
Abstract
Purpose:
To evaluate the feasibility of intensive laparoscopic training shortening the learning curve of laparoscopic suturing in surgical postgraduate students.
Materials and Methods:
Eighty-seven surgical postgraduate students participated in this study, including novice (N), junior (JR), and senior (SR) trainees. The N trainees were divided into novice control (NC) and novice experimental (NE) groups. The training curricula contain three stages: Fundamentals of laparoscopic surgery tasks, intensive laparoscopic suturing task, and laparoscopic enucleation model training. The NE, JR, and SR groups completed all three stages. The NC group just performed the first and third stages. The performances of each group were recorded and analyzed.
Results:
For the first stage, the SR group performed better than the N and JR groups. There was no significant difference in the post-test total scores between the N and JR groups, although the N group had lower pretest total scores. For the second stage, no significant difference was found in the post-test scores among the NE, JR, and SR groups, although the SR group had better pretest scores. For the third stage, the NE, JR, and SR groups had better performance than the NC group at the five exercises. There was no significant difference at the fifth exercise among the NE, JR, and SR groups, although the SR group performed better at the former four exercises.
Conclusion:
This study documented the feasibility of intensive laparoscopic training curricula shortening the learning curve of laparoscopic suturing in surgical postgraduate students, regardless of baseline experience.
Introduction
In the past decades, simulation of the laparoscopic operation has gained tremendous acceptance by abundant literature reports with a wealth of validation evidence supporting the efficacy of simulation-based training. 3 –6 It is considered an important adjunct to operating-room–based training for establishing and maintaining technical skills. Traditional courses to develop laparoscopic suturing skills are mainly aimed at residents and consultants. So far, there have been few studies concerning laparoscopic training in surgical postgraduate students in medical college. The opportunity for surgical postgraduate students to acquire these skills at an early stage of their career may reduce the learning curve and maximize the benefit of real patients. Furthermore, current training curricula need additional refinement to maximize the benefit of learners.
