
Abstract
Purpose:
To report the development of panurethral stricture disease and other lower urinary tract abnormalities as a complication of photovaporization of the prostate (PVP).
Patients and Methods:
We evaluated three patients who were referred for the treatment of urethral stricture disease after PVP. Evaluation included antegrade cystoscopy, urethroscopy, retrograde urethrography, and cystourethrography.
Results:
All three patients had panurethral stricture disease, and a low capacity bladder with bilateral vesicoureteral reflux had developed in one patient as a complication of PVP.
Conclusions:
Although not previously reported, a potential complication of PVP is devastating panurethral stricture disease.
Introduction
GreenLight™ laser photoselective vaporization of the prostate (GreenLight PVP), first described for LUTS by Watson in 1995, 3 –5 uses a potassium-titanyl-phosphate (KTP) laser to vaporize prostatic adenoma with similar functional outcomes and less morbidity when compared with traditional TURP. 6,7 KTP uses a visual spectrum wavelength that does not heat tissue like early generation lasers, which used infrared energy. KTP is transmitted freely through aqueous tissue medium but is readily absorbed by intracellular oxyhemoglobin, which is highly expressed in prostatic tissue. Thus, the technology allows highly specific vaporization and spares surrounding tissue. 8 GreenLight laser systems include an 80 W photovaporization system, a 120 W High Performance System, and a 180 W Xcelerated Performance System with a liquid cooled fiber.
Physiologic saline can be used as an irrigant during PVP as opposed to the hypertonic solutions (glycine, mannitol or glucose) 9,10 needed for TURP. Saline irrigant allows longer operative time, decreased incidence of transurethral resection syndrome, and permits faster recovery. 5,8 Finally, patients who undergo PVP can continue anticoagulant therapy before surgery. 11 Since the adoption of KTP laser technology in the late 1990s, more than 500,000 procedures have been conducted worldwide with an associated decline in traditional TURP. 5,12 Thus, the urologic community has embraced GreenLight PVP as a treatment option for the surgical management of LUTS. 12
Urethral strictures and bladder neck contractures are uncommon but known complications for both TURP 3,13 and PVP, 6,14 with an incidence of approximately 1% to 4% across all reported series. 4,15 –17 These contractures are limited to a specific portion of the urethra, such as the fossa navicularis, and are highly amenable to effective treatment. Panurethral stricture, a devastating morbidity, has not yet been reported in the literature after initial uncomplicated TURP or PVP. We report three cases of grade IVa complications of anterior panurethral and posterior stricture after uncomplicated PVP for LUTS.
Case Reports
Case 1
A 54-year-old man with a history of diabetes and LUTS underwent microwave thermotherapy for LUTS. He experienced temporary symptomatic improvement, and then increased symptoms developed that did not respond to dutasteride and tamsulosin. His prostate-specific antigen (PSA) level was 0.5 ng/mL. Two years after his microwave thermotherapy, he was treated with GreenLight PVP for recurrent LUTS despite receiving dutasteride and tamsulosin. On cystoscopy, the patient had a 2-cm lateral lobe prostatic occlusion and mild bladder trabeculation, but no urethral abnormalities. PVP was performed with a 26F rigid cystoscope and a laser fiber at 80, 100, then 120 W to open the prostatic urethra. The distal boundary of the surgery was the verumontanum.
Three days after the catheter was removed, severe penile and scrotal edema and retention developed, and a catheter was placed. The patient subsequently was treated with antibiotics for urethritis and passed a voiding trial, but continued to have obstructive and irritative symptoms. He was noted to have distal urethral stricture disease, which was managed with dilation. Three months after the PVP, he underwent dilation with sounds to 28F and TURP.
Subsequent to catheter removal, retention developed, and the patient could not be catheterized; a suprapubic tube was placed. He then underwent filiform and follower urethral dilation, and the suprapubic tube was then removed. No urethral imaging was performed before treatment. The patient was then advised to continue to urinate with obstructive symptoms and not pursue further treatment unless complete retention developed.
He continued to remain symptomatic for an additional year; he then obtained a second opinion and was referred. The distal urethra calibrated to 9F with bougie-à-boule, and retrograde urethrography confirmed a >20 cm pananterior urethral stricture extending into the departure of the anterior urethra with narrow caliber change (Fig 1). There was irregularity of the contour of the membranous urethra. The bladder was then filled in retrograde fashion so that voiding cystourethrography could be performed, because this is the best imaging test to evaluate the posterior urethra.
