
Abstract
Background and Purpose:
The metallic ureteral stent was first developed for patients with ureteral obstruction related to malignant disease, but it can be used in all patients needing chronic indwelling ureteral stents, including those with benign disease. The traditional method of polymer stent management often necessitates multiple exchanges per year depending on patient and logistical factors. This has significant direct financial cost and likely a negative effect on patients' overall health. The objective was to analyze and compare the costs associated with chronic indwelling metal and silicone-based ureteral stents.
Patients and Methods
: A prospective database of patients undergoing metal stent placement from February 2008 to June 2010 was reviewed. Mean charges for a single traditional nonmetal and metal stent insertion were calculated. Charges were based on direct hospital charges related to stent cost and surgery. Cost data were based on the fiscal year 2010 cost for polymer or metal stent insertions.
Results:
Twenty-one patients underwent metal stent placement at our institution. Of these, three traditional stent placements were omitted from analysis because of bundled charges for ureteroscopy at the same setting. Mean charges per single traditional and metal stent placement were $6072.75 and $9469.50, respectively. The estimated annual charges for traditional stents (3–6 exchanges) would be $18,218.25 to $36,436.50. Compared with metal stents, this is a potential financial savings of 48% to 74%. The mean direct cost to patients was 21.6% and 25.4% of the charges for metal and polymer stents, respectively. No patient needed early discontinuation of his or her metal stent because of lower urinatry tract symptoms or gross hematuria.
Conclusions:
Metal stents are well tolerated by patients with ureteral obstruction of various etiologies and provide a significant financial benefit compared with polymer ureteral stents. For patients who are not fit for surgical intervention regarding their ureteral occlusive disease, the metal Resonance stent is a financially advantageous and well-tolerated option.
Introduction
There are significant direct financial costs such as hospital-related charges and intangible costs, such as loss of work and productivity. The metallic Resonance (Cook Medical, Bloomington, IN) ureteral stent was first developed for patients with ureteral obstruction related to malignant disease, but it can be used successfully in all patients needing chronic indwelling ureteral stents for malignant or benign disease causing ureteral obstruction. 4 In regard to managing chronic ureteral obstruction, the Resonance stent provides superior long-term drainage when compared with standard polymer stents. 5,6
This metallic ureteral stent is a high tensile strength, MRI compatible, flexible stent. It is composed of a tightly wound metallic coil that resists lumen occlusion significantly more than traditional polymer stents. 4,7 Its composition not only resists occlusion by extrinsic compression, but it also allows for prolonged indwelling times of up to 1 year. 4,7 Given its ability to resist extrinsic obstruction and lengthy indwelling time, it is a viable treatment option for patients with upper urinary tract obstruction who are not fit for surgical reconstruction.
When compared with standard stent options, the metal stent needs fewer annual surgical procedures because of its ability to remain indwelling for up to 12 months. Lopez-Huertas and associates 8 reported a small series of patients whose benign upper tract obstruction was managed with metallic stents and found a 43% reduction in annual direct cost for each patient secondary to fewer stent placements.
We report our experience with the placement of Resonance metallic stents for benign and malignant ureteral obstruction, anecdotal patient experience, and comparative hospital charges to polymer-based ureteral stents.
Patients and Methods
A prospective database of patients who were undergoing metal stent placement from February 2008 to June 2010 was retrospectively reviewed. All metal stents placed were Resonance ureteral stents. All patients were preoperatively evaluated with a history, physical examination, serum creatinine determination, and pertinent imaging that demonstrated chronic unilateral or bilateral ureteral obstruction. Each patient had previously undergone a minimum of one polymer ureteral stent placement with anticipated removal or exchange within 3 to 6 months.
Patients who were not fit for surgical reconstruction were thoroughly counseled on their treatment options for relief of their chronic ureteral obstruction, which included metal or polymer stent placement. Metal ureteral stent placement was only offered to patients who were not fit for surgical reconstruction due to decreased life expectancy from malignancy, advanced age, or significant comorbidities. This included patients with benign etiologies of their upper urinary tract obstruction who had significant comorbidities and/or advanced age with reduced life expectancies. All patients were offered stent placement via a retrograde approach, because no patients in this series had failed this approach previously. Furthermore, metal stents were not offered to patients with ureteral obstruction secondary to urolithiasis or with a life expectancy that was less than 6 months. Patients who tolerated the metal stents and did not experience acute renal failure or adverse events underwent scheduled stent exchanges on an annual basis.