Aggarwal and colleagues 7 have shown laparoscopic suturing can be learned by junior residents in a 2-day training curriculum; this study is just a dry laboratory training curriculum. For better transferring of the training skills to the operating room, a wet laboratory training curriculum is indispensable. 8 Therefore, our study evaluates the feasibility of our intensive laparoscopic training curricula, which contain both dry and wet laboratory training programs, shortening the learning curve of laparoscopic suturing in surgical postgraduate students.
Materials and Methods
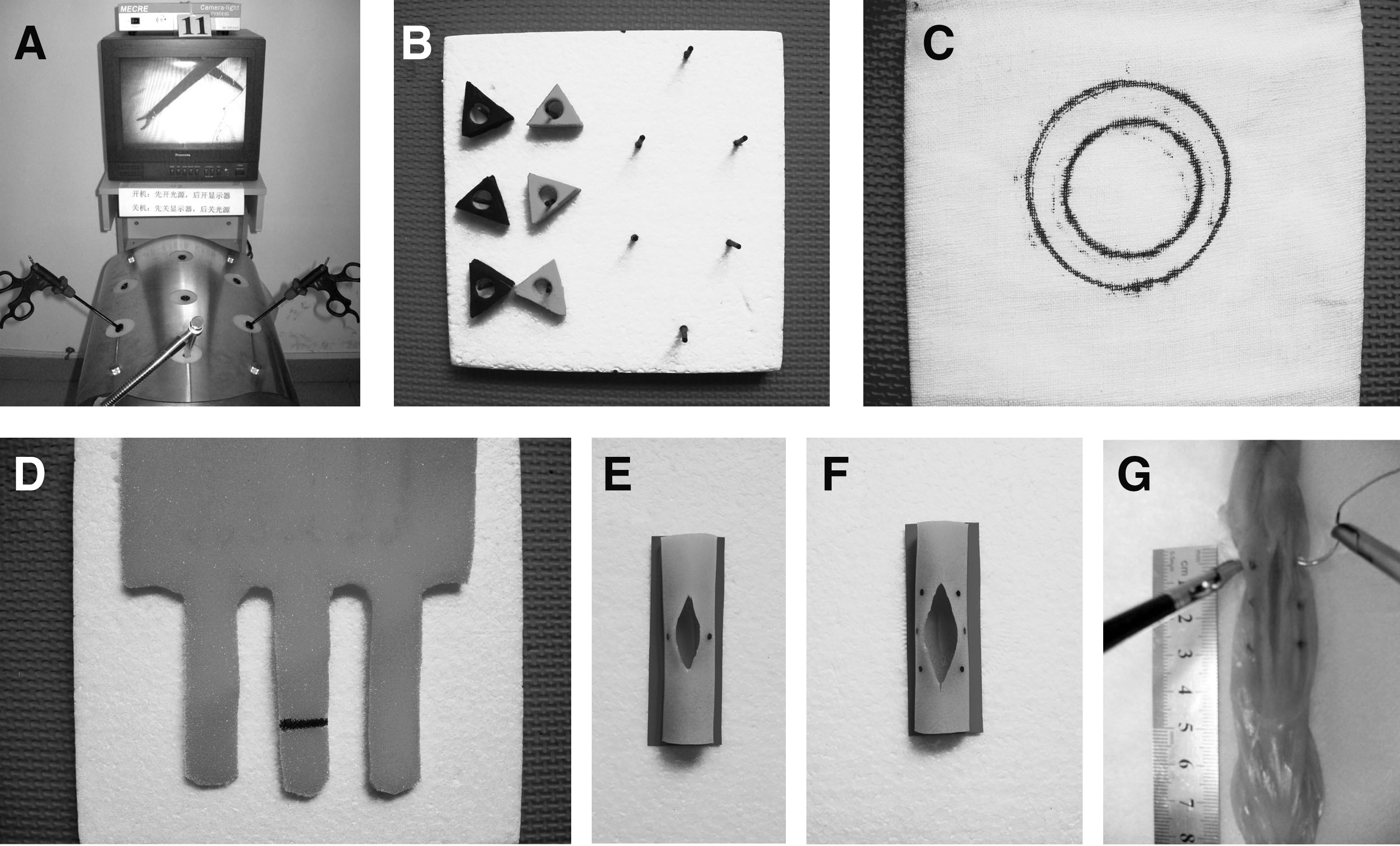
All of the study was conducted at the Laparoscopic Training Center, Medical College of Wuhan University. The training system used in this study was the Laparoscope Skill Trainer (Guangzhou Mecre Medical Equipment Co., China) (Fig. 1). Eighty-seven surgical postgraduate students from Medical College of Wuhan University completed a questionnaire at the beginning of the study, including demographics and baseline experience (Table 1). The participants were divided into different groups depending on baseline experience, including novice (N), junior (JR), and senior (SR) groups. The N group was defined as interns with no experience in laparoscopic techniques. The JR group was defined as interns with very limited experience (less than 10 laparoscopic operations, as assistants). The SR group was defined as interns with more than 50 laparoscopic operations as assistants. The laparoscopic training curricula contain three stages of training: Fundamentals of laparoscopic surgery (FLS) tasks (Fig. 1), intensive laparoscopic suturing task, and laparoscopic enucleation (LE) model training.
N=novice; JR=junior; SR=senior.
All the participants received the first stage of training. Then the N trainees were divided into novice control (NC) and novice experimental (NE) groups. The NE, JR, and SR groups completed the other two stages successively. The NC group just performed the first and third stages. The study algorithm is shown in Figure 2.
