
Abstract
Objectives:
Nonpalpable testes account for 20% of cryptorchidism. Laparoscopy is now the mainstay in management, but open surgery has been the only option for many patients in the past and even today. We suspected that open exploration may have missed gonads in presumed negative open exploration. As abdominal gonads are even more prone to cancerous degeneration, we proposed laparoscopic re-evaluation to patients with previous inconclusive open exploration for impalpable testis.
Patients and Methods:
All boys presenting to our referral center with past history of inconclusive open exploration for nonpalpable testis or with clinical or lab evidence of functional testicular tissue were consecutively offered laparoscopic re-exploration. Standard diagnostic laparoscopy with same-stage laparoscopic orchiopexy or one stage Fowler procedure was employed as required. The presence, number, and site of detected gonads were recorded.
Results:
141 male patients with nonpalpable testis comprising 171 nonpalpable gonads were laparoscopically explored with no adverse events. Sixteen patients (19 gonads) already had a negative open exploration. Seven gonads were discovered in these boys, 5 iliac and 2 retrovesical.
Conclusion:
Although a modest number of samples, our results underscore the prevalence of missed diagnosis. Obviously, laparoscopic re-exploration is indicated when a child with previous bilateral inguinal exploration presents with hormonal evidence of functioning gonadal tissue. Further we now recommend laparoscopic re-evaluation in most patients with nonpalpable testis and history of negative open exploration altogether.
Introduction
Classic surgical teaching dictates that any nonpalpable testis must be accounted for by exploration to bring it to one of three fates: a, reposition the gonad into a palpable location, b, remove a nonviable or dysgenetic organ, or c, definitively prove the absence of a missing aplastic or vanished testis.
Although laparoscopy has become the mainstay in the management of nonpalpable testes in most major centers, open surgery continues to be widely utilized. The very few reports comparing open and laparoscopic orchiopexy have shown both to be suitable modalities for treatment, but the same is not certain for diagnostic accuracy. 5,6 There are many reports that proclaim laparoscopy as the best surgical management modality for the nonpalpable testis. 1,3,7,8
After confronting virilization in the first of our patients who had been declared anorchic at an early childhood surgery, followed by productive laparoscopic exploration; we began to look into the possibility of misdiagnosis at initial open explorations for nonpalpable testis as discussed further on.
Patients and Methods
We reviewed all of our patients who had undergone laparoscopic exploration for nonpalpable UDT at our referral center in the previous 9 years. Past surgical data on patients with history of previous open exploration for cryptorchidism was collected from their preceding hospital. As was our standard approach for the past decade, all primary patients presenting with nonpalpable testis after 9 months of age underwent diagnostic laparoscopy. The abdomen is initially explored through one umbilical port. Two additional trochars are added unless blind ending vas and vessels are unequivocally encountered on the side of concern. If a testis is found, orchiopexy follows standard laparoscopic method as adequately elaborated in previous reports.
Results
From Aug 2003 to Dec 2010, 141 boys with nonpalpable UDT aged 10 months to 15 years were evaluated at our center. Altogether 171 nonpalpable gonads were laparoscopically explored. Sixteen individuals had already undergone open inguinal exploration in the past (almost always before 2 years of age). Altogether, 19 impalpable gonads were re-explored by laparoscopy in these 16 boys. One of seven right-sided UDT, two of six left UDT, and two of three bilateral cases harbored testes which had been overlooked at the preceding open surgery, and were discovered during laparoscopy. Altogether seven gonads were discovered. Six were successfully pexed into the scrotum at the same session, by standard orchiopexy or Fowler Stephens technique as required. The seventh gonad, a dysplastic testis with disjoined epididymis was removed for cancer prophylaxis. Five of these gonads were found in the high pelvic (iliac) region as seen in Figure 1, and two in retrovesical position. (Fig. 2)

Testis found in the more frequent high pelvic/iliac location.
