
Abstract
Introduction:
Many surgical training programs utilize simulation-based strategies for instruction and assessment of laparoscopic skills. While the use of inanimate, animate, and virtual-reality simulation for basic or procedural skills training has been well described, the use of simulation for the purpose of training surgeons in managing intraoperative laparoscopic complications has been given less attention. We describe a novel, affordable inanimate surgical model for use in simulation-based training of laparoscopic renal hilar vessel injury management.
Methods:
Using a laparoscopic box trainer, a half-inch Penrose drain, standard silicone intravenous tubing, and a commercially available kidney part-task trainer, an inanimate surgical training model was developed to simulate various clinical scenarios involving renal hilar vessel injuries. To evaluate the construct validity of this training model, urology residents from the University of California, Irvine, completed a simulated scenario involving a renal vein injury (RVI) during laparoscopic radical nephrectomy (LRN).
Results:
This surgical model is able to simulate both renal arterial and venous injuries during laparoscopic radical and partial nephrectomy scenarios. Initial cost to construct the model was ∼800 U.S. dollars (USD) and each subsequent use was an additional 7 USD. Resident training level correlated strongly with technical performance (p<0.01) and “blood loss” (p=0.02) during the “RVI during LRN” scenario. The checklist and global rating scale used to assess performance demonstrated adequate reliability (Cronbach's α=0.82).
Conclusions:
While further validation, technical refinement, and improved fidelity are being considered, we present a novel, affordable surgical model for simulating laparoscopic renal hilar vessel injuries that is suitable for urology trainees.
Introduction
While many have now accepted and adopted the integration of simulation-based education (SBE) to address the changing surgical training paradigm, 5 –8 the majority of SBE in surgery has focused on instruction and assessment of basic surgical skills. With improving technology and software design, computer-based simulators with higher fidelity are being developed for procedural skills training. However, despite explicit regulatory and administrative mandates to reduce surgical errors and increase outcomes-based practices, relatively little attention has been directed at the use of simulation for training surgeons on the management of intraoperative surgical complications.
The majority of surgical training programs employ a single instructional method, namely didactic lectures, to teach surgical trainees the principles and techniques involved in managing intraoperative laparoscopic complications. While this approach is able to address many of the cognitive learning objectives, it does not allow the trainee to meet any of the associated skills-based psychomotor objectives related to management of intraoperative laparoscopic complications. As outlined by a conceptual framework proposed by Fitts and Posner, 9 learning a new skill involves not only a cognitive phase but also an associative phase involving practice and feedback. Since deliberate practice during high-stakes clinical surgery on human patients is neither feasible nor ethical, the use of simulation can aid in achieving more than just the “knows” and “knows how” but also the “shows how” and “does” levels of skills competency in surgical education. 10
Although there are a variety of inanimate, animate, virtual-reality, and team-based simulations available for basic and procedural skills training, to our knowledge, there are very few simulators that are specifically focused on technical skills training for the management of surgical complications. We present a novel, affordable, and reusable inanimate surgical training model that can be utilized for simulation-based technical training in the management of intraoperative laparoscopic renal hilar vessel injuries.
Methods
A proprietary laparoscopic pelvic box trainer (Karl Storz, El Segundo, CA) made out of acrylic was used to simulate the abdomen and intraperitoneal space (Fig. 1); provided that it is constructed out of a water-resistant material, any of the many different commercially available pelvic trainers would also suffice. A rubberized kidney part-task trainer (Item 7001; The Chamberlain Group, Great Barrington, MA) was placed within the pelvic trainer and used to simulate the kidney (Fig. 2); a variety of kidney models are commercially available, many of which would be equally suitable. Standard silicone intravenous (IV) tubing and a half-inch Penrose drain were passed through the hilar region of the kidney model to simulate the renal artery and vein, respectively (Fig. 3); the tactile feedback and resistance characteristics of silicone IV tubing resembles a renal artery while the more mobile and compressible quality of the Penrose drain approximates a renal vein. Irrigation fluid, stained red with food coloring for increased realism, was then connected to either end of the IV tubing and Penrose drain; the fluid can be pressurized such that the flow from a “hilar vessel injury” can simulate brisk bleeding. A standard fluid collection drape is utilized to capture all irrigation fluid from the base of the pelvic box trainer, and the entire area surrounding the pelvic box trainer is draped off to simulate a sterile field and to conceal the irrigation tubing. This surgical model is able to simulate both renal arterial and venous injuries during laparoscopic radical and partial nephrectomy scenarios.