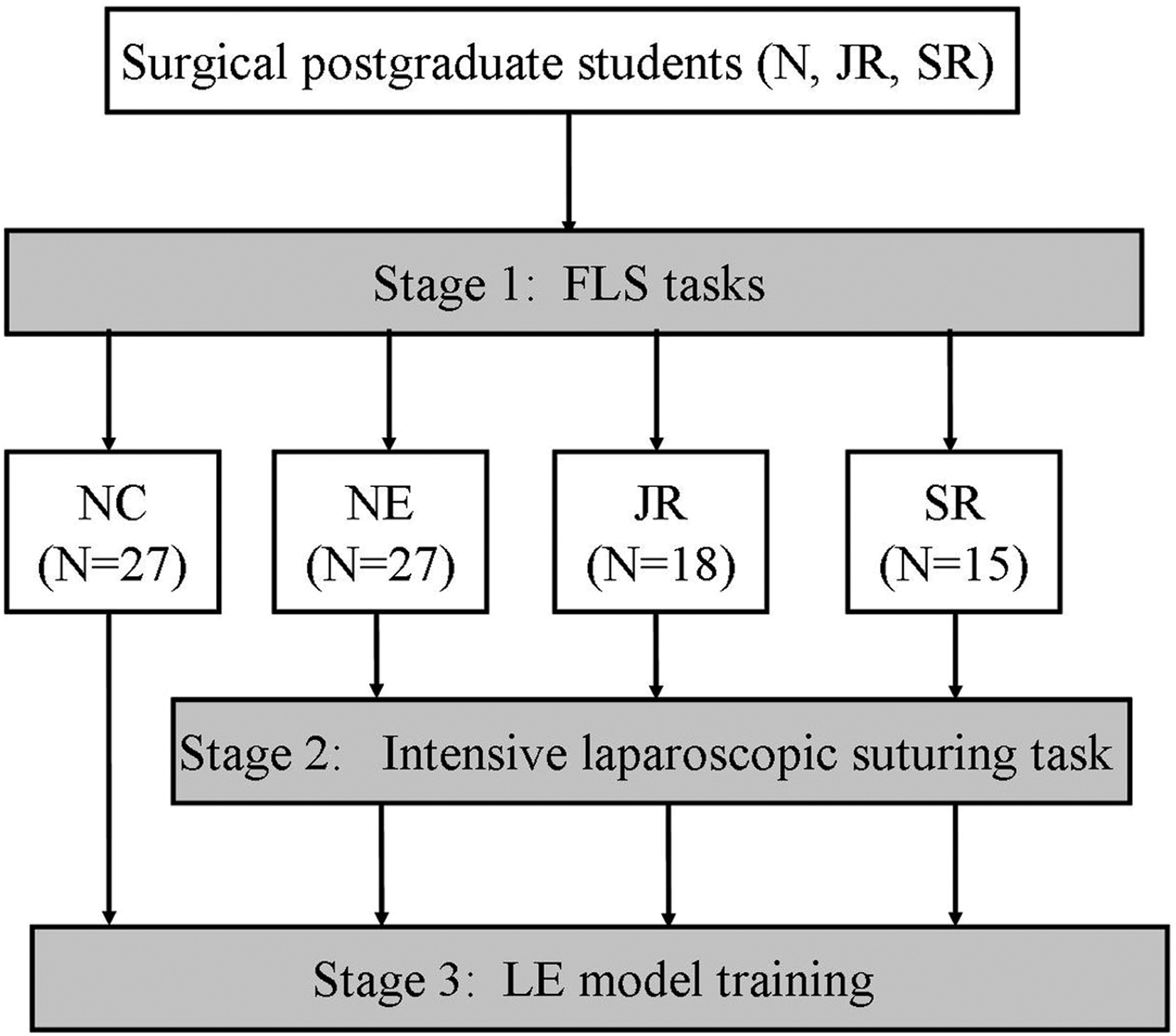
Study algorithm. N=novice; JR=junior; SR=senior; NC=novice control; NE=novice experimental.
The FLS tasks included five inanimate tasks of increasing complexity, as described in detail by Ritter and Scott. 9 Before these tasks, all participants watched a video tutorial of FLS task training, describing the appropriate method for completing the training together with the learning objectives. Each task was assessed using detailed measurements, which are shown in Table 2, and a score was calculated using the formula: Score=cutoff time − completion time − penalty scores. The participants trained until they achieved a passing total score (270) described for FLS examination. Training duration, number of repetitions, and total scores achieved at pretest and post-test were recorded and analyzed.
