
Abstract
Purpose:
We aimed to evaluate whether the Hounsfield unit (HU) value predicts outcome in percutaneous nephrolithotomy (PCNL).
Patients and Methods:
One hundred and seventy-nine patients who had undergone PCNL in our clinics in the last 4 years were included. Demographic and clinical data of the patients and complications, if any, were recorded. The mean age of the patients was 45.3±14.3 years (range 5–82 y), and 111 of them were males (62%). The mean stone size and HU values were found to be 693.1±628.0 (95–4200) mm2 and 706.3±245.0 (214–1325), respectively.
Results:
In logistic regression analysis, the size of the stone, the opacity of the stone, and the HU values were found to be independent predictors of the failure of the procedure (P<0.05). A cutoff value of 677.5 was used for the HU in the receiver operating characteristics analysis. Having a HU value under the cutoff value increased the likelihood of procedure failure by 2.65 times, whereas stones residing in the staghorn localization increased failure by 5.68. It was also observed that if the stone's size was 485 mm2 or more, the chance of failure increased by 1.9, whereas when the stone was nonopaque, failure increased by 6.04 times (P<0.05). There was a positive correlation between hematocrit decrease and a decrease in HU values (P<0.05), but no correlation was observed between the HU values and duration of surgery or fluoroscopy (P>0.05).
Conclusion:
In addition to the size and location of the stones, the HU value determined in the unenhanced CT scan may be one of the parameters affecting PCNL outcomes. PCNL is a more efficient method in stones with higher HU values. Therefore, the HU values may be a useful tool for the selection of the treatment modality in patients with renal stones.
Introduction
The success in PCNL is identified by a stone-free rate. These rates are, in turn, affected by factors such as the weight of the stone and its localization. 3 Viewing residual stones via fluoroscopy is largely dependent on the opacity of the stone and its size. 4 It has been reported that the Hounsfield unit (HU) values determined in the unenhanced CT is associated with the visibility of stones on plain radiography and may predict the outcome of shockwave lithotripsy (SWL). 4,5 To the best of our knowledge, there is no study in the literature that evaluates the predictive role of HU value, the indirect indicator of stone opacity in PCNL outcomes.
Our aim in this study was to investigate the relationship between HU values and PCNL outcomes while keeping in mind the fact that visibility in fluoroscopy decreases as the density of the stone decreases.
Patients and Methods
We retrospectively reviewed the records of 286 consecutive patients with renal calculi who had undergone PCNL at our institution between July 2007 and May 2011 after the Institutional Review Board approved the study. One hundred and seventy-nine of these patients were included in the study because they had undergone an unenhanced CT along with other imaging techniques in the radiology department and their data had been retrievable. Preoperative parameters of the patients, including age, sex, localization of the stone, size of the stone, and HU values, were recorded. Parameters related to the surgery, including fluoroscopic imaging duration, decrease in hematocrit, duration of the surgery, residual stone(s), and complications, if any, were documented as well.
All patients were evaluated before the procedure by urinalysis and bacteriologic analysis, whole blood count, serum biochemistry, and coagulation tests. The HU values of every stone were calculated in our hospital by unenhanced CT scan that is used in renal stone protocols (Siemens Somatom Emotion Duo). For calculation of the HU values, PACS Dicom Viewer-V2.7 software was used to digitally view and evaluate the scans. The biggest possible circular diameters were taken into account to record the average HU values. Stone sizes were calculated according to their stone surface area using the guidelines established by the European Association of Urology. 6 Localization of the stones was classified as single calix, renal pelvis, pelvis+single calix, and staghorn. Because there are no objective criteria in the literature used to define stone opacity and keeping in mind the positive correlation between HU values and stone visibility shown on plain radiography as reported in the literature, we classified stones with HU values of less than 350 as nonopaque and those with HU values exceeding 350 as opaque. 4
During the PCNL procedure, 6F open-ended ureteral catheters were placed in all patients in the lithotomy position after administration of general anesthesia to view the anatomy of the collecting system. After this, all patients were brought back to the prone position, and the collecting system was viewed by fluoroscopy with the help of radiocontrast medium. Thus, percutaneous entrance was achieved. Amplatz dilators (Microvasive/Boston Scientific, Natick, MA) were used for the dilation of the tract. For the nephroscopy procedure, 26F nephroscope was used, while a pneumatic lithotriptor (Elmed Vibrolith, Ankara, Turkey) was used for in vivo lithotripsy. Multiple entrances were provided if needed in large and complex stones. Residual stone existence and the intactness of the collecting system were evaluated by fluoroscopic imaging and antegrade nephrostography intraoperatively.