Laparoscopic pelvic box trainer.
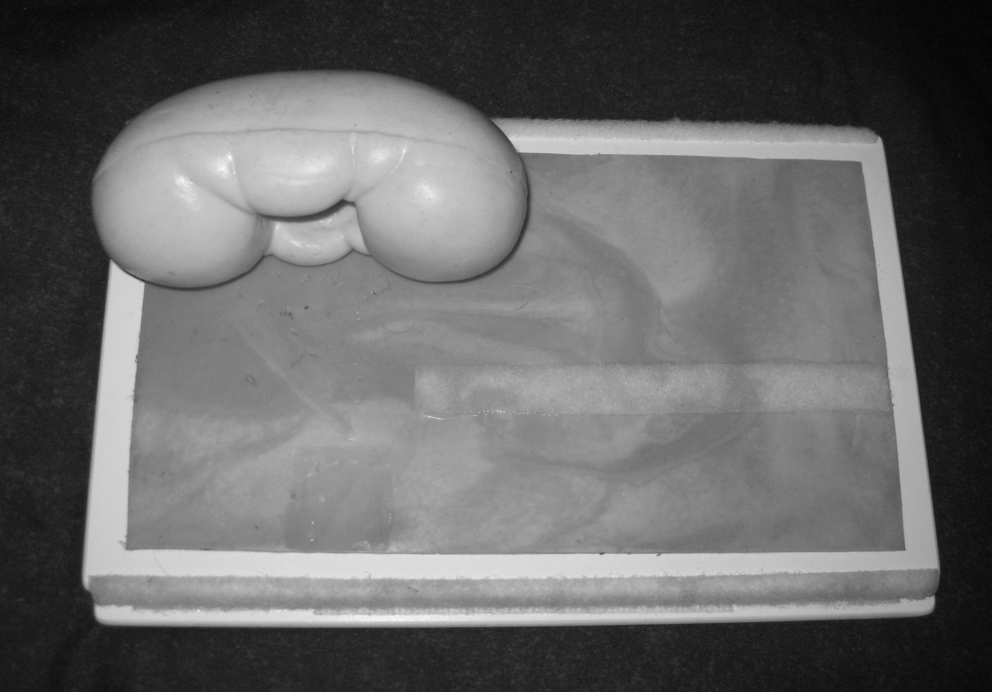
Kidney part-task trainer (The Chamberlain Group, Great Barrington, MA).