The intensive laparoscopic suturing task was to place three single interrupted sutures on a length of porcine bowel with an 18-cm length of suture material (Fig. 1). Premarked spots were placed at entry and exit points to ensure the task was standardized in terms of exiting through the incision before taking the second bite. A knot was formed by tying one surgeon's knot followed by two squared half hitches. Errors defined as inaccuracy of suture placement and knot insecurity (a previously validated checklist designed by Dayan and colleagues 10 was used, consisting of 27 items). Performance during training was assessed with objective scores based on time and errors using a modified formula: Score=cutoff time (600)−completion time−5×accuracy error−5×security error. Three experts with known proficiency in laparoscopic suturing performed, and their mean results were used as the performance goal. The participants trained until they achieved an expert-derived proficiency level. Training duration, number of repetitions, and scores achieved at pretest and post-test were recorded and analyzed.
The LE model designed by our center was used to test laparoscopic operative performance. It consists of a metallic box, a fresh porcine heart, a dropping bottle filled with red-dyed water, and a Laparoscope Skill Trainer System. The porcine heart was fixed on the unfolded inner cap of a metallic box. Staples were inserted into the heart muscle as a sign of tumor locations. A spherical enucleation about 2 cm in diameter was performed. Then sutures with a laparoscopic needle holder carrying a 26-mm needle were placed in the bed of resection. The chambers of the heart need an unremitting infusion of red-dyed water during the two steps to duplicate the blood supply in operation (Fig. 3). Each participant completed five exercises during the training period. All the procedures were recorded on videocassettes, which were reviewed and analyzed for total time, sutures time, global performance, and quality of suture repairing. Rating scales for performance and quality error assessing are shown in Tables 3 and 4.