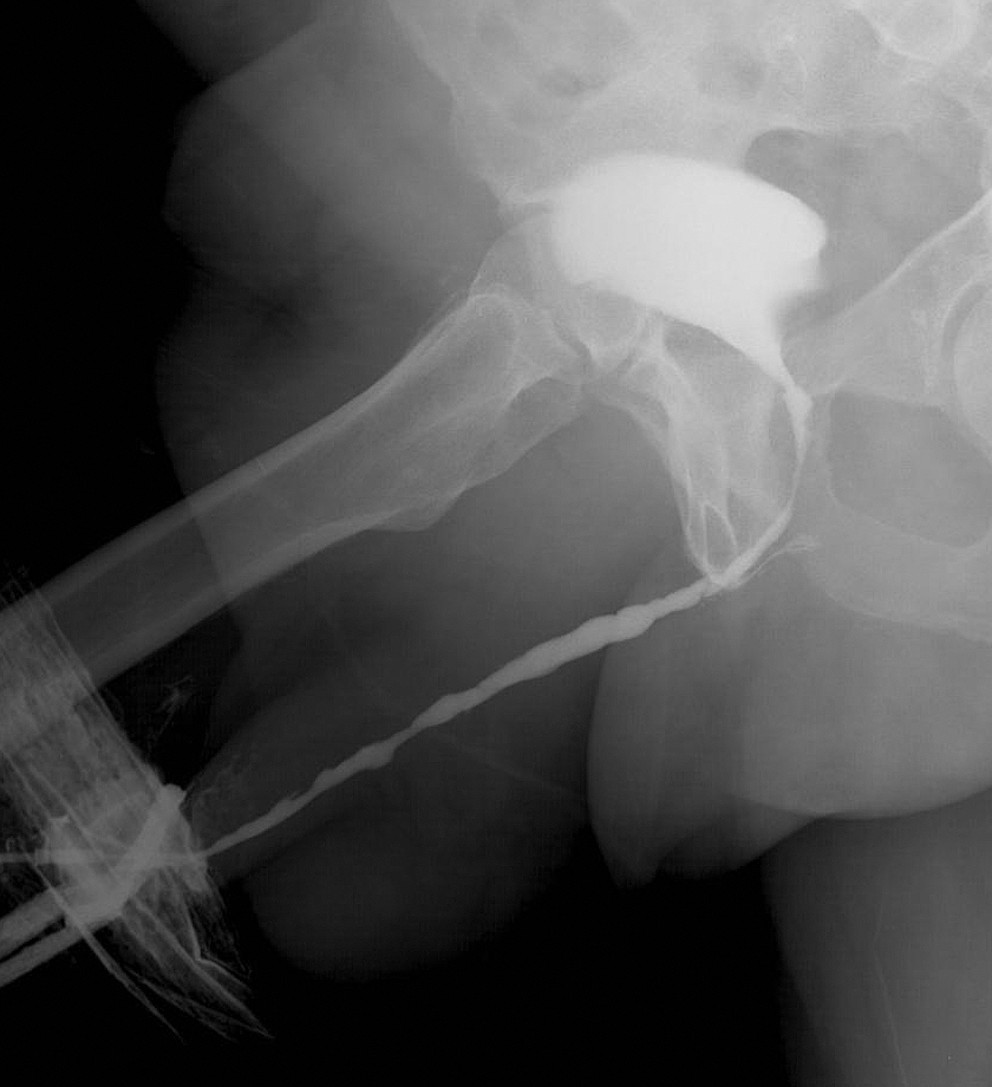
Case 1: Cystourethrogram and retrograde urethrogram demonstrated panurethral stricture extending >20 cm from the penile to the bulbar urethra, with membranous involvement and urinary bladder neck contracture.
The patient could not void at the time of the study, however. Therefore, a suprapubic tube was placed, and after the tract was mature, antegrade cystoscopy was performed. This study confirmed a bladder neck contracture. Given the fact that the disease involved the entire anterior urethra, the posterior urethra, and bladder neck, the patient elected to undergo a formal urinary diversion.
Case 2
A 67-year-old man presented with LUTS. Results of the rectal examination were benign, and the PSA level was 2.3 ng/mL. He was treated with terazosin and finasteride for 6 months but did not have adequate symptomatic relief. Cystoscopy revealed marked lateral lobe hypertrophy and mild middle prostatic lobe enlargement, but there was no indication of urethral stricture disease. His peak flow was 8 mL/s with a postvoid residual of 120 mL. He underwent PVP with a GreenLight laser advanced through a 23F ACMI cystoscope and a near-contact 80 W technique. Electrovaporization with a VaporTrode® was then used with 104 kJ to remove additional tissue because of the large size of the prostate. A urethral catheter was placed at the conclusion of the procedure.
On postoperative day 1, penile discomfort developed, and the patient failed a voiding trial; a catheter was replaced. After 4 days, the patient was still unable to void and was noted to have a capacity of only 120 mL. Cystoscopy revealed stricture disease and diffuse inflammation in the absence of infection. The patient received steroids as treatment for a possible latex allergy and underwent periodic distal urethral dilation. Three weeks after surgery, cystoscopy revealed a distal stricture that was dilated to allow scope advancement into the bladder, and a diffuse inflammatory process was again noted.