All patients were evaluated in the postoperative third month by intravenous urography, ultrasonography (US), or unenhanced CT scan. The procedure was considered successful if the patient was either stone-free or had only a clinically insignificant residual fragment (residue <4 mm). Stone analysis was carried out by the X–ray diffraction method. Operation duration was calculated as the time it took from inserting the ureteral catheter and bringing the patient to the prone position to inserting the nephrostomy tube. Average hematocrit decrease was calculated taking into account the hemograms that were performed 24 hours before the operation and 36 hours after the operation along with any blood transfusions (each unit of blood given was accepted to increase the hematocrit level by 3%). 7
Statistical analyses were performed using a commercially available software (SPSS version 15.0, Chicago, IL). In addition to frequency and percentage distributions of the data, the Student t test was used in group comparisons, and the chi-square test was used for variables between categorical data. Pearson correlation analysis was used for relationship between proportional variables. By receiver operating characteristics (ROC) analysis, the HU cutoff value, which increases the likelihood of being stone-free, was determined. The odds ratio regarding the variables that increase the residue probability was carried out by logistic regression analysis. P<0.05 was considered to be statistically significant.
Results
The age of the patients was 45.3±14.3 years (range 5–82 y) with 111 (62%) males and 68 (38%) females. One hundred and thirty-eight of the patients (77.1%) were primary patients, and 41 (22.9%) had had previous renal stone surgery. Renal stone characteristics are summarized in Table 1. Success rate was 134 (74.9%) patients altogether, mean operation duration was 92.9±42.3 (35–270) minutes, the duration of fluoroscopy was 4.4±2.7 (0.4–17) minutes, and the fall in hematocrit was observed as 6.4±3.5% (1–19%). Complications were seen in a total of 37 (20%) patients. There was bleeding necessitating transfusion in 18 (10%) patients, fever in 12 (6%), necessity of additional interventions in four (2%), pulmonary side effects in two (1%), and colon perforation in one of the patients (0.5%).
SD=standard deviation; HU=Hounsfield unit.
The data were divided into successful and unsuccessful groups depending on the stone-free status. Data belonging to these groups are given in Table 2. In the multivariable analysis performed to evaluate the factors that affect surgery success, opacity of the stone, localization, HU value, and the size of the stone were found to be factors that were effective. In the ROC analysis, it was found that the area under the curve was significant, and the cutoff value for HU was designated as 677.5 (Fig. 1). A logistic regression model was set up using variables that were found to be of effect in surgical success. In this model, HU values were categorized as higher and lower than 677.5. Being successful or unsuccessful in the logistic regression model is a dependent variable, whereas localization, opacity, categorized HU value, and size of the stone are independent variables. It was seen that the model set up by using the Omnibus test is of significance (P<0.05).
