
Abstract
Background and Purpose:
Ureteroileal anastomosis strictures are well-known complications of ileal conduit urinary diversion that occur in 4% to 8% of patients. Open surgical repair is the standard definitive treatment with minimally invasive, endoscopic approaches developed to prevent the need for major surgery when possible. Robot-assisted surgery has been applied to most primary urologic procedures, but the role of this surgery in the management of complications is undefined. We report our experience with two cases of robotic repair of ureteroileal anastomotic strictures after robot-assisted cystectomy, the first such cases to our knowledge, and review the literature regarding management of these strictures.
Patients and Methods:
Two patients underwent robot-assisted ureteroileal anastomosis revision for left-sided strictures of 1 and 6 cm in length after failed endoscopic management. Three ports were used in the first and four in the second procedure. The diseased segment was identified, and the healthy end of the ureter anastomosed to a new site on the conduit with a temporary stent. In the second case, the conduit was mobilized and brought to the end of the ureter for a tension-free anastomosis because of the length of the stricture.
Results:
Both patients were discharged on the first postoperative day without complications and are without recurrence after nearly 2 and 3 years since the robotic procedure.
Conclusion:
Minimally invasive definitive revision of ureteroileal anastomotic strictures is feasible with a robotic surgical approach. The advantages of robotic instrumentation allowed successful repair in two patients after previous robot-assisted cystectomy and avoided major open surgery.
Introduction
Robot-assisted laparoscopic surgery has been applied to most primary urologic procedures, including radical cystectomy. 4 As with open cystectomy, complications of urinary diversion after robot-assisted cystectomy can occur, including ureteral anastomotic strictures. The role of robotic surgery in the management of such complications after the primary procedure is undefined. We report our experience with two cases of robotic repair of ureteroileal anastomotic strictures after robot-assisted cystectomy, the first such cases to our knowledge, and review the literature regarding management of these strictures.
Cases
Patient 1
