
Abstract
Despite its increasing use in the management of symptomatic benign prostatic hyperplasia, the long-term complications after potassium-titanyl-phosphate photoselective vaporization of the prostate are poorly reported. We describe a rare complication of this technology—calculi formation in the prostatic urethra. All patients presented with visible hematuria and variable lower urinary tract symptoms up to 5 years after the original surgery. In all cases, the calculi were successfully removed endoscopically. Possible causes for this unusual complication are discussed, and the importance of warning patients about this potential long-term complication are highlighted.
Introduction
There has been a paucity of data regarding long-term complications, although bladder neck contractures and necessity for re-treatment are well recognized. We describe an unusual complication of KTP laser photoselective vaporization of the prostate (PVP) that has only been reported rarely in the literature 4,5 —the formation of calculi in the prostatic urethra. We describe four cases of prostatic urethral stones, all symptomatic; the patients presented up to 5 years postoperatively.
Patients
Case 1
A 90-year-old man was referred to our service with painless, macroscopic hematuria and bothersome voiding lower urinary tract symptoms (LUTS) refractory to pharmacotherapy with a selective alpha-blocker (tamsulosin) and 5-alpha-reductase inhibitor (dutasteride). Upper-tract imaging revealed no cause for his hematuria, and flexible cystourethroscopy revealed an occlusive, vascular prostate. He therefore underwent a KTP-laser PVP, in 2005 and his symptoms subsequently improved.
He was rereferred 16 months later with recurrent painless hematuria and plain radiography revealed the presence of small calcifications in the prostatic cavity (Fig. 1). Flexible cystourethroscopy revealed a good prostatic cavity with no bladder-neck contracture, but the presence of numerous small calculi in the prostatic urethra and bladder (Fig. 2).
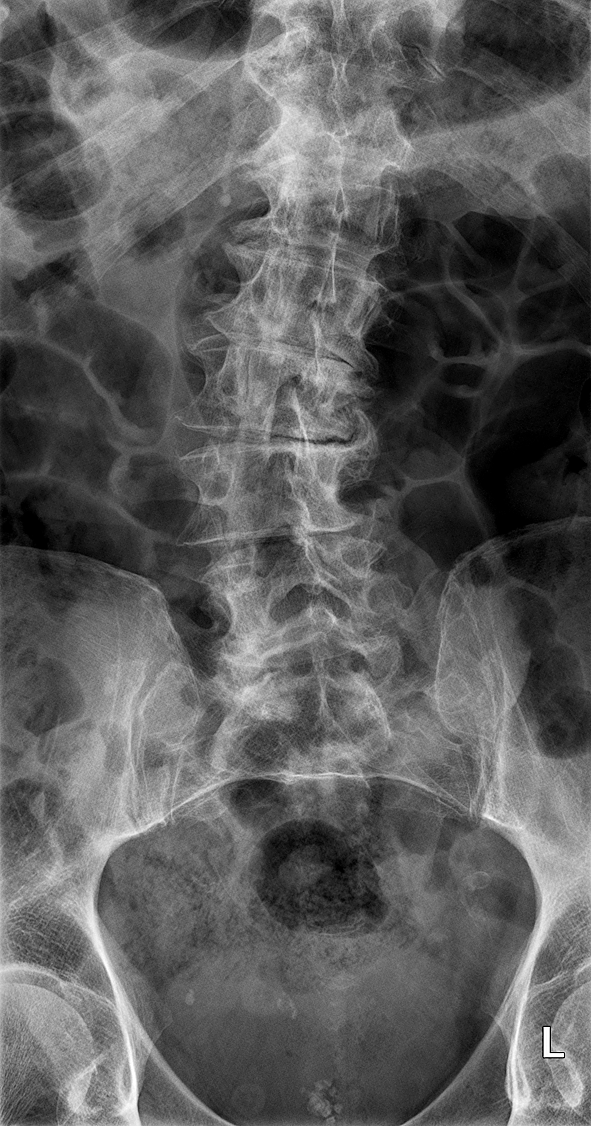
Plain radiography of the kidneys, ureters, and bladder shows the presence of numerous small calculi in the prostatic cavity.

Numerous calculi are seen in the prostatic urethra during cystourethroscopy.
Under general anesthesia, the stones were mechanically pushed into the bladder, fragmented, and removed. His hematuria settled, and he was subsequently discharged without complication.
Case 2
A 74-year-old man was evaluated because of voiding LUTS. His Interntional Prostate Symptom Score (IPSS) score, maximum flow rate (Qmax), and residual urinary volume were 17, 13.3 mL/s, and 59 mL, respectively. He underwent a KTP-laser PVP in 2005, and a postoperative flow test showed an improvement with a Qmax of 30 mL/s.