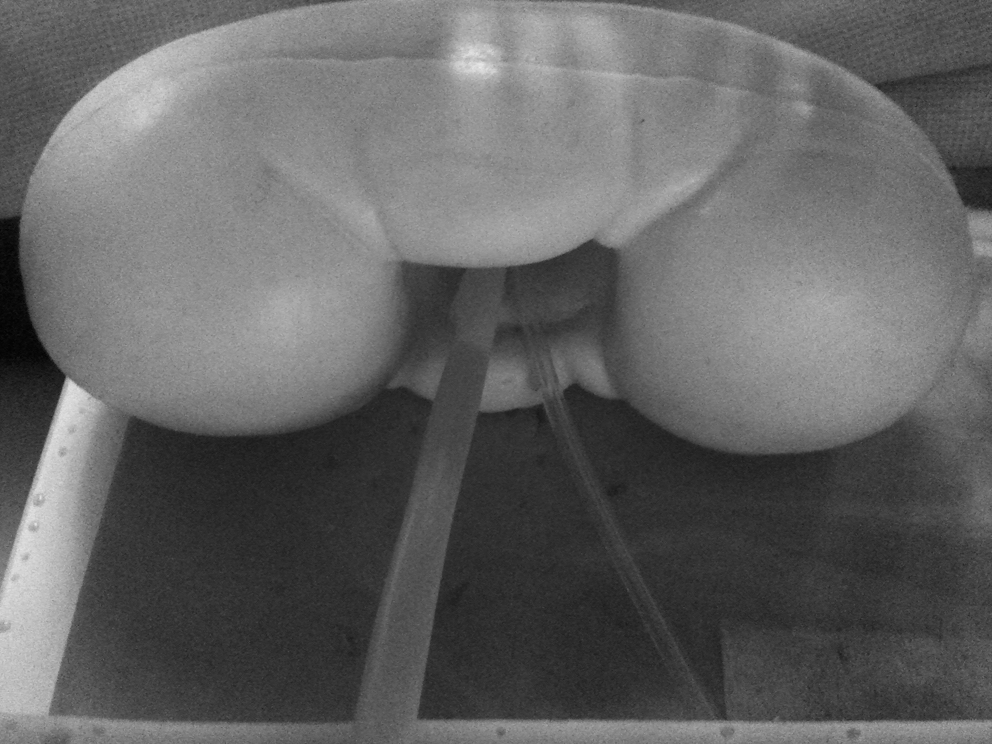
Kidney part-task trainer with simulated “renal vein” (Penrose drain) and “renal artery” (silicone intravenous tubing).
To evaluate the construct validity of a simulated scenario using this surgical model, the Institutional Review Board approval was obtained and urology residents from the University of California, Irvine, were asked to participate in a simulated scenario involving practice of the technique for management of the renal vessels during laparoscopic radical nephrectomy (LRN). The residents were not advised before the training session that a complication, renal vein injury (RVI), would occur during the LRN practice. The clinical scenario was standardized for all subjects and involved the preplacement of two 1-cm lacerations on the superior edge of the renal vein (i.e., Penrose drain).
Subjects were instructed that the goal of the SBE scenario was to develop pneumoperitoneum using a Veress needle technique and to place laparoscopic trocars in an adequate position to perform a right-sided LRN. They were then informed that upon insertion of a laparoscope, they would immediately see an already exposed renal hilum (i.e., the colon had already been mobilized off of Gerota's fascia) and that they were to perform an LRN beginning with the securing and ligation of the renal hilar vessels. All subjects were unaware of the RVI aspect of the simulation.
When the study subjects began ligation of the renal artery (i.e., IV tubing), the water irrigation connected to the Penrose drain was turned on to initiate “venous bleeding.” Subjects were responsible for managing the RVI complication in any manner they saw fit; completion of the scenario was determined to be the achievement of complete hemostasis or the loss of 2000 mL of “blood.” A standardized set of laparoscopic instruments, including graspers, needle drivers, kittners, metal clips, Hem-o-lok clips (Weck Closure System, Research Triangle Park, NC), endoscopic vascular staplers, and suture material were provided for all subjects; each of whom was free to use any or all of the provided materials. A trained “confederate” surgical assistant was present during the simulated scenario but only provided passive support, with no independent actions initiated. All performances were video-recorded for debriefing following the simulated scenario and for future analysis.
A task-specific checklist was developed specifically for performance assessment during the “RVI during LRN” simulated scenario and consisted of key technical elements to be assessed for a “RVI during LRN,” as determined by expert laparoscopic urologists using a modified-Delphi method 11 ; key elements included the demonstration of proper Veress needle technique, correct sequence of renal vessel ligation, proper technique for renal artery ligation, recognition of RVI with appropriate initial management (e.g., direct pressure, increasing pneumoperitoneal pressure, placement of additional ports, etc.), appropriate definitive renal vein laceration management, and achievement of full hemostatic control or timely decision to convert to open surgery. A global rating scale, which consisted of a 5-point Likert scale, was used to assess the overall technical performance of each study subject. Two independent laparoscopic urologists, trained to use the checklist and rating scale, were blinded to the level of training of each subject and assessed the video-recorded technical performances of each subject. In addition, “blood loss” was calculated by measuring the amount of water used during each simulated scenario.