Baseline demographic information for each patient was available, including his or her cause of ureteral obstruction, stent size and length, current status with or without the stent, number of stent exchanges, length of follow-up, complications, premature discontinuations, serum creatinine level, and laterality. A t test was used for comparison of patients' mean pre- and postmetal stent serum creatinine levels. Patients with a metal stent(s) with a planned annual exchange or those who died from their disease with the stent indwelling were considered successes, while stent-related complications or early removal were considered failures.
Mean charges for insertion of a single polymer and metal stent were calculated. Charges were based on direct hospital charges related to stent cost and surgical fees. This included anesthesia, fluoroscopy, pharmaceuticals, and surgeon charges. Annual charges for polymer stents were based on single stent placement charges that were then extrapolated based on stent exchanges made every 3 to 4 months. Metallic stent charges were based on the single annual procedure. The mean cost for patients undergoing metal or polymer stent placement was based on the fiscal year 2010 collection data available for all patients undergoing these procedures.
Results
Between February 2008 and June 2010, 21 consecutive patients underwent metal ureteral stent placement at our institution for chronic ureteral obstruction. All stents were placed via a retrograde approach under general anesthesia. Of these, three traditional stent placements were omitted from analysis because of bundled charges for ureteroscopy at the same setting. Another three patients did not undergo a polymer stent placement at our institution and, therefore, charges made to the patient were not available. Therefore, polymer stent data was available for 15 patients. The number of polymer stent exchanges before metal stent placement ranged from two to six with a mean of three exchanges. One patient's metal stent surgical fee data were not usable because orthopedic and urologic procedure charges were bundled together. Therefore, Resonance metal stent data were available for 20 of the patients.
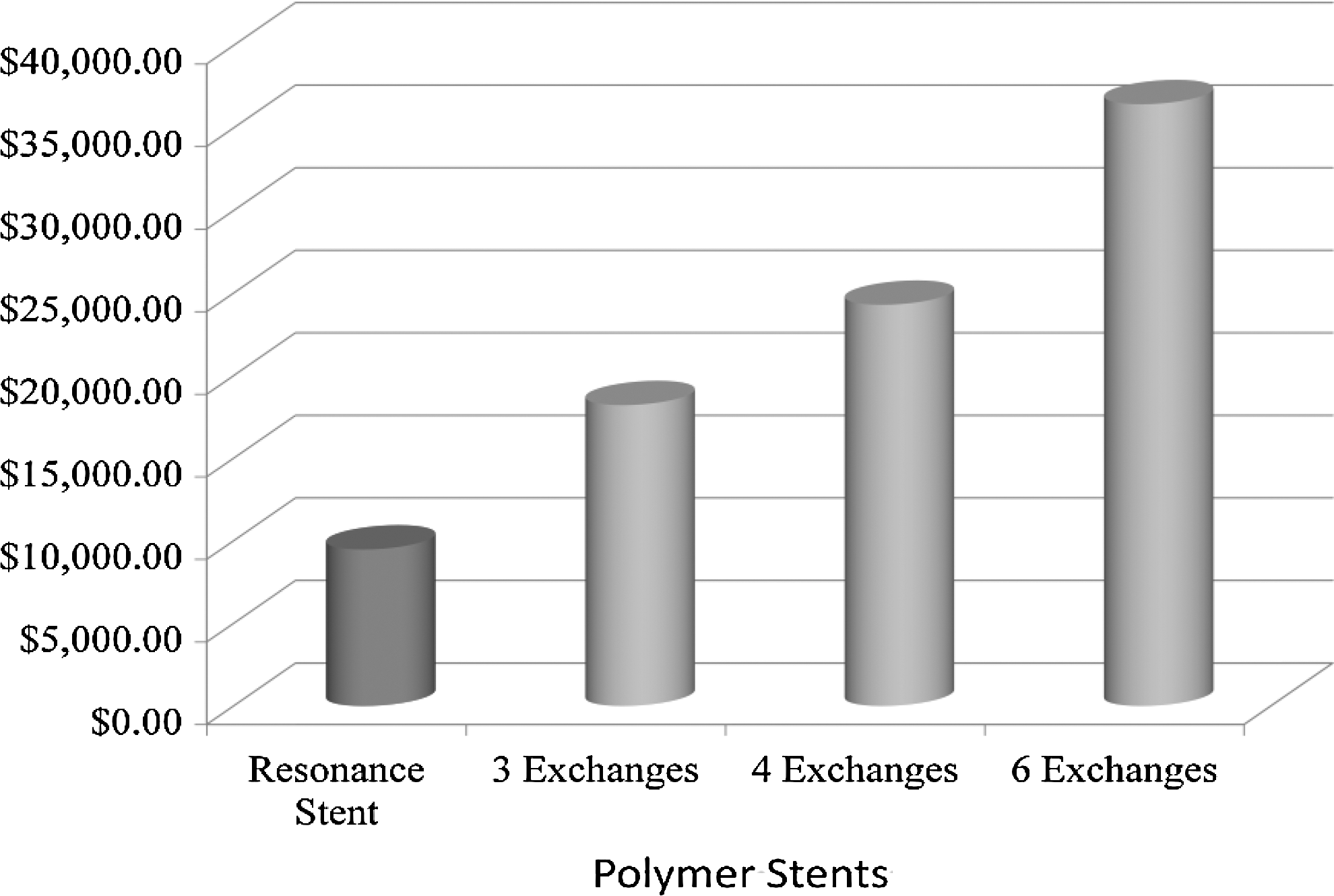
The median charge per single traditional/polymer stent placement was $6072.75, whereas the median charge for a single metal stent placement was $9469.50 (Table 1). The extrapolated annual charges of traditional/polymer stents (3–6 exchanges) would then be roughly $18,000 to $36,000 (Table 2, Fig. 1). Furthermore, based on the fiscal year 2010 collections, the mean cost to patients was 21.6% and 25.4% of the overall charges applied for metallic and polymer stents, respectively.