The patient was then referred for evaluation and management. Bougie-à-boule urethral calibration indicated a 14F fossa, despite recent dilation, and urethroscopy with a pediatric rigid cystoscope indicated whitish discoloration of the anterior urethra. The patient then underwent suprapubic tube placement. During routine changes, the patient was noted to have a low tolerance to bladder filling despite treatment with anticholinergic medication.
After 3 months of urethral rest, the patient returned for a urethral evaluation. The urethral meatus calibrated to less than 10F with bougie-à-boule, and retrograde urethrography revealed diffuse penile and distal bulbar urethral narrowing and irregularity and an obliteration beginning at the level of the midbulbar urethra. There was significant venous extravasation despite gentle injection, and this was likely related to inflammation of the mucosa despite previous urethral rest as opposed to aggressive injection technique. Simultaneous antegrade and retrograde imaging was then performed in the operating room (Fig. 2). Extravasation was again noted along with a severely contracted bladder and bilateral reflux. The patient ultimately needed a bladder augmentation and urinary diversion.
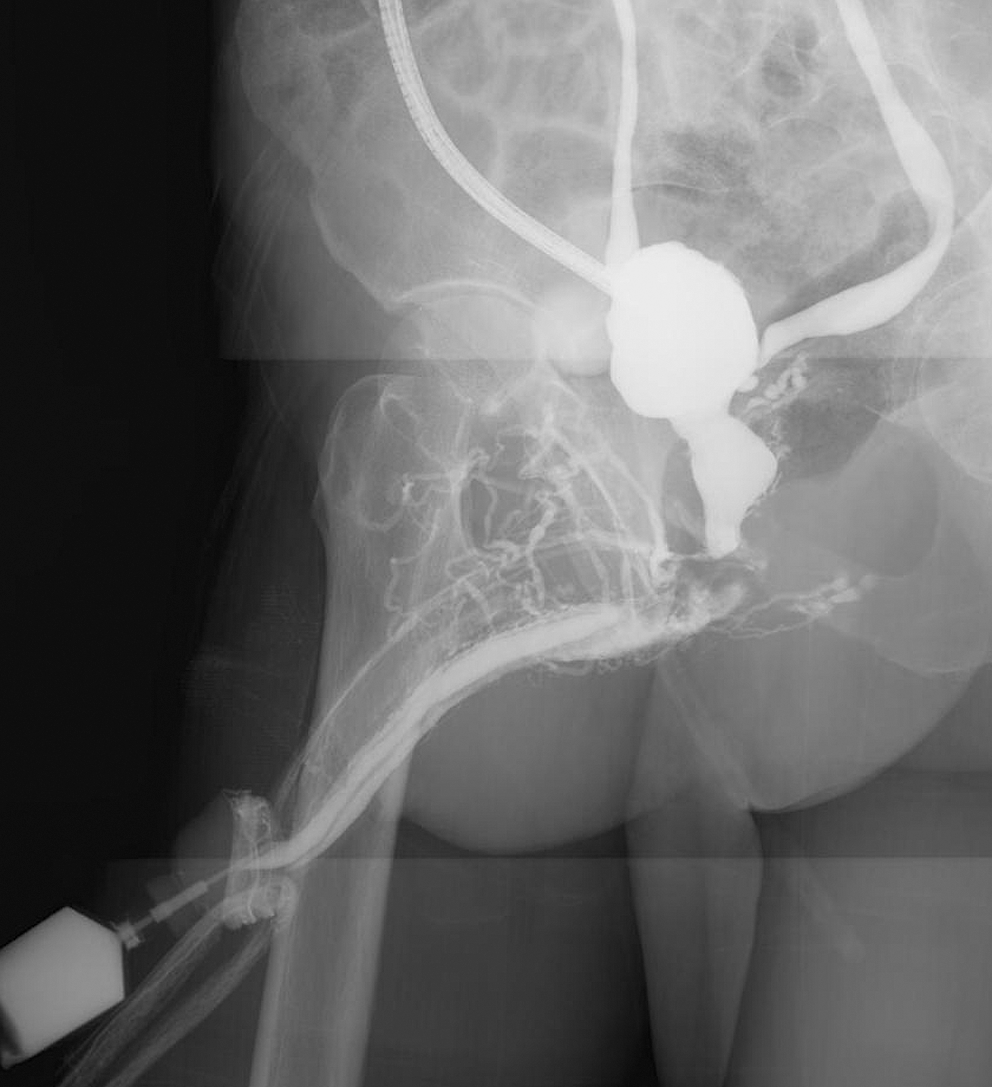
Case 2: Cystourethrogram and retrograde urethrogram reveal diffuse penile and distal bulbar urethral narrowing, irregularity, and an obliteration beginning at the level of the midbulbar urethra, venous extravasation, a contracted bladder, and bilateral vesicoureteral reflux.