A 53-year-old man underwent robot-assisted radical cystoprostatectomy for pT3aN0 bladder cancer with extracorporeal ileal conduit urinary diversion through the 3-inch extraction site incision without complications in the perioperative period. He presented to an outside hospital with urosepsis 4 months postoperatively. A left nephrostomy tube was placed for left hydronephrosis, and a left ureteroileal anastomotic stricture was subsequently found on antegrade nephrostography. Antegrade stent placement was unsuccessful, such that the stricture was reevaluated by left antegrade ureteroscopy 1 month later, revealing a tight stricture 1 cm from the conduit on simultaneous loopogram without any evidence of tumor recurrence on endoscopy and imaging (Fig. 1). Multiple attempts to place a wire through the stricture were unsuccessful.
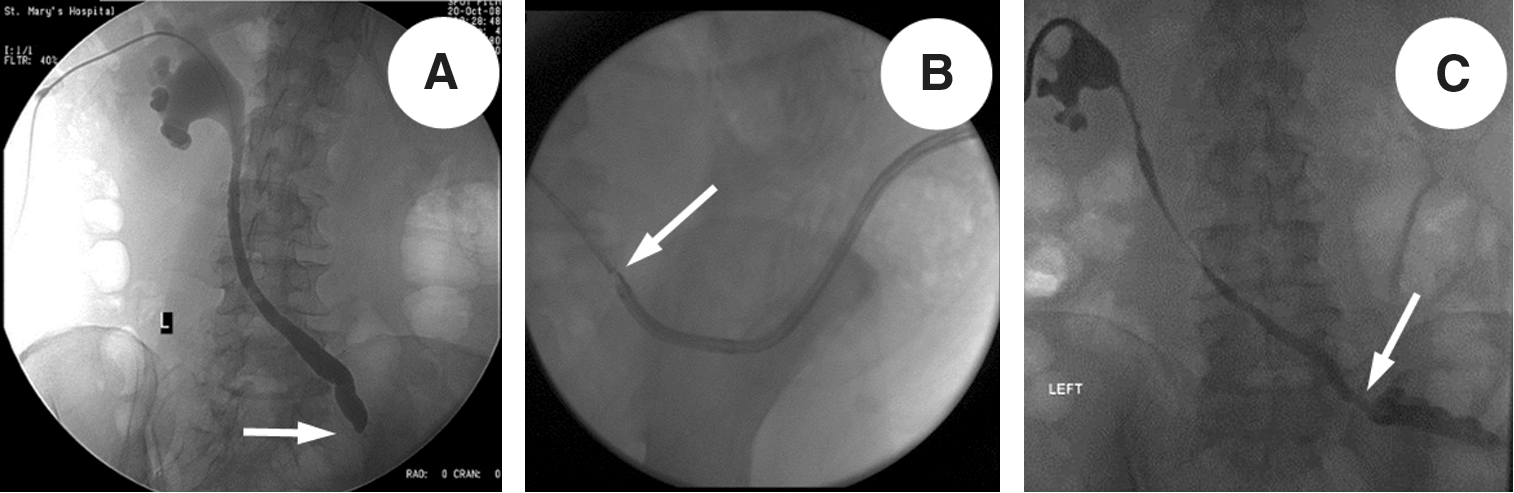
Left ureteroileal anastomosis stricture identified on antegrade nephrostogram
After a detailed discussion, the patient was offered robotic ureteroileal anastomosis revision with open repair at the same setting if unsuccessful robotically. The patient was positioned supine with the bed rotated to 30 degrees to elevate the right side. The procedure was performed using three ports (12 mm for the robotic scope and two 8-mm ports for robotic instruments). Ports were placed in triangulation around the internal end of the conduit, reusing two previous port sites from the original robot-assisted cystectomy, including the original camera-port site used for the robotic right arm and the original left instrument port site used for the camera (Fig. 2). Placement of an assistant port was planned if needed for suction or retraction, but because this was found unnecessary, additional adhesiolysis was not performed to make place for an assistant port and sutures were instead introduced as needed through the robotic ports by temporarily removing a robotic instrument. The healthy portion of the left ureter was readily identified after limited adhesiolysis in the region surrounding the conduit. A short stricture at the anastomosis site of approximately 1 cm in length was identified.
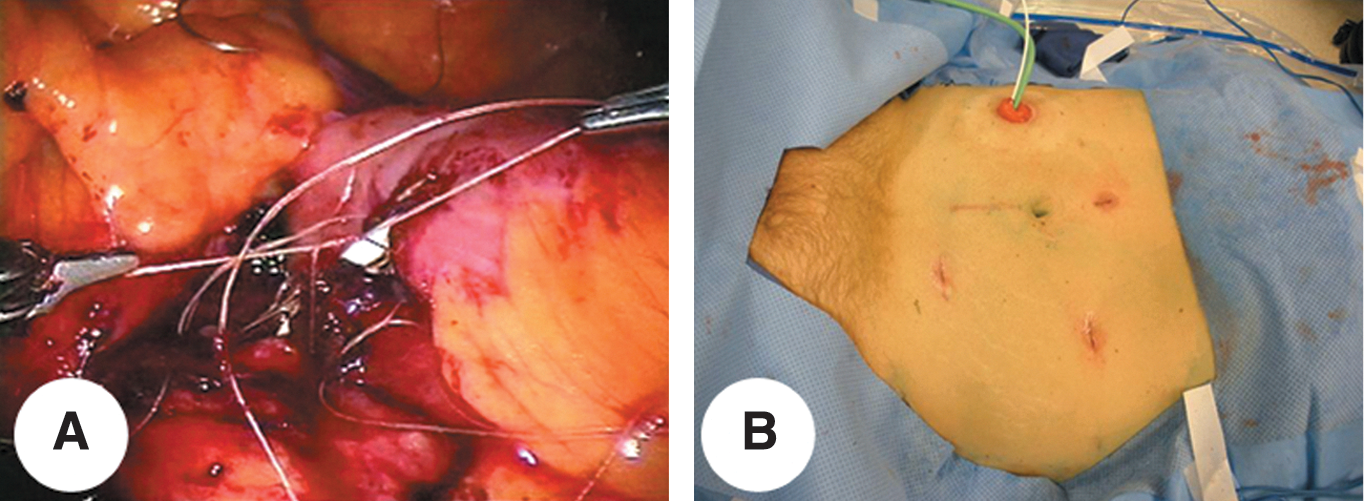
Intraoperative image of interrupted sutured anastomosis after all sutures placed and stent advanced through stoma at bedside
The dilated ureter proximal to the stricture was detached from the conduit leaving the scar in place, and the healthy end of the ureter was reimplanted at a new site on the conduit using interrupted 4-0 polyglactin sutures. Bleeding at the cut end of the ureter was used to indicate that an appropriate site had been chosen for the new anastomosis. A urinary diversion stent was placed across the anastomosis before completion by advancing a wire through a Yankauer suction tip guided through the stoma by the bedside assistant until the end could be seen at the anastomosis opening internally. The wire was then directed into the ureter with the robotic instruments, and the stent was then advanced over the wire.
