
Abstract
Background and Purpose:
Lithotripsy is an established method to fragment kidney stones that can be performed without general anesthesia in the outpatient setting. Discomfort and/or noise, however, may deter some patients. It has been demonstrated that audiovisual distraction (AV) can reduce sedoanalgesic requirements and improve patient satisfaction in nonurologic settings, but to our knowledge, this has not been investigated with lithotripsy. This randomized controlled trial was designed to test the hypothesis that AV distraction can reduce perceived pain during lithotripsy.
Patients and Methods:
All patients in the study received identical analgesia before a complete session of lithotripsy on a fixed-site Storz Modulith SLX F2 lithotripter. Patients were randomized to two groups: One group (n=61) received AV distraction via a wall-mounted 32″ (82 cm) television with wireless headphones; the other group (n=57) received no AV distraction. The mean intensity of treatment was comparable in both groups. Patients used a visual analogue scale (0–10) to record independent pain and distress scores and a nonverbal pain score was documented by the radiographer during the procedure (0–4).
Results:
In the group that received AV distraction, all measures of pain perception were statistically lower. The patient-reported pain score was reduced from a mean of 6.1 to 2.4 (P<0.0001), and the distress score was reduced from a mean of 4.4 to 1.0 (P=0.0001). The mean nonverbal score recorded by the radiographer was reduced from 1.5 to 0.5 (<0.0001).
Conclusions:
AV distraction significantly lowered patients' reported pain and distress scores. This correlated with the nonverbal scores reported by the radiographer. We conclude that AV distraction is a simple method of improving acceptance of lithotripsy and optimizing treatment.
Introduction
Despite these improvements in lithotripsy, patients can still experience anxiety and pain during treatment, and this can result in reduced patient tolerance and erratic respiration leading to difficulty targeting the stone and a consequent reduction in treatment efficacy. Analgesia regimens for lithotripsy vary, but some centers give opioid-based analgesia, and occasionally sedation is needed. Reducing patient pain and distress during lithotripsy is not only desirable for compassionate reasons but also could reduce analgesia requirements, accelerate postprocedure recovery, allow maximal energy delivery, and lead to overall improvement in stone fragmentation.
The use of various distraction techniques to reduce pain and anxiety has been reported in other medical procedures. 3,4 The published effects of music alone on pain perception and analgesia requirements during lithotripsy have been equivocal. 5 –7 In this study, we tested the hypothesis that combined audio and visual (AV) distraction (using a television and wireless headphones) can decrease the perception of pain during lithotripsy. To our knowledge, this is the first study to evaluate the effects of AV distraction on pain perception in lithotripsy.
Patients and Methods
We based our estimate of the sample size needed for the study on the assumption that there would be at least a 30% reduction in the perception of pain after AV distraction was given. A power calculation predicted a requirement of at least 48 patients in each group, assuming a P value of 0.05 and a power of 80%.
Between February and June 2011, patients undergoing elective outpatient lithotripsy for ureteral or renal stones were recruited prospectively. Emergency patients and those with ureteral stents in situ were excluded. All lithotripsy treatments were performed on the same Storz Modulith F2 lithotripter by one of two experienced radiographers. Lithotripsy sessions were evenly distributed between the two radiographers. All patients were treated in a supine position using fluoroscopic guidance only. All patients received the same preprocedure analgesia, antiemetic, and prophylactic antibiotics (pethidine 100 mg intramuscularly, diclofenac 75 mg per rectum, prochlorperazine 12.5 mg intramuscularly, ciprofloxacin 100 mg orally). This was administered a few minutes before treatment in the same manner for both groups.
Lithotripsy was delivered at low energy for ∼200 shocks to acclimatize the patient to lithotripsy and then gradually increased to the highest tolerable/maximum recommended intensity at a frequency of 2 Hz for a maximum of 4000 shocks. We aimed to deliver 4000 shocks in each treatment in total but reduced this if the patient could not tolerate the treatment or if the stone was adequately fragmented. This resulted in most treatment times lasting around 35 to 40 minutes. Intensity of each treatment was recorded (number of shocks given, highest energy reached, and highest frequency reached), and the mean intensity of each group calculated (mean intensity=mean number of shocks×mean highest energy reached×mean highest frequency reached).
Patients needing epidural anaesthesia or treatment in the prone position were excluded. Of the 137 patients approached for randomization, 6 were unwilling to participate and 13 had incomplete assessment forms. Consequently, 118 patients were eligible for evaluation. These were randomly allocated into two groups. Group 1 received no AV distraction (n=57) and group 2 received AV distraction (n=61).