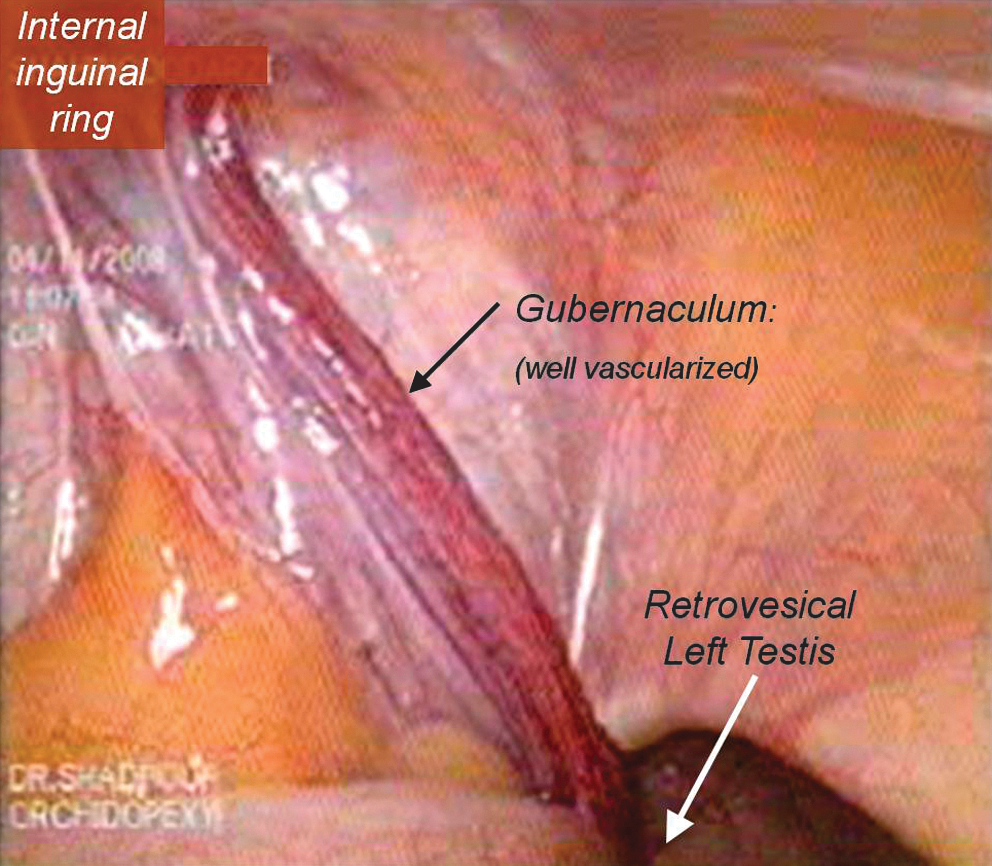
Testis in retrovesical location, second most frequent.
Imaging results preceding open surgery were unknown to us, but of all the new ultrasound scanning available for all patients, the gonad in only one retrovesical finding had been equivocally mentioned. Magnetic resonance imaging was negative in both patients who had undergone MRI. Laparoscopy later confirmed the absence of testicular tissue in one of these, but in the other we found high pelvic testis mistaken for nodal tissue.
We checked the follicle-stimulating hormone (FSH) level in two of three bilateral cases who were prepubertal, with 1.6-fold elevation in one boy who had both testes on subsequent laparoscopy. Our first case had already begun to virilize and so no additional test was carried out.
Intraoperative findings during laparoscopy were compared with the original operation report obtained from the past open procedure in 16 re-explored boys. In many cases detailed mention of individual findings regarding the vas, gonad, and spermatic vessels (and even excision of the nubbin one case) were lacking. Frequently the surgeons had only recorded their conclusion that is, absence of the respective testis. Encouragingly, none of two cases in whom blind vessels had been documented had a testis. However, two of three documented “blind vas” cases ended up with an overlooked testis: One with congenitally disjoined epididymis, and the other with an exceptionally long loop vas.
Discussion
Undescended testes carry increased risk for malignancy, most notably so in abdominal nonpalpable gonads. It is therefore mandatory to confidently determine the existence (or otherwise absence) of such tissue. 1 Laparoscopy has become the recommended diagnostic procedure to this end. 1,3,7,8
The overall utility of radiological evaluation in localizing a nonpalpable testis by ultrasonography and magnetic resonance imaging were very low in the 1990s. Although improved by advances in imaging technology and skill, diagnostic accuracy has never approached that of exploration. 1,9 –12 Further, surgical exploration is inescapable in the case of the nonpalpable testis where it serves both diagnosis and treatment.