Five years later he was rereferred to our service with painless, macroscopic hematuria. Renal tract ultrasonography showed no upper-tract abnormality, and flexible cystourethroscopy revealed a good prostatic cavity, no intravesical malignancy, but the presence of a solitary calculus embedded in the prostatic urethra as well as several small calcifications in the bladder.
The stone in the prostatic urethra was embedded so tightly that it was not possible to mechanically dislodge it. Therefore, under general anesthesia, the stones were resected along with some prostatic tissue. His hematuria subsequently improved, and histopathologic analysis confirmed benign prostatic tissue with prostatic calcification (Figs. 3, 4).
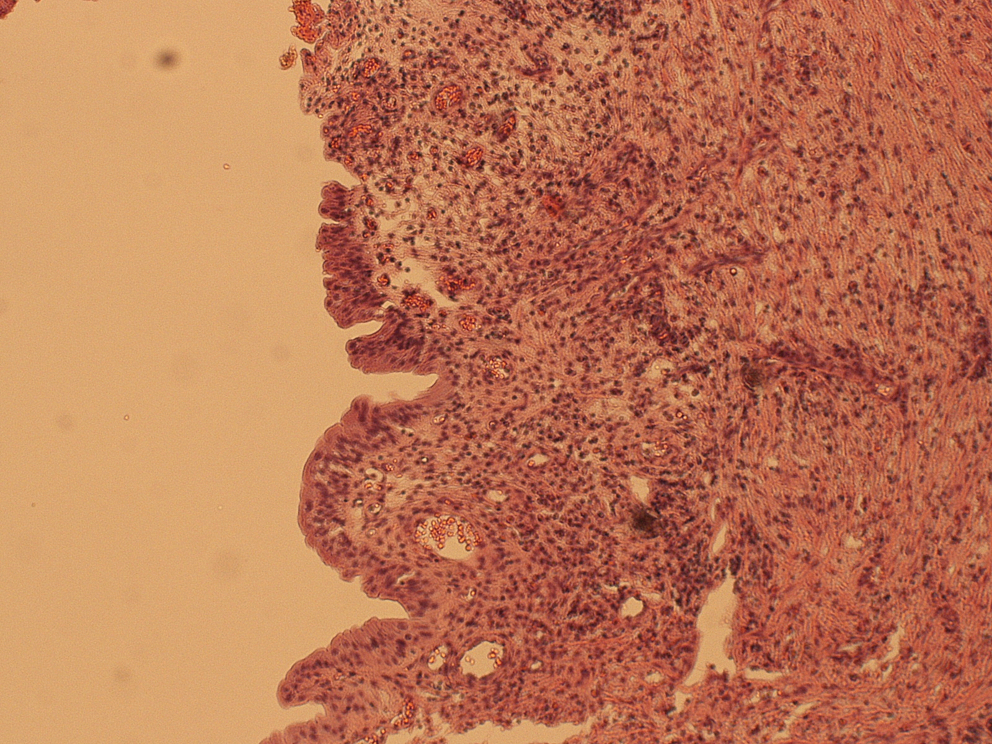
Slide shows reactive prostatic urothelium with underlying mild inflammation.

Slide shows calcification in the prostatic tissue.
Case 3
A 78-year-old man, who had previously undergone monopolar TURP 7 years earlier, underwent a KTP-laser PVP in 2005 for recurrent voiding LUTS. His Qmax improved postoperatively to 19.9 mL/s. Six months later, however, significant storage LUTS developed, mainly frequency and urgency, as well as a urinary tract infection with Escherichia coli. Subsequent flexible cystoscopy revealed a good prostatic cavity with no bladder-neck stenosis. He had a stone in the prostatic urethra, however, and some small calcifications inside the bladder.
The urethral stone was mechanically pushed into the bladder under anesthesia, and all stones were removed and sent for chemical analysis. This revealed a chemical composition of carbonate apatite (70%), magnesium ammonium phosphate (20%), and calcium phosphate (10%). His symptoms subsequently improved, and he was, therefore, discharged.
Case 4
An 83-year-old man underwent a KTP-laser PVP in 2005 for voiding LUTS. Postoperatively, his IPSS improved to 2 with a quality-of-life score of 1 and so he was discharged. He re-presented to our service 33 months later with symptoms of painless, macroscopic hematuria. Upper-tract imaging revealed no cause for his symptoms, and flexible cystourethroscopy again demonstrated a good prostatic cavity with a small calculus at the proximal aspect of the prostatic urethra that was fragmented in the bladder and removed (Fig. 5). Chemical stone analysis revealed a composition of calcium oxalate monohydrate (71%) and calcium oxalate dihydrate (29%).