Robotic parastomal hernia repair was then performed in the same patient by securing a mesh cut to a “C” shape to the fascial edges of the hernia defect around the internal aspect of the conduit with permanent suture. Operative time from incision to dressings was 178 minutes with 10 mL of blood loss, and the patient was discharged on the first postoperative day with uneventful recovery.
The stent was removed after 3 weeks, and an antegrade nephrostogram confirmed patency 2 weeks later before tube removal. No hydroureteronephrosis has been seen on follow-up CT imaging for cancer surveillance nearly 3 years later.
Patient 2
A 64-year-old man underwent robot-assisted cystoprostatectomy for muscle-invasive bladder cancer after chemotherapy achieved a complete response of nodal metastasis (pT3b, ypN0). Ileal conduit urinary diversion was performed extracorporeally. Five months later, the patient presented with renal insufficiency with a serum creatinine level of 2.79 mg/dL (baseline 1.6 mg/dL) and bilateral hydronephrosis. A loopogram was performed and did not show reflux from the conduit into either ureter, prompting bilateral nephrostomy tube placement because obstruction was suspected bilaterally.
Two months later, antegrade nephroureterography and ureteroscopy revealed no obstruction on the right side such that the nephrostomy tube was removed without further event. On the left side, obstruction was confirmed, with a blind ending left ureter several centimeters from the conduit during simultaneous loopogram (Fig. 3). No evidence of recurrent tumor was seen on looposcopy or ureteroscopy.
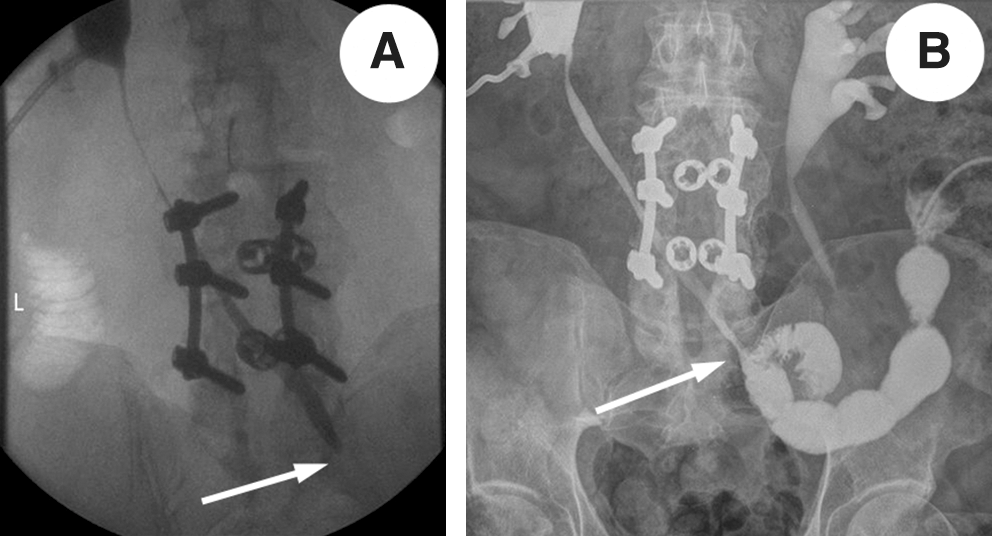
Representative images of antegrade nephrostogram identifying left ureteroileal anastomotic stricture with abrupt cutoff
Given the lack of a lumen to allow a wire to be placed across the stricture as well as the length of the stricture, definitive repair was recommended with robotic surgery if possible and open conversion if necessary. Ten months after the original procedure, robot-assisted ureteroileal anastomosis revision was performed using a four-port approach, triangulating robotic instruments around the end of the conduit with an additional assistant port (Fig. 4). The right ureteroileal anastomosis was identified first and used to identify the region of the left anastomosis on the other side of the conduit. The strictured left ureter was then traced retrograde until a healthy and larger caliber appearing end was seen, which was unfortunately all the way back to where the left ureter was crossing under the mesentery of the sigmoid colon.