AV distraction was provided via a wall-mounted 32-inch (82 cm) television (Technika) with wireless headphones (Sony). A selection of 30 different DVDs of 30-minute television programs were given to the patient before the procedure allowing DVD selection to suit different patient's age/sex/personality. During the procedures in which no AV distraction was given, the television was covered with a white sheet.
Primary outcome measures were independent pain perception results from both the patient and radiographer. After the procedure, patients recorded both pain and distress levels on visual analogues scales (VAS) (using a 10 cm scaled VAS on which 0=no pain at all/no distress at all to 10=very painful/very distressful) (Fig. 1). The distance between the origin of the line on the left and the patient's mark was measured and the result in centimeters was recorded as score. All patients completed their pain scores in the postprocedure recovery area within 30 minutes of treatment. The recovery nurses were blinded to the group into which the patients had been assigned.
Patient visual analogue scales for pain and distress.
The radiographer recorded a nonverbal pain score during the procedure (scale 0–4). Marks were given for any nonverbal clues of visible distress or pain of the patient; vocal complaints, facial grimaces and winces, bracing and restlessness (Table 1). Each of the four criteria was scored as 0 or 1, giving a minimum score of 0 and maximum score of 4.
The Mann-Whitney comparison was used for statistical analysis. A P value of 0.05 or less was regarded as statistically significant.
Results
The demographics of the two groups were comparable. The mean age of the no-AV group was 53.4 (median 54, range 24–88). The mean age of the AV group was 51.7 (median 52, range 26–79). In the no-AV group, there were 25/57 (44%) female patients compared with 28/61 (46%) the AV group. In the no-AV group, 28/57 (49%) of the stones were right sided,and in the AV group, 36/61 (59%) were right sided. In the no-AV group, 37/57 (65%) of the stones were in the kidney and 20/57 (35%) were in the ureter compared with the AV group where 44/61 (72%) were in the kidney and 17/61 (28%) were in the ureter (Table 2). The mean treatment intensity was slightly higher in the AV group (48166) compared with the no-AV group (43662) (Table 3).
AV=audiovisual.
AV=audiovisual.
Mean pain scores were significantly lower in the AV group compared with the non-AV control group, with a reduction from 6.1 to 2.1 (P<0.0001) (Fig. 2). Similarly, the patients' distress scores were significantly lower in the AV distraction group from 4.4 to 1.0 (P<0.0001) (Fig. 3). Correspondingly, the pain score recorded by the radiographer was significantly lower in group 1 (the AV distraction group) compared with the control group with no AV distraction (P<0.0001) (Fig. 4).