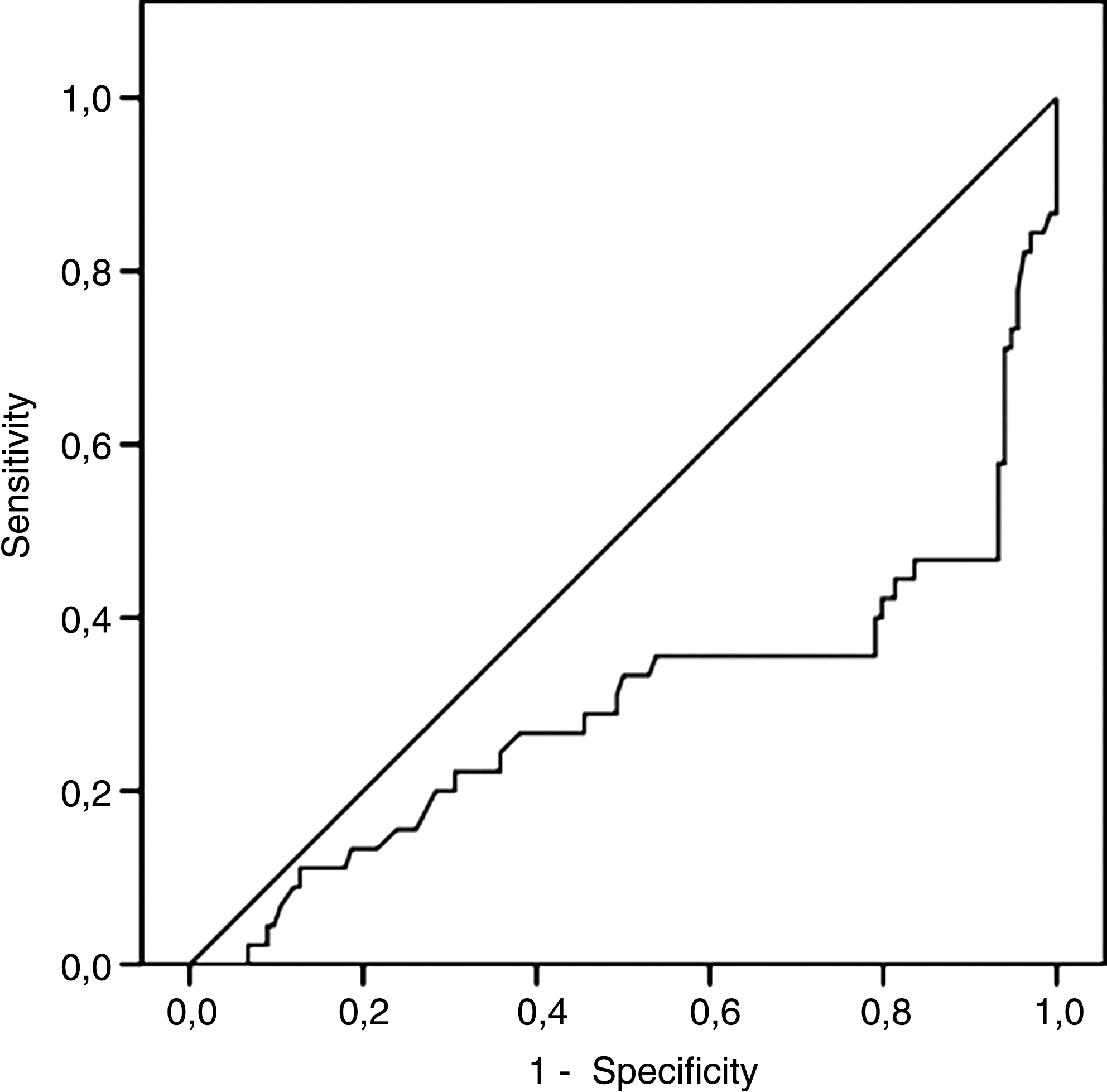
Receiver operating characteristic (ROC) curve shows an area of 0.299 for the Hounsfield unit value and success of outcome after percutaneous nephrolithotomy.
N=number of patients; SD=standard deviation.
In the logistic regression analysis conducted with the same cutoff value of 677.5, it was seen that when the HU value was under the cutoff, the likelihood of residue increased by 2.65. Again, in the same analysis, it was observed that having the stones in staghorn localization increased the residue probability by 5.68, while those with a size of at least 485 mm2 increased this likelihood by 1.9. When the stones were compared according to opacity, being nonopaque turned out to increase the residue risk by 6.04 (P<0.05). Data belonging to logistic regression analysis are shown in Table 3.
OR=odds ratio; HU=Hounsfield unit.
According to the chemical analysis of the stones, it was found that 140 (78.2%) were calcium, 21 (11.7%) were struvite, 17 (9.5%) were uric acid, and 1 (0.6%) was cystine stone. When comparing the success rate according to stone analysis results, it was observed that 117 (84%) patients with calcium stones were treated successfully. This was achieved in eight (38%) patients with struvite and nine (53%) patients with uric acid stones. When the results were compared with the calcium stones in one group and the rest of the stones in another group, there was a statistically significant success rate in favor of the calcium stones (P<0.05). In a total of 24 staghorn stones, success was achieved in 7 of 13 (53.84%) with high HU degrees near cutoff values and in 3 of 11 (27.27%) stones with low HU values.
When the relationship between the HU levels and hematocrit loss was evaluated, it was observed that there was a positive significant correlation between loss of HU value and hematocrit decrease (P<0.05). HU values did not correlate with either duration of the operation or duration of the fluoroscopy (P>0.05).
Discussion
In the present study, we retrospectively analyzed the predictive role of HU values determined in unenhanced CT scans in the success rate of PCNL. To our knowledge, we demonstrate for the first time in the literature that an HU value lower than 677.5 is one of the most prominent factors predicting failure of the PCNL procedure. Confirmation of our findings in larger, prospective studies may serve a useful tool for the selection of treatment modalities in patients with renal stones.
Fluoroscopic imaging is widely used in PCNL to provide an entrance to the collecting system as well as to identify the whereabouts of residual stones. 2 Stones with weak opacity on plain radiography are hard to spot in fluoroscopic imaging. If the opaque agent that is administered to the collecting system partially oozes out during dilation, it can be impossible to spot with fluoroscopic imaging.