Annual charges.
Polymer stent bundled charge excluded.
No polymer stent charge data available.
Resonance bundled charge excluded.
The average age of all patients at the time of placement was 70.6 years, ranging from 46 to 87 years. Six patients had right-sided ureteral obstruction, 10 left, and 5 (24%) bilateral. Seven (33%) patients had extrinsic compression from malignancies (metastatic prostate in two patients, and uterine, ovarian, endometrial, multiple myeloma, and colon cancers in one patient). Fourteen patients had ureteral obstruction secondary to benign disease (Table 3). All patients had their metallic stent(s) in place currently awaiting their annual exchange with exception of three. Two patients with malignant ureteral obstruction had a ureteral stent in place for nearly 12 months before succumbing to their respective diseases. The other patient with a metal stent in place had a symptomatic left ureteropelvic junction (UPJ) obstruction and died of other causes with the metal stent in place for nearly 12 months. One patient had left metal stents for a total of 23 months with a single exchange before urothelial carcinoma of the bladder developed; the patient underwent a radical cystectomy.
UPJ=ureteropelvic junction.
Overall, a single patient experienced failure of metallic stenting. This patient had metastatic prostate cancer and shortly after bilateral metal stent placement needed bilateral percutaneous nephrostomy tubes for acute renal failure from malignant obstruction. Overall, seven patients had undergone exchange after 11 to 13 months from initial placement. The median duration with metal ureteral stents was 12 months (2–32 months).
All patients tolerated the metallic stents well, and none needed removal or a shortened indwelling period except the single patient mentioned above. Furthermore, no adverse events were experienced (Table 4). The majority of premetal stent creatinine levels were available in both groups of patients (12 of 14 patients in the benign group and 6 of 7 patients in the malignant group.) The mean premetal stent creatinine level was 1.07 mg/dL (0.4–1.9) and 1.66 mg/dL (0.9-–3.1) for the benign and malignant groups. respectively. Both patient groups experienced a nonstatistically significant increase in their mean creatinine levels (Table 4).
Pre-cr and post-cr=mean serum creatinine levels before and after metal stent placement.
Discussion
Resonance metallic ureteral stents are 6F in diameter and come in a variety of lengths accommodating a wide spectrum of body habitus. They have proven to be a viable option for patients with benign or malignant ureteral obstruction of varying degrees. Although the stent was initially developed for extrinsic malignant compression, we have found it of benefit for varying etiologies of obstruction ranging from UPJ obstruction to metastatic disease.