Patient pain perception scores. Audiovisual (AV) distraction significantly reduced the pain perception scores (P<0.0001) irrespective of stone site.
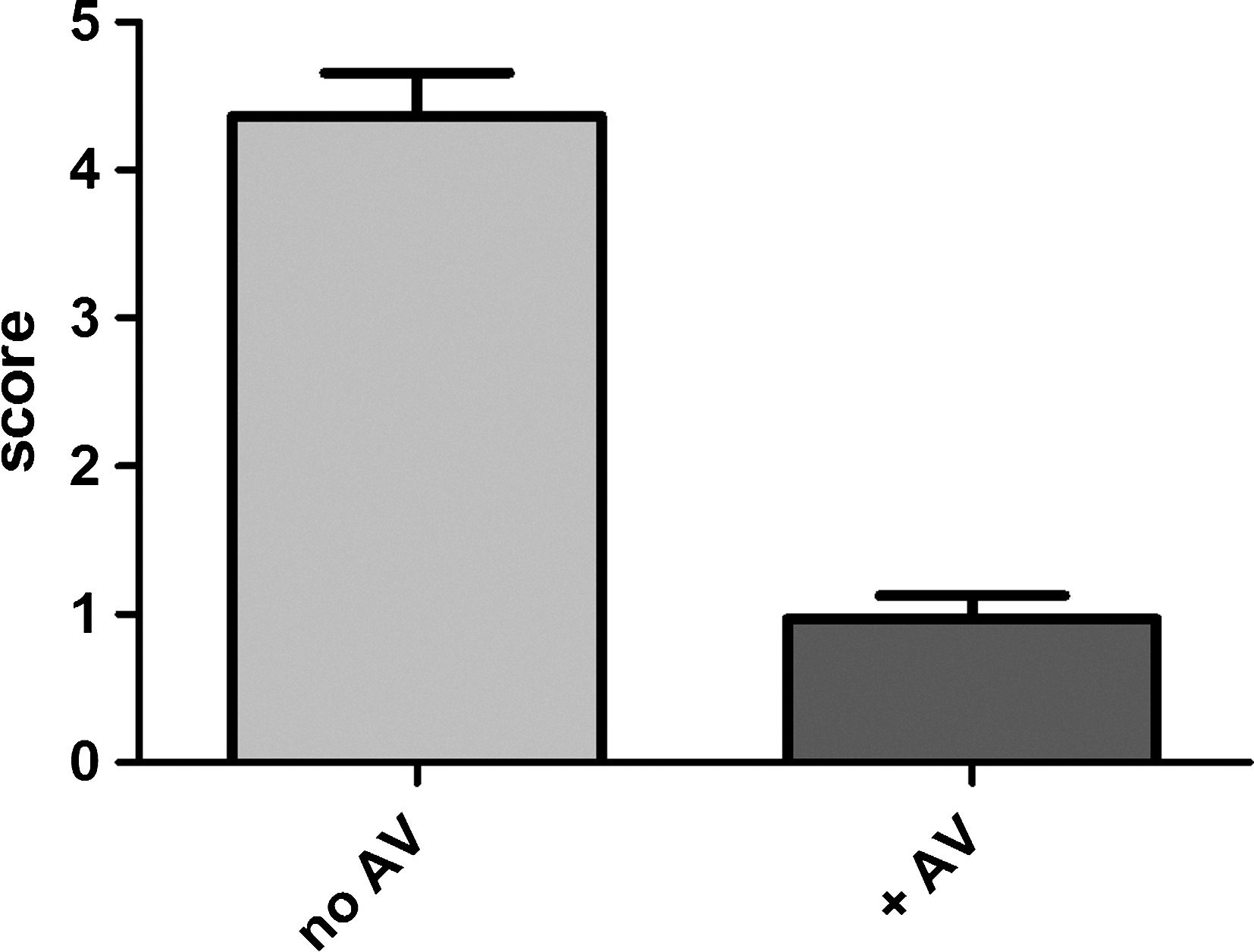
Patients' distress perception score.

Pain perception score as recorded by radiographer.
The reduction in perceived pain with AV distraction was observed irrespective of stone site (ureter/kidney) (Fig. 2). Also, significant reductions in distress and observed pain scores were noted in both ureteral and kidney stones (data not shown).
Virtually all patients in both groups would agree to undergo lithotripsy again (98% of the group with no AV distraction and 100% of the group with AV distraction).
Discussion
The use of various distraction techniques to reduce pain and anxiety has been reported in other medical procedures. 3,4 The use of such techniques, however, has not been described during lithotripsy treatments for renal calculi.
Consistent with the literature, our study demonstrates that lithotripsy is generally well tolerated with relatively small amounts of simple analgesia. 8 –10 Even in the group that did not receive AV distraction, 98% of the patients would be happy to have the treatment again. These patients, however, did find the procedure moderately painful (mean score 6.1) and distressful (mean score 4.4). Addition of AV distraction proved an effective and relatively low-cost method that significantly reduced both the pain and distress from lithotripsy. Patient comfort has several potential clinical benefits: Repeated treatments will become more acceptable to the patient and may allow avoidance of more invasive procedures; a comfortable patient is less likely to move or have erratic respiration, reducing targeting maneuvers and treatment duration; and reducing pain perception may allow the operator to maximize the intensity of treatment to improve stone fragmentation efficacy.
The introduction of AV distraction during lithotripsy in our study has given us evidence that both pain and distress scores can be lowered by a simple measure such as distraction. These results are corroborated by the pain scores recorded independently by the radiographer during the procedure. Further studies are needed to improve analgesia and distraction therapy to establish the optimum for patient experience, treatment efficacy, and departmental productivity.
Conclusion
This randomized trial demonstrated that AV distraction can reduce the perceived and observed pain and distress in patients undergoing lithotripsy for renal or ureteral calculi.
Footnotes
Acknowledgments
We would like to thank Jackie Redgwell, Mandy Spencer, and Paul Martin for preparing the AV equipment and for help with collection of data for this trial.
Disclosure Statement
No competing financial interests exist.