
Abstract
Purpose:
We describe the feasibility of partial arterial clamping (PAC) during robot-assisted partial nephrectomy (RAPN).
Patients and Methods:
We undertook a retrospective study of five patients who underwent PAC vs 17 who underwent complete hilar clamping (CHC). Estimated blood loss (EBL), transfusion rate, operative/console time, warm ischemia time (WIT), pathology, and postoperative glomerular filtration rate (GFR) were compared.
Results:
PAC patients were older (P=0.002) and more likely to have had previous abdominal surgeries (P=0.032). PAC vs CHC was associated with higher median EBL (350 mL vs 75 mL, P=0.026), although there were no differences in blood transfusions (P=0.250). PAC was associated with shorter WIT (14 min vs 21 min, P=0.023). Positive margin rate and GFR change were similar.
Conclusions:
PAC offers a simple and reproducible technique that limits WIT during RAPN. PAC was not associated with more transfusions or positive margins. Further study is warranted to determine the utility of PAC with larger tumor size as well as the long-term benefits on renal function.
Introduction
More than 20 minutes of complete renal arterial clamping leads to diminished renal function. 12 Technical modifications of hilar control and renorrhaphy to reduce or even eliminate WIT have been described. 13 –15 We describe our initial experience with partial arterial clamping (PAC) during RAPN to attenuate WIT while maintaining vascular control to demonstrate that this is a feasible and reproducible technique.
Patients and Methods
Patient enrollment
Between 2006 and 2011, 40 PNs were performed by a single surgeon (JCH). In 2011, we performed RAPN with PAC in five consecutive patients. For comparison purposes, we excluded open and laparoscopic PN, those undergoing PN without hilar clamping, those with unrecorded WIT (n=3), and one RAPN performed for nonfunction in a duplicated system. The final cohorts consisted of 17 RAPN with complete hilar (renal arterial and venous) clamping (CHC) vs 5 with PAC. Data were prospectively collected by research personnel uninvolved with clinical care and entered into a database approved by the Institutional Review Board.
Surgical technique
We performed RAPN consistent with previous descriptions of port placement and technique. 10,14 Monopolar scissor and bipolar Maryland currents are set to 25 W. The tumor is identified using preoperative imaging. Intraoperative ultrasonography is used only for endophytic tumors. The margin of planned resection is landmarked by circumferentially scoring the surrounding renal capsule with monopolar current. Before PAC and tumor resection, the left bipolar Maryland dissector is replaced with ProGrasp™ (Intuitive Surgical, Sunnyvale, CA) forceps. Furosemide and mannitol are administered. A laparoscopic bulldog clamp is applied by the assistant such that approximately 50% or less of the arterial diameter is occluded. The renal vein is left unclamped (Figs. 1 and 2). The tumor is then resected with cold scissors. During excision, there is moderate bleeding, but visualization remains adequate with suction performed by the assistant.
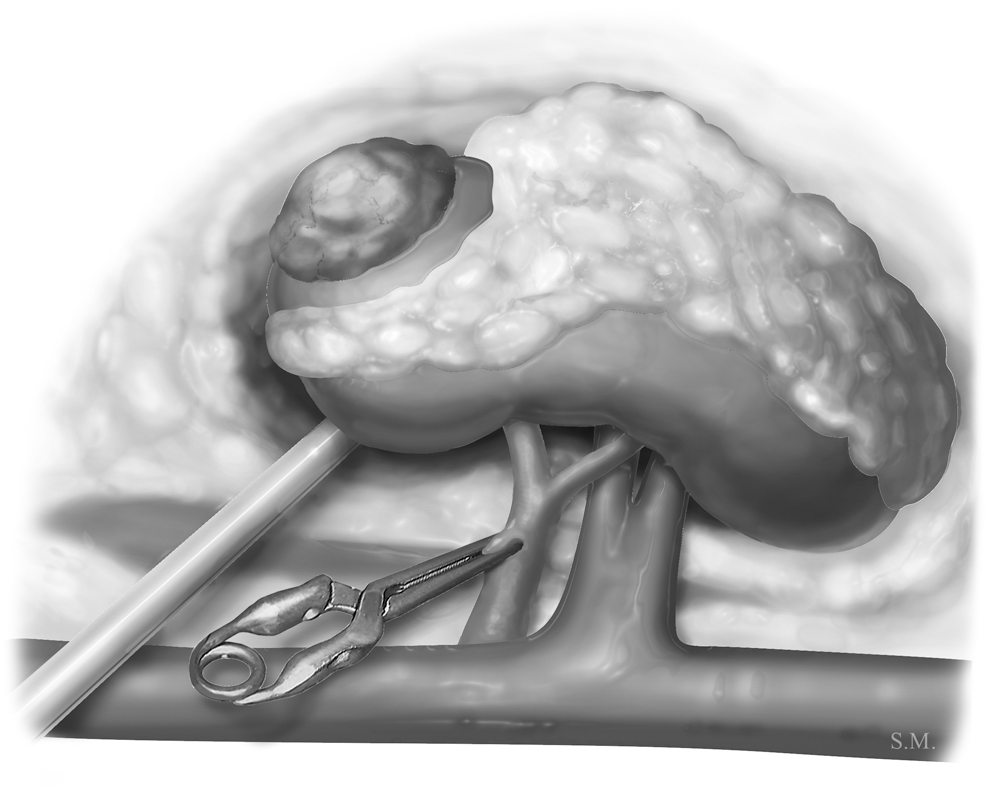
A bulldog clamp is applied to the right renal artery such that only 50% or less of the renal artery diameter is clamped. The assistant suction tip is used to retract the lower pole of the kidney anteriorly.