Results
For the “RVI during LRN” scenario, eight urology residents ranging from postgraduate year 2 (PGY-2) to PGY-5 completed the simulation; all subjects were able to complete the scenario before reaching the 2000-mL blood loss threshold. Eighty-eight percent (7/8) of the subjects felt that the “RVI during LRN” simulated scenario was helpful for learning the technical skills necessary to manage laparoscopic RVIs. Similarly, 88% felt that the fidelity of the model was adequate for trainees.
Based on blinded, expert assessment of performance, junior (PGY-2–3) and senior (PGY-4–5) residents scored 57.9±7.4 and 75.0±2.7 on the task-specific checklist and 1.75±0.5 and 4.00±0.0 on the global rating scale, respectively. Mean “blood loss” ranged from 200 to 1400 mL and was 1075±342 mL and 462±3 mL for junior and senior residents, respectively (Table 1). Using Spearman's rank correlation coefficients, level of training was found to significantly correlate with the checklist score (p=0.004), overall global rating score (p=0.002), and measured “blood loss” (p=0.022). The assessment device (task-specific checklist and global rating scale) demonstrated adequate reliability (Cronbach's α=0.82).
(4) represents the number of residents in each group.
Discussion
Within the current academic health care environment in North America, the traditional Halstedian paradigm of surgical training is inadequate to meet all of the learning objectives found in most training programs. With diminishing clinical exposure for trainees, reduced opportunities for directed teaching, the introduction of novel surgical technologies that increase the complexity of surgical procedures, and escalating legal and administration emphasis on patient safety and the reduction of medical errors, it is imperative that surgical training programs implement other educational strategies such as SBE to adequately meet certain skills training objectives. For example, the development of the psychomotor skills and clinical judgment necessary to competently manage difficult intraoperative laparoscopic complications (such as renal vascular injuries) requires more than the classic apprenticeship style of learning but rather it necessitates deliberate practice, timely feedback, and opportunities to refine behavior. 4,5,12,13
Over the past two decades, urologists have witnessed the gradual permeation of laparoscopy into clinical practice to the point that it has now become the gold standard treatment for many urologic disease processes. Despite having developed a “critical mass” of proficiency throughout the field of urology, laparoscopic complications are not uncommon and as such it is still imperative that surgical trainees learn the principles of, and basic skills required for, managing intraoperative laparoscopic complications.
The aviation industry has long led the charge with respect to the use of simulation-based instructional strategies to train learners to deal with errors and complications. The aviation industry is dedicated to, and has institutionalized, the use of low-stakes, computer-based simulation to provide pilots with opportunities for sustained, deliberate practice and immediate expert feedback to improve management skills of in-flight problems, malfunctions, and disasters. 14 –16
Within medicine, SBE for training in complications management has predominantly been championed by anesthesiology, critical care, and emergency medicine subspecialties. Significant literature can be found in these fields documenting the integration of hi-fidelity SBE methods of instruction into existing training curricula. 17 –23 More recently, team-based training has emerged as a popular instructional method aimed at reducing miscommunication and errors among health care team members in high-pressure, high-stakes environments, such as the operating room, trauma bay, or even during cardiac arrests. 24 –26 In urology, team-based training is still a very new concept with most studies aimed at instruction and assessment of communication skills between health care providers or the theoretical, cognitive management of intraoperative complications. 27,28 While a few virtual-reality simulators that include modules involving the management of surgical errors or complications do exist, such modules are rudimentary and have not yet been validated. 29 To our knowledge, our study describes the first surgical simulation-based training model for instruction or assessment of surgeons on the technical skills required to manage an intraoperative complication.