In the first two cases of this series, history of open negative bilateral exploration for nonpalpable UDT with clinical or laboratory evidence of functioning testicular tissue (virilization or normal FSH) prompted our laparoscopic re-evaluation. Beyond that, any patient with nonpalpable UDT claimed testis-negative at open exploration, where the surgical findings fell short of fulfilling the above mentioned criteria was counseled on the odds and offered the option of laparoscopic re-evaluation. The same was done for patients with suggestive clues of unilateral formerly functioning testis (e.g., well developed ipsilateral hemiscrotum) but no nubbin orchiectomy.
To our knowledge very few reports have included laparoscopy in patients with previous negative exploration for impalpable testis. 2,13,14 They conclude that laparoscopy is an accurate method in documenting the diagnosis of a nonpalpable testis even in patients with negative previous exploration. Barqawi et al found gonads in 67% of 27 studied patients; including canalicular testes or testicular remnants in three on laparoscopic re-exploration. 2 Lakhoo et al studied 18 such boys and reported a 59% failure of previous open exploration. 13 Unlike our series which includes open abdominal exploration however, their patients had undergone simple inguinal orchiopexy alone. This could explain the relatively higher accuracy of the preceding open surgery reflected in lower rate of overlooked gonads (36.8%) in our series. Also contributing to this ratio could be wider access to hormonal screening and referral facilities, including those providing laparoscopic surgery, in this country compared with the time and place of previous reports.
Also of note, is that all gonads discovered in our patients were located far from the inguinal canal, in high iliac or retrovesical position, which would not have been accessible to most inguinal exposures. Two patients in our study with bilateral impalpable testes and previous history of negative open exploration had shown hormonal evidence of functioning gonadal tissue later on in life, and bilateral testes were confirmed on laparoscopic re-exploration.
In retrospect, it seems likely that open inguinal exploration for UDT is frequently terminated short of finding blind ending spermatic vessels, probably just after exploration of the inguinal area and the retroperitoneal space immediately adjacent to the internal inguinal ring. Thereby many such open orchiopexies are inconclusive as a diagnostic surgical exploration based criteria mentioned earlier on. Accordingly, those of our patients in whom blind vessels had been recorded, indeed had no ipsilateral gonad. However, a “blind ending vas” was by no means conclusive, even when clearly observed and documented. In fact, as demonstrated by our report, an apparently “blind vas” actually may not be “blind ending”, but a tight hairpin loop of a long looped vas, macroscopically resembling the former on open exploration. Laparoscopic magnification can facilitate this distinction.
Based on our findings, and those of previous reports including our own, 15 laparoscopy can make an important contribution to patients with inconclusive previous open exploration for impalpable testis. Particularly a noneunuch patient presenting with bilateral impalpable testis proclaimed anorchic on a previous open surgery, demands diligent evaluation.
Both diagnostic and therapeutic laparoscopy for cryptorchidism are considered low difficulty laparoscopic interverntions. 16 As such, the complication rate for these procedures is very low (0.4%). 16 Laparoscopic skills have been rapidly propagating throughout the urologic community. With such refined anesthetic methods and care, alongside polished surgical technique, laparoscopic re-exploration is advisable in such patients who are still considered at risk for testicular cancer. 2 For the less experienced in laparoscopy, and where access to such equipment is lacking, a formal systematic suprainguinal abdominal exploration such as detailed by Jones is in order. 17
Conclusion
Because of the particularly elevated risk of cancer in cryptorchidism with an abdominal testis, and high likelihood of overlooking the misplaced gonad during open inguinal exploration; unproductive previous open surgery for UDT must not preclude laparoscopic re-exploration, regardless of the findings on preoperative imaging. Second-look laparoscopy is imperative when a child with previous history of bilateral inguinal exploration presents at a later age with hormonal evidence of some functioning gonadal tissue, and in any patient with inconclusive previous surgical notes that is, anything short of blind ending vessels.
Footnotes
Disclosure Statement
None of the contributing authors have any conflict of interests, including specific financial interests, relationships and affiliations relevant to the subject matter or materials discussed in the manuscript, and there has been no specific funding for this study.