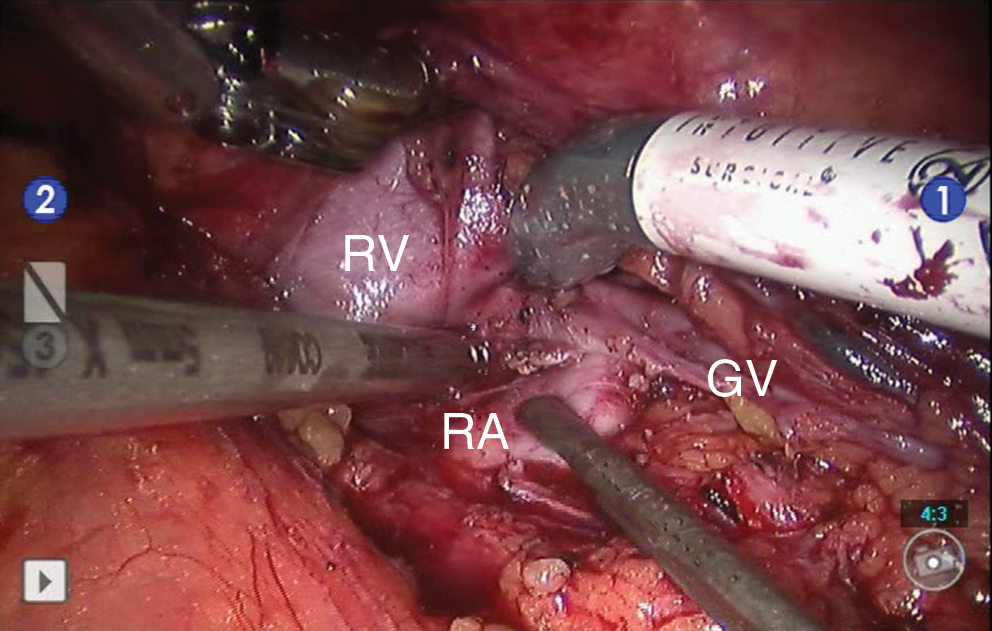
Intraoperative image of partial arterial clamping of the left renal artery.
Two-layer renorrhaphy is performed. First, the base of the renal defect is repaired with a running 3-0 polyglactin suture on a CT-3 needle with a Lapra-Ty® (Ethicon, Cincinatti, OH) applied to the tail. This initial suture is used to ligate bleeding arterioles evident during PAC as well as collecting system defects. A second Lapra-Ty is applied to maintain suture line tension on the base repair. A modification of the sliding-clip renorrhaphy is used 14 for the second layer of the renorrhaphy with a running vs interrupted suture line using 0 polyglactin on a CT-1 needle (Fig. 3). After the corner bite is placed, the laparoscopic bulldog clamp is removed, and the sliding-clip technique is used with each running bite. In the CHC group, we removed the clamp after completion of the sliding-clip renorrhaphy in contrast to earlier unclamping with PAC. We avoid bolsters during renorrhaphy because of concern of resulting potential space after bolster reabsorption contributing to pseudoaneurysm formation.