Within this study's patient population, the metal stent was able to remain indwelling for 12 months without the risk of encrustation or failure from extrinsic compression that we have encountered with polymer stents. For this reason, we typically exchange a polymer stent, even those approved for 12-month indwelling periods, at preplanned 3- to 6-month intervals to avoid complications or early stent failures like those experienced with past patients. These increased frequencies of exchanges are performed in all patients, including those patients without a history of stone formation, to avoid encrustations and other complications necessitating additional and more invasive surgeries. Furthermore, we have not had a single early discontinuation of a metal stent because of bothersome lower urinary tract symptoms, urinary tract infections, gross hematuria, or stent migration (Table 4). Unlike other series, no additional procedures were needed for stent replacement or repositioning because of migration or other adverse events. 9
With a single patient failure as described above, our success rates in this cohort were 95% overall and 86% in the patient group with a malignant etiology of his or her obstruction. This is comparable to other series' success rates of roughly 70% to 95% using metal stent treatment of upper tract obstruction. 10 With follow-up thus far of up to 2 years, we have not encountered some of the complications experienced with other metallic stenting devices. Li and colleagues 11 presented 92 months of follow-up data for the self-expanding metallic stent used in benign causes of ureteral obstruction. Only 9 of 13 achieved patency, with 2 patients needing nephrectomy and 2 needing extraction of the stent because of infection and a hyperplastic epithelialization of the stent leading to obstruction. Others have encountered a stenosis rate of nearly 19% because of epithelial hyperplasia using the metal mesh self-expanding material. 12 We did not experience this hyperplastic process in this cohort of patients and have presented our outcomes concurrently in another article. 13 Furthermore, stent encrustation was not experienced in this patient group, unlike other series with other metallic stenting devices with reported encrustation rates of 3.7% up to 27%. 14 Thus far, there has been a 0% adverse event rate in this patient cohort (Table 4).
Metallic stents are robust stents that resist compressive forces roughly 2.5 to 8 times that of other stents. Furthermore, unlike other stent options, the Resonance stent does not show evidence of permanent deformation after the compressive forces were applied, nor did its ability to resist compressive forces change along its length. 15 Although in-vivo results have shown greater flow rates through standard polymer stents compared with the Resonance stent, the flow rate was adequate to maintain renal drainage and it continued to provide flow after attempted occlusion with 0-silk ties, whereas the standard stent did not. 16 Its ability to resist extrinsic compression is key to its success as a viable surgical option in benign and malignant disease processes that lead to compression/obstruction of ureters. Other stent options do exist with Food and Drug Administration-approved periods of up to 12 months, but we have limited our discussion and analysis to our experience with the metal stent and other metallic stenting devices.
A few limitations of this study do exist, including its retrospective design. Although all patients had a polymer stent in place before the insertion of a metal stent, three patients had initial placement at an outside facility. We were therefore unable to include these polymer stent placements in our analysis. This limited our small sample size. As expected, overall a small number of patients underwent metal stent placement, because the majority of patients presenting with upper tract obstruction of various etiologies are fit for definitive surgical reconstruction. Further limiting our sample size, three patients' charge data for initial stent placement were excluded from analysis because of bundled charges for procedures more complex than simple stent placement. Given the cost benefit readily apparent in using the metallic stent, we thought this would inappropriately skew our charge data benefiting the Resonance stent. For the 15 patients with data available regarding polymer stent changes, an average of 2.5 (range 0–9) stent changes were made before metal stent insertion.
Another potential limitation is the lack of upper tract imaging studies, such as ultrasonography, to evaluate possible changes in hydronephrosis. Overall, many of these patients were elderly and/or had major competing comorbidities, drastically reducing their life expectancies, and their renal function was often tenuous. Therefore, creatinine levels were followed typically by providers outside of our institution. Notably, a single patient did experience acute renal failure, as noted above. Although an overall increase in serum creatinine level from premetal stent to postmetal stent placement was seen, it was not statistically significant (Table 4).
Last, data regarding the use of prestent chemotherapy or radiotherapy in patients with malignant etiologies of their obstruction were not available. This was because of the tertiary referral pattern, with many of these patients receiving such treatments at outside referral sources.
In the current cost-reductive environment in which physicians practice, the metal stent is an appropriate option for patients who need long-term indwelling stents. There is little information available on the financial benefit of these stents. With an estimated annual burden of roughly $18,000, $24,000, and $36,000 based on three, four, or six polymer stent changes, we found a cost reduction of roughly 48%, 61%, and 74% respectively (Table 2). Based on the typical three to four exchanges per year, this is similar to the 43% reduction in annual direct cost for patients found in another sampling of patients with placement of metallic stents. 8 The actual cost to patients or their insurers based on the fiscal year 2010 collection data was 21.6% and 25.4% of the overall charges for metallic and polymer stents, respectively. This slight disparity in actual cost to patients only further widens the gap between the two stent groups supporting metal stent placement.
Conclusions
Metal stents are well tolerated by patients with ureteral obstruction secondary to benign or malignant disease and provide a significant financial benefit compared with polymer ureteral stents. For patients who are not fit for surgical intervention for their ureteral occlusive disease, the metal Resonance stent is a financially advantageous and well tolerated option compared with standard polymer stents.
Footnotes
Disclosure Statement
No competing financial interests exist.