The initial cost to construct this inanimate surgical training model was ∼800 U.S. dollars (USD): kidney part-task trainer 595 USD, laparoscopic pelvic box trainer 200 USD, silicone IV tubing 14 USD, Penrose drain 0.49 USD. Each piece of tubing and drain was sufficient for two simulated scenarios and thus, each repeated simulation required a recurring cost of only 7.25 USD. Complete construction of the training model required ∼15-minute preparation time and replacement of the “renal vessels” between simulated scenarios required 5-minute total time.
The efficacy and validity of hi-tech virtual-reality surgical simulators has been well studied and their utility for instruction clearly demonstrated. Unfortunately, the high financial investment required to purchase such simulators is often quite prohibitive. The surgical model we have developed is relatively inexpensive in comparison to such simulators, making its utilization and integration into the majority of training curricula much more feasible. For under 10 USD per simulated scenario, this surgical model provides the trainee an affordable opportunity for deliberate practice in a low-stakes environment with the potential for formative and summative feedback.
In addition to the “RVI during LRN” scenario, this inanimate surgical model can be used for several different simulated clinical scenarios. For example, in a simulated case involving an RVI during a laparoscopic partial nephrectomy, a small laceration can be placed in the Penrose drain (either prior to the simulation or “inadvertently” caused by a confederate surgical assistant during the simulated scenario) and the trainee would then be required to identify the location of the bleeding, obtain adequate hemostatic control, and repair the laceration. Varying levels of difficulty can be integrated into the simulation by altering the location, size, and number of vascular injuries. In addition, the number of “renal vessels” included in the simulation can also be manipulated between scenarios simply by adding pieces of Penrose drain or IV tubing.
With the variability in simulated scenarios, this surgical training model can facilitate a “mixed practice” model 30 as well as the development of an individualized, competency-based curriculum, both of which are critical to improving durability of learned skills and the achievement of mastery learning. In addition to different clinical scenarios (e.g., LRN vs. laparoscopic partial nephrectomy), varying degrees of difficulty can be introduced within each scenario (e.g., one laceration vs. two lacerations, anterior injury vs. posterior injury, etc.) as well as unique situations such as instrument failure (e.g., stapler malfunction, etc.) or distractions (e.g., answering pager, distractive scrub nurse, etc.). Through the ability to alter the level of difficulty and add elements to increase fidelity of the simulated scenario, very realistic crisis situations can be simulated that require the trainee to consider a variety of options for management of a renal hilar vessel injury—critical to the process of developing not only surgical skill but also surgical judgment.
There are several limitations to this surgical training model. While the initial cost of the inanimate surgical model itself is relatively affordable, it does require access to a fully functional laparoscopy tower: laparoscope, light box, and TV monitor. Also, depending on the scenario, the cost of disposable instruments used per simulation (e.g., clips, sutures, and staples) may not be negligible for some training programs. In all likelihood, however, most surgical training centers will have some form of pelvic box trainer and related instruments available for practicing laparoscopic skills. Therefore, the majority of this simulation model is of little additional expense.
The current design and construction of the surgical model does not include a dissection aspect to the renal hilar vessel simulation, which can often be an important learning objective to the procedural training. Also, unlike its virtual-reality counterparts, this surgical model simulator has no scoring algorithm to collect data on various performance metrics and requires video-recordings of performance for future analysis or the presence of experts to provide immediate assessment of the trainee.
While the “RVI during LRN” simulation using this surgical model demonstrated construct validity, the evaluation involved only eight subjects and requires further validation in large, multi-institution studies. Also, while several different simulated scenarios are feasible with this model, only the “RVI during LRN” scenario was evaluated; independent validation of each of the various scenarios will be the focus of future research.
Conclusions
While further technical refinement, improved fidelity, and validity testing are required, we present a novel, affordable surgical model that can be utilized in a simulation-based training curriculum for the management of laparoscopic renal hilar vessel injuries. The current iteration of the surgical model is likely most suitable for urology trainees or novice laparoscopic surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.