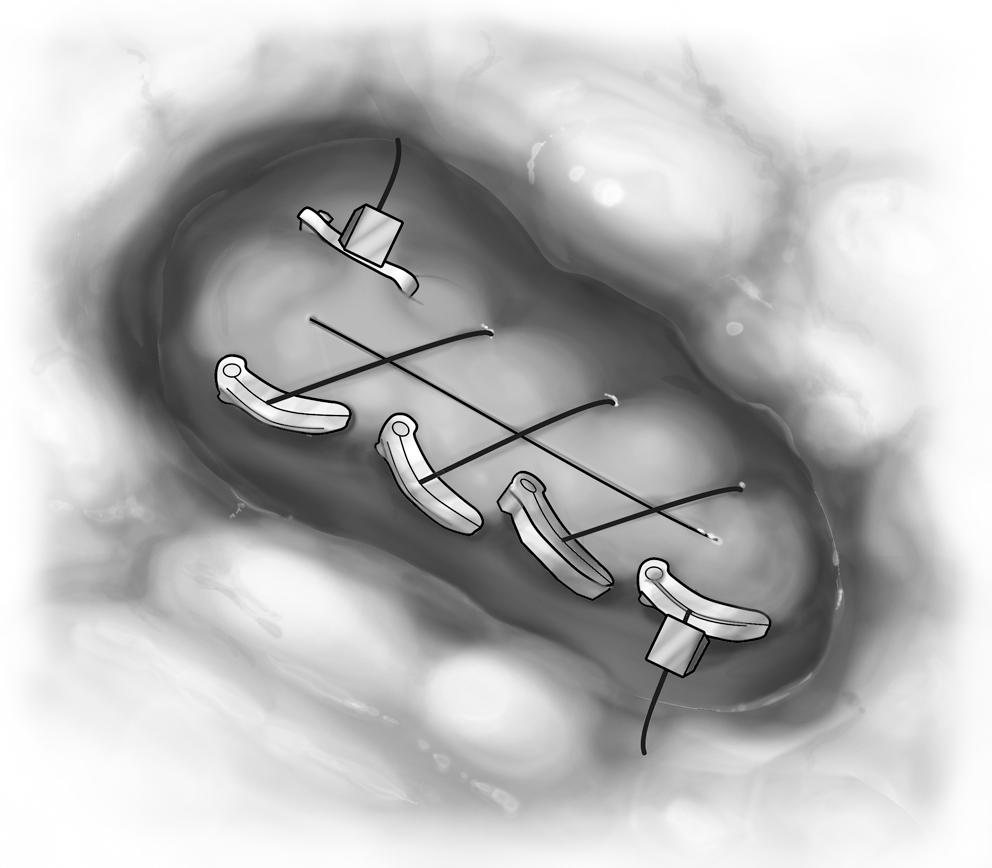
A two layer renorrhaphy is used. The base of the defect is first repaired with a running 3-0 polyglactin suture, encompassing bleeding arterioles as well as collecting system defects. After the first layer of closure, the bulldog clamp is removed. A running sliding clip renorrhaphy is then used.
Outcomes
Perioperative outcomes were prospectively recorded and included estimated blood loss (EBL), blood transfusion, operative and robotic console time, WIT, final pathologic diagnosis, and positive margins. Postoperative glomerular filtration rate (GFR) was measured using the Modification of Diet in Renal Disease equation with the most recent creatinine values and a median follow-up of 15 months.
Statistical analysis
Baseline demographic, perioperative, and pathologic data were compared using the Kruskal-Wallis test for medians and the Fisher exact test for proportions.
Results
Table 1 summarizes preoperative characteristics and intraoperative outcomes. Patients undergoing PAC were older (P=0.002) and more likely to have had previous abdominal surgeries (P=0.032). There were no significant differences in tumor location. PAC vs CHC was associated with significantly higher median EBL (350 mL vs 75 mL, P=0.026), although there were no differences in blood transfusion rate (P=0.250). PAC was associated with shorter clamp times (14 min vs 21 min, P=0.023), attributable to earlier unclamping during renorrhaphy.
Pathologic and renal functional outcomes are summarized in Table 2. There were no significant differences in pathologic outcomes or positive margins. Preoperative and postoperative GFR changes did not differ between the PAC vs CHC cohorts. The potential benefit of PAC, however, was exemplified in the first case of the series, in which preoperative GFR decreased from 64 to 56 on postoperative day 2 after RAPN for a 3.4 cm lower pole mass in a solitary kidney.