Second patient with excised segment of ureter (left) and four-port approach reusing two from original-assisted cystectomy (right).
The diseased portion of ureter was excised and the remaining end spatulated using caliber and the pink color of the mucosa to confirm that a healthy area had been chosen for anastomosis. The ureter could not be mobilized because dissection was limited by the sigmoid mesentery such that the proximal end of the conduit was instead mobilized by adhesiolysis and brought to the healthy end of the ureter for a tension-free anastomosis at a new site on the conduit. A stent was placed before completion of the anastomosis, and the conduit was irrigated at the bedside to confirm a watertight repair. A Foley catheter was left in the conduit, but no peritoneal drain was left. Operative time from incision to dressings was 173 minutes with less than 25 mL of blood loss.
The patient was discharged on the first postoperative day without complications. Pathologic evaluation revealed a 6-cm strictured ureter without malignancy. The stent was removed 5 weeks later with a nephrostogram confirming patency at 3 months after the revision, at which time the nephrostomy tube was removed. A loopogram at 6 months revealed free reflux without obstruction bilaterally. Nearly 2 years since the revision, the patient remains without evidence of bladder cancer on surveillance imaging and with stable renal function.
Discussion
Management of ureteroileal anastomotic strictures is challenging, with several options described for the initial surgical approach. With the advent of endoscopic access to the upper urinary tract, most strictures are initially managed with balloon dilation (16%–83%), 2,5 –11 endoureterotomy (30%–50%), 5 and/or stent placement (45%). 12 Initial minimally invasive management may avoid definitive open anastomotic repair, but the success rate for all endoscopic interventions declines with time and with repeated interventions exacerbating scarring (Table 1). All endoscopic techniques share a common limitation in that they do not address the presumed etiology of the stricture, thought to be ischemia of the anastomosed tissues leading to scarring.
DiMarco and associates 13 reported 79 procedures in 40 patients with ureteroileal anastomotic strictures (27 open repairs and 52 balloon dilations). 13 The patency rate at 1, 2, and 3 years was 92%, 87%, and 76% for open repairs and 15%, 15%, and 5% for balloon dilation, respectively. The authors noted that those strictures greater than 1.0 cm were more likely to recur, and those strictures that formed within 6 months of ileal conduit creation and were treated with dilation alone failed within 1 year. A similarly low success rate (18%) was also reported by Kwak and colleagues 14 in their cohort of patients that included 18 ureteroileal anastomotic strictures with at least 9 months of follow-up even with repeated dilations up to four times at 1-month intervals.
Liatsikos and coworkers 15 evaluated the use of self-expandable, metal stents for 3 to 8 cm ureteroileal anastomotic strictures and reported encouraging outcomes, yet only after secondary interventions. The immediate clinical success rate was 71%, but 1 and 4-year patency rates were only 37.8% and 22.7%, respectively. Following secondary interventions on 15 ureters, the 1 and 4-year patency rates were 64.8% and 56.7%, respectively. Frequent imaging to assess for endoluminal hyperplasia and ingrowth was recommended because of this predisposition with metal stents.
Alago and colleagues 16 reported their experience using retrograde nephroureteral stents in 49 patients with benign ureteral strictures with periodic stent exchanges. The authors reported technical success in 56 of 61 renal units (91.8%) and clinical success in 44 of 49 patients (89.8%) with a mean clinical follow-up of 22 months, but delayed complications of these indwelling stents over the long term included urosepsis, stent encrustation, and stent dislodgement.
Lin and associates 3 performed Acucise endoureterotomy in 9 patients and reported a success rate of 30%. Of these 9 patients with 10 benign strictures, 70% needed subsequent open repair. Similarly, Laven and coworkers 17 in their cohort of 22 patients treated 15 renal units endoscopically with 16 renal units needing open revision. 17 The success rate for endoureterotomy at a median follow-up of 35 months was 50% (8 of 16) compared with 80% patency (12 of 15) after open revision. The authors noted that of the open procedures in which recurrent strictures developed, one patient had undergone preoperative radiation therapy and the other two had undergone previous endoureterotomy.