For each item, scoring scale from 0 (best possible score) to 5 (worst possible score).
Total score scale from 0 to 70.
For each item, scoring scale from 0 (best possible score) to 10 (worst possible score).
Total score scale from 0 to 30.
After the training, the participants in NE, JR, and SR groups were requested to complete a questionnaire that consisted of five questions with a five-point Likert-type scale (1=inappropriate and 5=excellent), assessing the intensive laparoscopic training curricula. The questionnaire included the following items: Satisfaction of the training system, satisfaction of each of the three stages, and usefulness of the assessment rating scales. The participant's suggestions for changes were also documented.
Training and testing data expressed as mean±standard deviation (SD) were recorded and analyzed. Statistical analysis was conducted using SPSS version 11.0 (SPSS Inc, Chicago, IL). Analysis of variance and t test were used to compare between-group differences and paired t tests were used for within-group comparisons. Differences were considered significant when a P value was <0.05.
Results
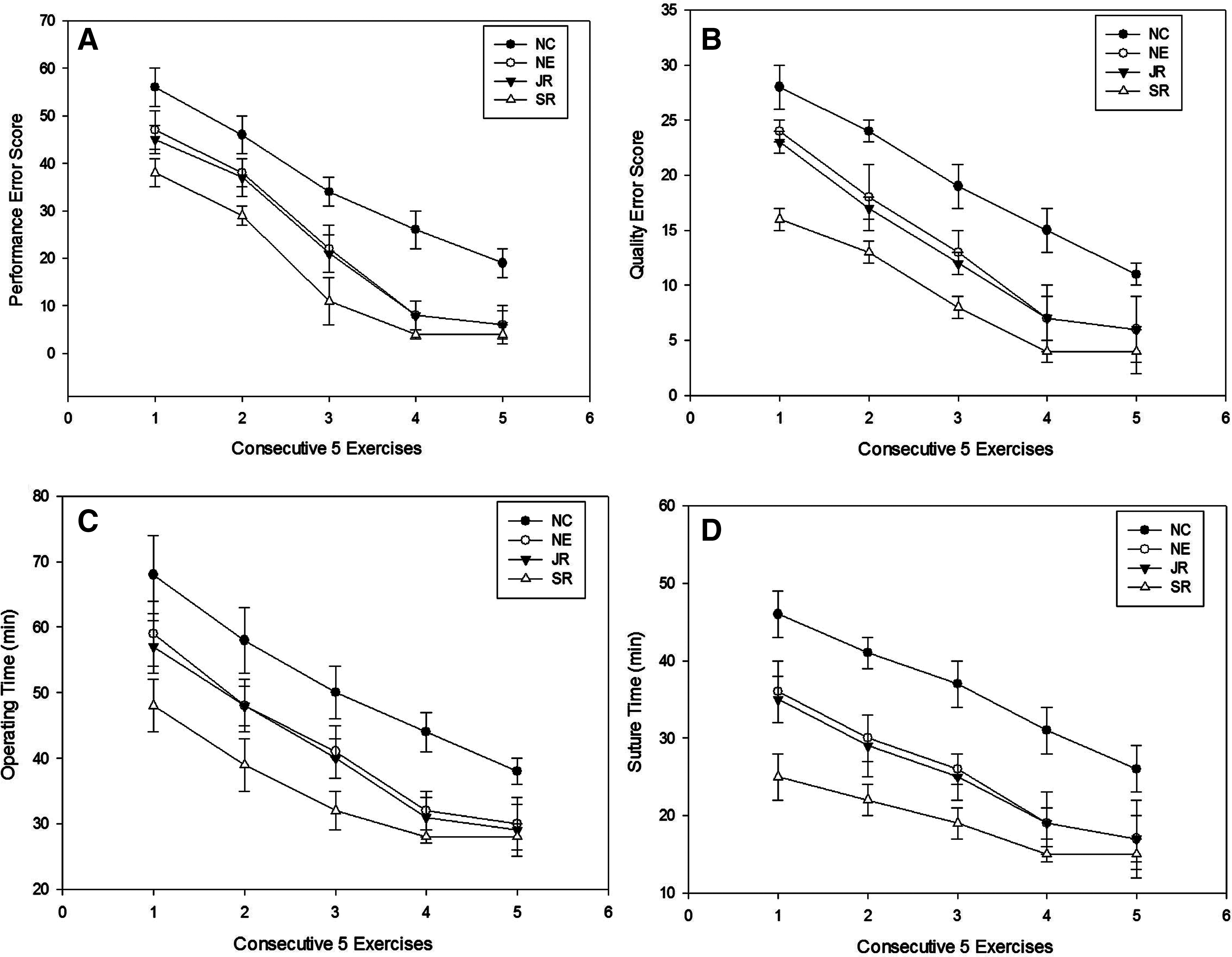
All 87 participants completed this study. The data of time duration and repetitions needed for achievement of proficiency in stage 1 and 2 are summarized in Tables 5 and 6. The mean pretest and post-test scores of each group in stages 1 and 2 are shown in Figures 4 and 5. The training results for the performance of each group in stage 3 are shown in Figure 6.

Mean total pre-test and post-test scores of each group in Stage 1. N=novice; JR=junior; SR=senior.