GFR=glomerular filtration rate calculated using Modification of Diet in Renal Disease formula.
Discussion
PN confers the benefits of better long-term renal function and overall survival while achieving equivalent oncologic outcomes vs RN. 1,5 Moreover, PN is associated with a lower risk of coronary artery disease, anemia, and bone loss. 6 In addition, even with prolonged WIT, patients undergoing PN vs RN have better postoperative renal function. 16 Therefore, PN by any surgical approach is the preferred approach to renal tumors. 1
Although PN vs RN leads to better renal function regardless of WIT, efforts should be made to minimize WIT and maximize postoperative renal function. 12 Numerous techniques to attenuate or eliminate WIT have been described. Gill and associates 15 described “zero-ischemia” PN whereby segmental arterial branches feeding renal tumors are skeletonized and clamped, and the tumor is excised during a period of induced hypotension. 15 There may be some degree of ischemia to parenchyma surrounding the tumor with systemically reduced arterial pressure, however, and this may be difficult to reproduce outside of tertiary academic centers without consistent and experienced anesthesia colleagues. Moreover, greater surgical skill and risk of arterial injury and bleeding is involved with dissecting out segmental arteries.
A porcine series by Bensalah and colleagues 17 demonstrated the principle of PAC leading to a favorable renal oxygenation profile vs complete arterial clamping, and we set out to demonstrate this in clinical practice. This novel technique of PAC reduces arterial pressure to allow adequate visualization and allow tumor excision, as demonstrated in the referenced video. 18 This may be performed without need for systemic antihypertensive medications, which may carry some risk for those with coronary artery disease. If blood loss increases or visualization is poor during resection or repair with PAC, a second bulldog may be placed across the renal artery. Alternatively, conversion of PAC to CHC with reapplication of one bulldog clamp may be performed. While blood loss was predictably higher in PAC, this did not impede visualization, and there were no positive margins. In addition, transfusion rates did not differ significantly for PAC vs CHC, and the only transfusion was given preemptively after RAPN with PAC in an asymptomatic patient with a history of a five-vessel coronary artery bypass grafting. Although postoperative GFR changes did not vary significantly for PAC vs CHC, our small cases series may be underpowered and has limited follow-up. This technique, however, is relatively straightforward and reproducible outside of tertiary academic centers.
Hemodynamically, PAC reduces the functional diameter of the renal artery while continuing to permit blood flow to the kidney. According to the Bernoulli principle, an increase in the speed of a fluid leads to a corresponding decrease in a fluid's potential energy. In the case of constricted fluid flow, as occurs with PAC, fluid velocity increases with a corresponding decrease in the static pressure of the fluid to comply with the laws of fluid dynamics:
where ρ is the density of the fluid, v 1 is the slower fluid velocity where the artery is wider, and v 2 is the faster fluid velocity where the artery is narrower. This is known as the Venturi effect. 19 In the case of PAC, while blood flow velocity may increase through the renal artery, it is at a lower pressure than if the artery were left unclamped. Physiologically, this drop in renal perfusion pressure may be accompanied by compensatory increased renin secretion from the juxtaglomerular apparatus, thus raising efferent arteriole resistance to maintain GFR. This needs to be studied and quantified in porcine or human models, however.
Our study must be considered in the context of the study design. First, this is a single surgeon case series that presents initial outcomes demonstrating the feasibility of a promising new technique and therefore may be underpowered to demonstrate improved renal functional outcomes. Further study is needed to compare long-term PAC vs CHC renal function. Second, this study was retrospective in nature and subject to the inherent limitations of retrospective data. Third, all tumors were exophytic and less than 3.5 cm in diameter. Further study is warranted for larger, endophytic tumors. PAC, however, supplements the armamentarium for arterial vascular control during PN, particularly for solitary kidneys.
Conclusions
PAC offers a simple and reproducible technique that limits ischemia during RAPN. We encourage its use in patients with preexisting renal insufficiency or with a solitary kidney in which any degree of ischemia may result in significant decline in renal function. Moreover, PAC avoids the greater complexity and risk associated with dissecting out segmental renal arteries or the anesthesia expertise and potential cardiac risks of systemic hypotension. We demonstrate that although there may be greater blood loss with PAC, it was not associated with more transfusions or positive margins. Further study is warranted to determine long-term benefits on postoperative renal function.
Footnotes
Disclosure Statement
No competing financial interests exist.