Prostatic urethral stones after being mechanically pushed into the bladder during cystoscopy.
His symptoms disappeared postoperatively, and he was subsequently discharged.
Discussion
The principal advantage of the KTP laser for the management of symptomatic BPH is its low documented rate of perioperative complications. Trials comparing KTP-laser PVP to the current gold standard, monopolar TURP, have confirmed the superiority of laser PVP in terms of blood loss, time to catheter removal, and length of hospital stay. A prospective nonrandomized study with 2-year follow-up revealed significantly lower rates of intraoperative bleeding (3% vs 11%), blood transfusions (0% vs 5.5%), capsule perforations (0.4% vs 6.3%), and early postoperative clot retention (0.4% vs 3.9%). 6
Despite these impressive short-term complication rates, various long-term complications have been documented. A single-center study with 5-year follow-up revealed bladder neck and urethral stricture rates of 3.6% and 4.4% respectively, with a re-treatment rate of 6.8%. 2 Only 27 of the initial 500 patients, however, were available at 5 year follow-up. Another single-center retrospective study of 246 patients demonstrated an overall re-treatment rate of 8.9% after 5 years, with 1.2% development of bladder neck contractures. 3 Consequently, the National Institute of Health and Clinical Excellence in the United Kingdom does not currently recommend KTP-laser PVP for the surgical management of BPH.
The formation of stones in the prostatic urethra has only been reported rarely as a long-term complication of this procedure, 4,5 and in our series, one patient presented with symptoms as late as 5 years postoperatively. Patients typically presented with recurrent hematuria or storage LUTS many months after the procedure, and stones were found embedded in the prostatic urethra or in the bladder. Symptoms improved almost immediately after removal of these calculi.
As previously suggested, there are a number of etiologic factors involved in the formation of calculi after KTP-laser PVP. 4 Typically, lower urinary tract stones form as a result of urinary stasis that may result from prostatic obstruction or urethral strictures. We did not identify urethral strictures in any of these patients, however, and they all had a good prostatic cavity. The presence of debris or foreign bodies may act as a nidus for stone formation, and this may represent a potential cause of stone formation in this group if the debris is not completely evacuated intraoperatively.
The application of laser energy to the prostate results in one of two possible laser-tissue interactions: Coagulation necrosis (which is more likely to occur if the laser energy is delivered from a distance greater than 0.5 mm from the prostatic tissue), or vaporization (the desired effect). 7 A large amount of coagulation necrosis, which is more likely to occur earlier in the surgeon's learning curve, may lead to the process of dystrophic calcification—calcification occurring in necrotic tissue, commonly as a reaction to tissue damage. It has been demonstrated that the KTP laser induces a wider zone of coagulation necrosis compared with TURP, 8 and it has been suggested that necrosis creates an environment lacking in calcification inhibitors. 9 Furthermore, long-term exposure of this necrotic tissue to infected, alkaline urine may exacerbate the risk of stone formation, and the fact that one of our patients had a carbonate apatite stone supports the role of urinary infection in its pathogenesis.
Other lasers used for the treatment of BPH differ in their absorption characteristics and their depth of tissue penetration. The holmium yttrium-aluminium-garnet (YAG) laser has a penetration depth of only 0.4 mm, and this high-energy density causes vaporization without any deep coagulation. 10 On the other hand, the 1064-nm neodymium:YAG laser and the diode lasers have larger penetration depths of 4 to 18 mm, resulting in deeper zones of coagulative necrosis. 10
All of these factors will result in a higher risk of calcification and, therefore, stone formation. The advantage of the high-power KTP lasers that have recently been developed is the maintenance of vaporization efficiency at distances of up to 3 to 5 mm from the target tissue, thereby minimizing the amount of coagulation necrosis that occurs. We would therefore expect a lower rate of stone formation with the use of these lasers, although whether this is truly the case remains to be seen.
Conclusion
We describe a unique long-term complication of KTP-laser vaporization of the prostate that has only been reported rarely in the literature. Patients may present with symptoms up to 5 years postoperatively, and so the formation of prostatic urethral stones should be considered as a possible cause in this group. With the advent of higher-powered lasers, however, we would expect this complication to remain rare.
Footnotes
Acknowledgments
We are thankful to the urology specialist nurses—Wendy Muir, Carol Davidson, and Ann Chambers—for their assistance in collecting the data.
Disclosure Statement
No competing financial interests exist.