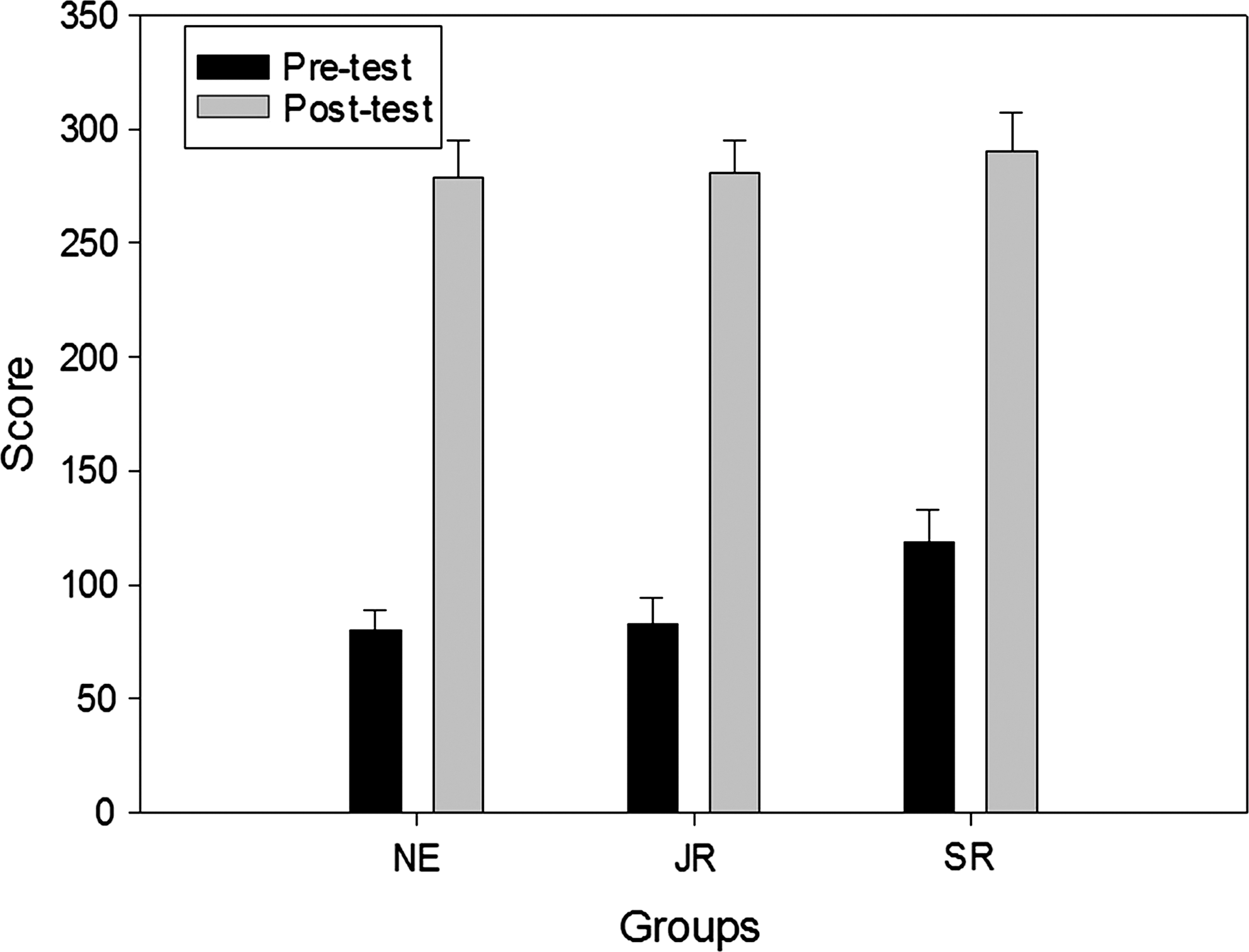
Mean total pre-test and post-test scores of each group in Stage 2. NE=novice experimental; JR=junior; SR=senior.
FLS=Fundamentals of Laparoscopic Surgery; N=novice; JR=junior; SR=senior.
NE=novice experimental; JR=junior; SR=senior.
Regarding the five FLS tasks of stage 1, all the participants showed significant improvements between pretest and post-test total scores (P<0.001) and achieved the predetermined passing level (total score ≥270). Intergroup comparisons showed the SR group significantly better than the N and JR groups in time duration, repetition, pretest and post-test total scores for the five tasks (P<0.05). Compared with the N group, the JR group had better performance in time duration and repetition at the first, second, and third tasks (P<0.001), although not at the fourth and fifth tasks (P>0.05). There was no significant difference in the post-test total scores between the N and JR groups (P>0.05), although the N group had lower pretest total scores (P<0.001).
For the intensive laparoscopic suturing stage, all participants in NE, JR, and SR groups completed the task and achieved proficiency level (score ≥270), although no group demonstrated proficiency before this stage of training. Statistically, improvements occurred between pretest and post-test scores (P<0.001). In reaching proficiency, the NE and JR groups trained longer and performed more repetitions compared with the SR group (P<0.05). No statistically significant difference was found in the post-test scores among the three groups (P>0.05), although the SR group had better pretest scores than the NE and JR groups (P<0.001). Intergroup comparisons showed no statistically significant difference between the NE and JR groups in time duration, repetition, pretest and post-test scores (P>0.05).