Case 3
A 57-year-old man with a history of LUTS that was refractory to medical management underwent GreenLight PVP. Cystoscopy at the time did not reveal any urethral stricture disease, and the PSA level was <0.5 ng/mL. Within days postoperatively, progressive voiding symptoms leading to retention developed, and a suprapubic tube was placed. Repeated cystoscopy revealed significant urethral stricture disease, and the patient was referred for treatment. He then underwent antegrade and retrograde urethral imaging and cystoscopy in the operating room. Cystoscopy demonstrated a very narrow caliber stricture of the fossa navicularis, palpable fibrosis with accompanying impassable stricture at the level of the midanterior urethra, and complete obliteration of the membranous urethra. Given the extent of stricture disease, the patient was not a candidate for surgical repair. He was advised of options, including formal urinary diversion and elected to continue with the suprapubic tube at that time.
Discussion
Panurethral stricture after PVP for BPH has not yet been described in the literature. We report three cases of panurethral stricture in men who presented for routine surgical management of LUTS with no record of previous urethral disease and no stricture visualized as the scope was advanced before photovaporization (Table 1). No specific cause could be determined, nor were consistent comorbidities or patient histories identified.
PSA=prostate-specific antigen; PVR=postvoid residual; LUTS=lower urinary tract symptoms; UTI=urinary tract infection; STD=sexually transmitted disease; NKDA=no known drug allergies; DM=diabetes mellitus; HTN=hypertension.
Urethral manipulation other than GreenLight was considered as a possible etiology. The Case 1 patient underwent microwave therapy years before PVP without subsequent evidence of urethral disease on cystoscopy. In Case 2, Vapotrode was used for a brief interval to remove residual tissue at the time of GreenLight PVP. Although it is difficult to isolate the cause of stricture between these two modalities, intraoperative duration of electrovaporization was significantly shorter than that of GreenLight PVP and certainly not extensive enough to damage the urethra or surrounding vasculature.
In both cases, the initial intervention may have left the tissue vulnerable, rendering it more prone to inflammatory or necrotic damage. The effects of vaporizing modalities may have been synergistic, as each technology uses different means to introduce energy into the tissue. Electrovaporization and thermotherapy use direct heat to vaporize the tissue, which is sufficient to vaporize the area in the loop, but also dissipates lesser coagulative temperatures to adjacent tissue. 8 As a result, there is the potential to cause unwanted necrotic damage surrounding the vaporized area. 12 In contrast, GreenLight PVP imparts energy at a wavelength efficiently absorbed by oxyhemoglobin, which is in high concentration in prostatic tissue. 8 Therefore, in principle, heat for vaporization in PVP is more focused for the desired tissue. 15 Despite the low incidence of urethral damage with each modality alone, the combined effects of TURP and GreenLight PVP have not been well described. In both cases presented here, however, stricture occurred after PVP and not other modalities.
Further, a latex allergy was considered as a possible cause of inflammation and stricture in Case 2. It is unlikely, however, that an allergic reaction is the etiologic factor, because nonlatex supplies were used during initial PVP and subsequent procedures. Moreover, skin testing for latex allergy was negative. Another possible explanation for the patients' strictures is mechanical damage from the cystoscope at the time of PVP, which led to necrosis and inflammation. This explanation is unlikely, however, as the three procedures were performed at different hospitals by different surgeons with extensive experience in transurethral surgery. Finally, the extent of the strictures, from the tip of the penis to the internal urethral sphincter, and the contracted bladder in Case 2 indicates damage that is more complex than that which could be attributed to the instrument.
The diffuse nature of the injuries suggests possible electrical or thermal damage. A review of the records, however, revealed no variation in any case from standard practice. Furthermore, the scopes, lasers, and irrigation solutions used in these cases represent standard equipment that has been used in many surgeries without complication. It is especially unfortunate that we do not know why this complication occurred, because we therefore cannot suggest what can be done differently to prevent this from happening in the future.
Conclusion
This case report illustrates a particularly unfortunate and devastating complication after GreenLight Laser PVP. Three men who presented with uncomplicated LUTS and underwent a routine procedure ultimately needed lifelong urinary diversion. We are not concluding that the PVP “caused” the strictures and other damage and are only reporting that these very long strictures developed after PVP. We invite the urologic community to share similar experiences, if any, to identify the incidence of such morbidity, especially cases involving panurethral strictures. Hopefully with more cases identified and examined, the cause of this very devastating complication can be elucidated and thus avoided.
Footnotes
Disclosure Statement
No competing financial interests exist.