is then laid down on the draped abdomen so as to remain passively retroflexed. A biplanar transrectal ultrasound probe is inserted into the rectum, and the prostate is visualized. A computerized cryoablation plotting system is used to calculate ideal cryoprobe placement, and probes and thermocouples are inserted transperineally via a placement grid. Position and depth of insertion are monitored simultaneously via transrectal ultrasonography and cystoscopy. If a probe is observed to pierce the bladder, it is immediately withdrawn and repositioned. Once all probes and thermocouples are properly positioned, a guidewire is passed through the cystoscope into the bladder. The cystoscope is then withdrawn, leaving the wire in place. As the cystoscope is being withdrawn, the urethra is observed for any evidence of transurethral passage of cryoprobes or thermocouples (Fig. 1). The scope is then exchanged over the guidewire for a urethral warming catheter. Two freeze-thaw cycles are then performed as described previously. 1,2 Once the final thaw is complete, all probes and thermocouples are removed, and the urethral warming catheter is exchanged for a standard Foley catheter. Hemostatic pressure is applied to the perineum for a short time before dressing the puncture wounds with a sterile dressing.
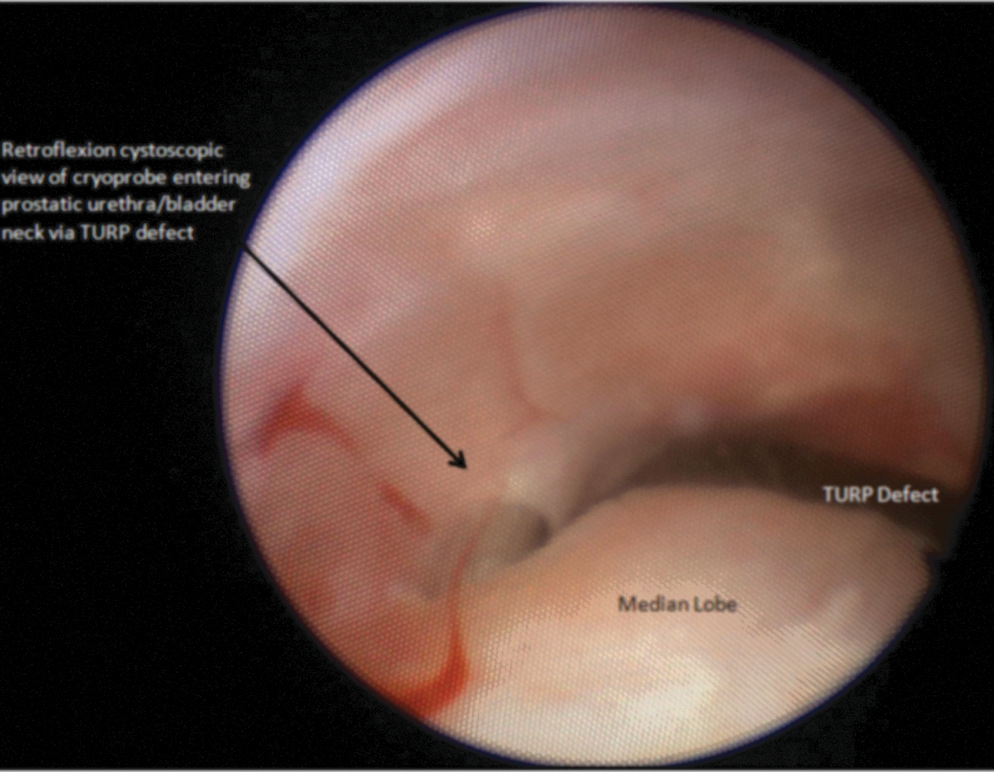
Retroflexion cystoscopic view of the cryoprobe entering prostatic urethra/bladder neck via TURP defect. TURP=transurethral resection of the prostate.
Discussion
This technique has now been used in 20 cases at our institution. Cystoscope placement at the onset of the procedure with continuous retroflexed viewing of the bladder neck in conjunction with transrectal ultrasonography allowed for accurate cryoprobe placement in all cases. In five cases, probes were observed to pierce the bladder neck or prostatic urethra, and this real-time observation of the bladder neck allowed for immediate withdrawal and repositioning of the cryoprobe. In several cases, real-time observation of the bladder neck allowed us to observing tenting of the bladder mucosa during insertion, allowing us to immediately halt insertion and prevent a bladder puncture. No cystoscope damage or instances of inadvertent transurethral misplacement of probes or thermocouples was observed in our series. There were no complications attributable to this technique.
The technique of continuous retroflexion cystoscopy in prostate cryoablation does not necessitate the use of any additional or specialized equipment when compared with traditional techniques. By allowing the cystoscope to remain inserted and passively retroflexed in a “hands-off” fashion, both the surgeon's hands are freed for insertion and manipulation of cryoprobes while maintaining a continuous view of the bladder neck. There is no danger in leaving the cystoscope light source engaged, because the bladder is adequately distended with sterile water. The continuous visualization of the bladder neck provided by this technique allows for immediate and accurate identification and repositioning of a probe misplaced into the bladder lumen or prostatic urethra. We have found this technique to be particularly helpful in cryoprobe placement for patients who have undergone previous transurethral resection of the prostate (TURP). In such cases, the prostatic urethral irregularity often makes cryoprobe placement unreliable. In fact, during such a case, we observed the cryoprobes entering the prostatic urethral lumen via the TURP defect, although on concurrent ultrasonography, it appeared that the cryoprobe tips were still traversing prostatic tissue. This technique allowed for immediate identification and retraction of the misplaced cryoprobes into prostatic tissue under direct vision. In addition, the scope can be manipulated within the urethra to facilitate identification of the urethral sphincter, sometimes difficult to visualize via ultrasonography, thereby assisting with proper placement of this very important thermocouple. Furthermore, in addition to making thermocouple and cryoprobe placement more efficient, this technique may decrease operative time by eliminating the steps of Foley catheter insertion and removal before cystourethroscopy.
There is essentially no learning curve associated with this technique, as urologic surgeons performing cryoablation can be assumed to be proficient in cystourethroscopy. In addition, there is no increased financial cost of using this technique, because the use of cystourethroscopy to ensure that the bladder and urethra have not been breached is standard. Furthermore, there should be essentially no risk of damage to the cystoscope or transurethral mispassage of probes or thermocouples if the standard 0.5-cm periurethral “no-freeze” zone is respected when placing probes. This technique can be recommended for use in all patients who are undergoing cryoablation of the prostate.
Footnotes
Disclosure Statement
No competing financial interests exist.