The LE model proved robust, and one porcine heart was used for two or three exercises without problems. All participants completed five exercises during the training period. There were significant improvements after five exercises in the four groups. In the NE, JR and SR groups, there was an obvious decrease in operative and suture time over the previous three exercises (P<0.05), whereas the operative and suture time remained at a relatively stable plateau during the later two exercises (P>0.05). Meanwhile, there was a slightly sharper decrease in the mean performance and quality error scores for the former three exercises (P<0.05), and few errors without statistically significant difference were observed during the later two exercises (P>0.05). Intergroup comparisons showed that the NE, JR, and SR groups had better performance than the NC group at the five exercises (P<0.05). There was no statistically significant difference of the four parameters at the fifth exercise among NE, JR and SR groups (P>0.05), although the SR group performed better at the former four exercises compared with the NE and JR groups (P<0.05). Compared with the JR group, the NE group had no statistically significant difference of the four parameters at the five exercises (P>0.05).
The participants in NE, JR, and SR groups returned completed questionnaires after the training. The questionnaires revealed an overall mean score of 21±4. When breaking down the results according to the groups, it appeared that the NE group showed a mean score of 21±4, the JR group 21±3, and the SR group 19±4. These results suggested that the training curriculum was helpful and could improve the laparoscopic skills for postgraduate students, especially in the techniques of suturing and knotting. Moreover, there were good suggestions for changes, including optimizing both the training session and assessment metrics, and improving the realism of the LE model.
Discussion
The traditional training paradigm has been challenged with the introduction of many new and complex procedures into surgical practice, the cost for learning in the operating room, and rising ethical concerns about learning on patients. Moreover, the skills needed to perform laparoscopic surgery are significantly different from those needed for open surgery. 11 Effectively performing laparoscopic surgery necessitates adapting to two-dimensional vision of the operative field, developing video-eye-hand coordination, and becoming accustomed to using long instruments that diminish tactile feedback. Because these abilities need more time for learning compared with open surgery, there has been an increasing trend for systematic training of both basic and advanced laparoscopic skills in a simulated environment.
Published studies have shown transferability of simulator-acquired skill to the operating room. 12,13 Surgeons progress through a learning curve, however, which may vary according to the level of advanced laparoscopic skills, such as intracorporeal suturing. 10 In our study, we emphasize the importance of surgical postgraduate students learning and practicing advanced laparoscopic skills on simulators before going into the operating room to shorten the learning curve and bring maximum benefit for real patients. During this study, the participants who completed the intensive laparoscopic training curricula achieved proficiency of laparoscopic suturing, regardless of baseline laparoscopic experience.
Currently, there are two modalities (physical and virtual reality) that are considered effective in teaching and improving laparoscopic skills. Despite providing a high level of realism, virtual reality simulators are expensive and still require continuous technical support. 14 The cost can be a big obstacle for the incorporation of simulator training, especially for students in many resource restricted countries. 15 A standard physical trainer that is significantly less expensive than a virtual reality simulator may be more suitable for the students in many resource restricted countries. Moreover, the physical simulator training may be more user-friendly for the novice surgeon to begin learning the challenging laparoscopic skills. 16 In this study, simple, inexpensive box simulators were applied for training laparoscopic skills outside the operating room. In addition, the box was made similar to the human abdomen, which can enhance the visual realism. After the training, high satisfaction scores achieved from the questionnaire indicated its efficiency.
One identical goal of many published studies was to identify the best training strategy for the acquisition of laparoscopic skills. Our results have shown that three staged training curricula are feasible for surgical postgraduate students, especially those without experience in laparoscopic techniques, to master laparoscopic suturing. Mastering basic laparoscopic skills first is important for mastering a more complex laparoscopic task and reducing resource requirements for a laparoscopic suturing curriculum. 17 FLS is an educational program that has gained support from the Society of American Gastrointestinal Endoscopic Surgeons, based on the McGill Inanimate System for Training and Evaluation of Laparoscopic Skills (MISTELS) from McGill University. 18 MISTELS is one of the best skill sets currently available, so similar training tasks were chosen in the first stage of the training curricula for basic laparoscopic skills training. All the participants achieved the predetermined passing level, although the SR group performed significantly better than the N and JR trainees at the five tasks.