A successful PCNL necessitates appropriate preoperative planning and an optimal percutaneous intervention. Therefore, CT has become an important imaging method in the planning of standard pre-PCNL intervention, insertion of the guidewire, and planning of the latter stages. 8 Gedik and associates 9 in a study concerning PCNL in pediatric patients documented that routine CT before PCNL is a must for identifying retrorenal colon and for providing the most convenient access. Moreover, higher success rates have been reported when planning access by CT. 10 Another contribution of CT imaging that is suggested by the aforementioned reasons is that the HU level, which is an objective and numerical indicator of stone opacity, can be calculated.
Huang and colleagues 4 have suggested that the ureteral stone visibility on plain radiography could be foreseen according to their characteristics in unenhanced CT. When the density of the stones exceeded 800 in HU standards, all ureteral stones could be seen, whereas only 26% of the stones could be seen on plain radiography when the HU level was less than 200. It was documented in in vitro studies that the HU value of the stone viewed in unenhanced CT scans can predict the fragility of the stone via SWL. 11 Pareek and coworkers 5 have reported in their clinical studies that HU values can predict the stone-free rate after SWL and that stones with lower HU values have higher success rates. HU values can be one of the parameters that predict PCNL outcomes. To the best of our knowledge, we provide the first data correlating HU value and the success rate of PCNL.
It has been shown in several studies that the success rate in PCNL is affected by the stone burden and the localization of the stones. 3 In the present study, one of the most important parameters that had an effect on the success rate was the localization of the stones. In our search for a new parameter that could alter the success rates, an HU value of 677.5 HU was found to be the cutoff value in our ROC analysis because it increased the risk of a residual stone (or stones). The fact that the area under the curve has been determined as 0.299 leads us to think that the cutoff value should be confirmed by more detailed studies. Nevertheless, when this is accepted as the cutoff value in cases with HU values less than 677.5, residual stone risk has increased by 2.65. It was observed that when the stone was nonopaque, this risk increased by 6.04 times. The authors think that this increase in residual stones is dependent on the fact that residual stones cannot be viewed by fluoroscopic imaging.
Intraoperative US might be an alternative option for these patients. It has been pointed out in several studies, however, that stones with lesser density are harder to see on US than stones with a higher density. 12 For these reasons, in patients with renal stones having lower HU values, fluoroscopic imaging alone is not adequate, and flexible nephroscopy should be used, if possible, to minimize the residue rates. It should be kept in mind that in these stone groups, after PCNL there is more need for SWL therapy for residual stones, and it can be used as a more effective strategy.
In their study on the role of CT in determining stone composition, Deveci and colleagues 13 pointed out that struvite and uric acid stones have lower HU values than other types of stones. Motley and associates 14 observed a positive correlation between stone size and radiodensity and reported higher HU values in bigger stones regardless of the composition of the stone. In our study, the lowest HU values, in increasing order, belonged to cystine, uric acid, and struvite stones. Except for cystine stones, these stones with low HU values are easily broken and shattered into pieces, and, when shattered, it is harder for these stones to be picked up completely. Moreover, these stones with weak opacity are even harder to view under fluoroscopy when they are diminished in size as well. Using a combined or ultrasonic lithotriptor in this stone group may be of additional help.
When evaluated according to stone analysis results, the success rate in the calcium stone group with average HU values of 749 was significantly high at 84%. The success rate was higher in struvite stones compared with uric acid stones (53% vs 38%). When viewed from the HU value perspective, the success rates of struvite and uric acid stones can be seen as a dilemma. When size and location effects are not taken into account, however, there were no significant differences between the two groups. Kacker and coworkers 15 reported decreased stone-free rate after PCNL in their studies with calcium phosphate-rich renal stones. The authors think that detailed data in PCNL therapy involving comparisons between stones with different compositions is needed.
Another important finding of our study was the positive correlation between HU values and hematocrit decrease. There is more bleeding as HU values increase, which can possibly be explained by the fact that stones with higher HU values are harder to break and require more energy during this process. Hence, there is more trauma. Another probable explanation is that the trauma occurred during the search for these stones. These can be easier to spot in fluoroscopic imaging.
Our study has several limitations. First, it has a retrospective design. Second, the patient number is relatively small, and all patients undergoing PCNL during the study period could not be included, because of missing data. Finally, as it is the first study of its kind, there were no other studies available for comparison. For these reasons, our findings should be supported by additional prospective studies with a large number of patients.
Conclusions
In addition to the size and location of the stones, the HU value determined in the unenhanced CT scan may be one of the parameters affecting PCNL outcomes. The SWL technique yields better results in stones with lower HU values, whereas PCNL is a more efficient method in stones with higher HU values. Therefore, the HU values may be a useful tool for the selection of the treatment modality in patients with renal stones.
Footnotes
Disclosure Statement
No competing financial interests exist.