While endoscopic treatment may delay or avoid definitive repair in some patients, open surgical revision of ureteroileal strictures remains the gold standard, with long-term success rates of 80% to 93%. 1,13,15 Tal and associates 12 identified 28 patients in whom ureteroileal strictures developed at a median of 7 months postoperatively, with 75% diagnosed by 1 year after the original surgery. 12 With a median follow-up after treatment of 62.5 months, long-term stent placement was chosen for 45% of patients, and in those who underwent attempted repair, balloon dilation failed in all while open repair was successful in 93%.
In these initial two patients who were treated with robotic anastomosis revision, both received diagnoses of strictures within the initial 6 months after the original surgery. Based on the findings of complete obliteration of the ureteral lumen, endoscopic management was not possible, and patients were offered attempted revision robotically. Even open repair can be challenging in such patients because of adhesions from the previous abdominal procedure and scarring in the area of the ureteroileal anastomoses, but applying the principles of the open repair to the robotic approach and the benefits of robotic instrumentation allowed success.
The critical steps of the operation include identification of the stricture site and length, recognition and mobilization of the healthy end of the ureter without compromising vascularity, and precise anastomosis of the ureter to the ileal conduit. These steps were successfully performed robotically and allowed these patients, who had both undergone minimally invasive robot-assisted cystectomy, a minimally invasive repair for their complications.
In both cases, the original ileal conduit creation had been performed extracorporeally. While doing so through a purposely small extraction incision may predispose to strictures from possible devascularization of particularly the left ureter to reach the skin level, we adjusted our technique for extracorporeal diversion after these two cases. This includes mobilization of the ureters no higher than just above the common iliac vessels, trimming of the ureters to the bare minimum length needed, and creation of the ureteroileal anastomoses below the skin level through the incision. With these modifications, we have not seen any strictures in the subsequent 30 patients with extracorporeal diversion with a minimum of 1 year of follow-up such that our overall rate of strictures is no worse than reported with open cystectomy.
While some have advocated for a completely intracorporeal technique to avoid this potential complication, we abandoned this technique more than 3 years ago having found that it adds an unreasonable amount of operative time. In obese patients in whom we become concerned that the less dissected ureters may not be of adequate length, we leave the robot draped during extraction and fashion the conduit and perform the bowel anastomosis through the extraction incision. Then, if the ureteroileal anastomoses cannot be performed through the extraction site, the fascia can be closed after reducing the harvested conduit and bowel and the robot redocked to perform the anastomoses robotically. Despite having patients of body mass index exceeding 40 kg/m2, we have not had any occasion in which we have needed to do this because even ureters that do not reach the skin level can be anastomosed below skin level inside the wound; we have found that the Alexis® wound retractor (Applied Medical Resources Corporation, Rancho Santa Margarita, CA) makes this possible with ease. Nevertheless, we would advocate for this hybrid extra/intracorporeal diversion technique rather than a completely intracorporeal technique so as to eliminate the significant time needed for intracorporeal bowel work.
As with endoscopic management, it is likely that not all ureteroileal anastomotic strictures will be amenable to robotic repair. A limitation of robotic and laparoscopic surgery remains the need for access to the abdominal cavity, which can be challenging in patients after major surgery, including bowel manipulation for conduit creation. It is possible that these two patients having undergone previous robot-assisted cystectomy rather than open cystectomy may have reduced intraperitoneal adhesions and made these procedures less daunting. Nevertheless, because endoscopic treatment is often offered to patients with ureteroileal strictures to attempt avoidance of definitive open surgical repair, a strategy of attempting robotic repair with patients prepared for possible need to convert to open surgery is not unreasonable. Defining which patients are best suited to robotic repair and whether definitive robotic repair should be considered even before attempted endoscopic management will require further experience.
Conclusion
Minimally invasive definitive revision of ureteroileal anastomotic strictures is feasible with a robotic surgical approach. The advantages of robotic instrumentation and optics provided adequate precision for successful repair in two patients after previous robot-assisted cystectomy and may aid in allowing this complex procedure to be performed in minimally invasive fashion.
Footnotes
Disclosure Statement
No competing financial interests exist.