Unlike basic laparoscopic skills training, laparoscopic suturing should be trained as an isolated skill and needs intensive training. In this study, we optimized both the training task and assessment metrics. The intensive laparoscopic suturing task in stage 2 was to place three simple interrupted sutures on a length of porcine bowel, which increased the training intensity compared with the previous MISTELS. In addition, we applied a more stringent scoring system, which increased error penalties by a factor of five. This modification strengthened the rigorousness and maximized the benefit of training. Trainees are not only capable of learning basic laparoscopic suturing skills but can also achieve good quality knots. The participants successfully achieved an expert derived proficiency level, and there was no statistically significant difference in the post-test scores among the NE, JR, and SR groups, although no group demonstrated proficiency before this stage of training. These results confirmed that successive intensive and rigorous laparoscopic suturing training after the five FLS tasks was efficient. Furthermore, the NE, JR, and SR groups had better performance compared with the NC group in the third stage of training. This result proved that an intensive laparoscopic suturing task before the third stage was indispensable.
The dry laboratory training is not enough for advanced laparoscopic procedures, which is considered advanced because of its complex and potentially life-threatening morbidity. The training curricula should be systematic, progressing from dry to wet laboratory. 19 For this reason, the animal model may be ideal and obviate the need for human testing. Korndorffer and colleagues 8 used a live porcine Nissen fundoplication model to assess transfer of simulator-acquired skill to the operating room. Although the validation evidence is strong for this porcine gastrogastric suturing model, the limiting factors for the use of live animals are ethical considerations and cost. Moreover, hemostasis is another important goal for laparoscopic suturing in many procedures, such as enucleation of the kidney or liver tumors. The gastrogastric suturing model is not suited for the condition of hemorrhage. From our point of view, the gap between wet laboratory training and the animal experiment could be filled by organ perfusion models. These models simulate blood supply of organs ideally. Because of the excellent quality of simulation and cost-effective aspects, the organ perfusion models in laparoscopic training devices serve to simulate difficult intraoperative situations and complications, simultaneously reducing currently required animal experiments. For the sake of explanation of its superiority, the laparoscopic suturing models in urology are summarized in Table 7. The advantages of organ perfusion models stand out even more clearly after comparison.
We designed a LE model using a fresh porcine heart, which offers trainees the opportunities to acquire the skills necessary for LE. During the laparoscopic training, the initial practice of cutting and suturing can be performed on the inanimate porcine heart model under the simulated state of blood circulation, bleeding, and acclivitous position. This LE model belongs to the category of organ perfusion models. Compared with other organ perfusion models, such as the kidney perfusion model, 20 our LE model can provide better blood fluency because of unremitting infusion of red-dyed water into the chambers of the heart. This advantage improved the simulation effect in our laparoscopic training. In our study, we also designed and optimized the performance assessment system, because the training curricula should not only improve operative speed, but also decrease operative errors. Our assessment system maximized the benefit of training while still maintaining efficiency, because the mean time declined and error score decreased significantly after five LE model exercises.
A criticism of training surgical postgraduate students without laparoscopic experience in suturing techniques is wariness of the possibility of some inexperienced trainees attempting inappropriate procedures too early on in their operative career. Superficially, this argument is reasonable in the sense of protecting patients, but it is untenable in the light of benefits of patients and the improvement of surgical skills. Moreover, surgical competence is comprehensive, which can be measured by many characters, such as medical knowledge, decision making, patient care, communication skills, and professionalism, and goes far beyond skills or ability to perform. 7 Our training curriculum is just intended to reduce the learning curve in the operating room rather than providing a license to operate independently.
Laparoscopic suturing skills increased with repetition until a plateau was reached in our training curriculum. The challenge now is to ensure that these students with the newly acquired skills will be given the opportunity to practice and develop their laparoscopic skills in their future studies. A limitation of this study was skill retention for these students after completion of all the training tasks. Future work should be to determine performance retention and optimize the training curriculum as the feedback questionnaires suggest.
Conclusion
This study documented the feasibility of intensive laparoscopic training curricula shortening the learning curve of laparoscopic suturing in surgical postgraduate students, regardless of baseline laparoscopic experience.
Footnotes
Acknowledgment
The authors would like to thank the surgical postgraduate students for their time commitment involved in this study and Navin Shrestha for his support in revising the English language for this manuscript.
Disclosure Statement
No competing financial interests exist.